A multiphase study on youth suicide in Utah has led researchers to the juvenile justice system, and ultimately, into homes as they work to prevent suicide in at-risk youth.
Douglas Gray, M.D.: “We’re giving the kids and parents what they need to succeed.”
The Utah Youth Suicide study began after concerned psychiatrists and mental health professionals in the Salt Lake City area met in the early 1990s to talk about how to end the epidemic of youth suicides in that state, according to principal investigator Douglas Gray, M.D., an assistant professor of psychiatry at the University of Utah in Salt Lake City.
Gray traveled to the annual meeting of the American Association of Suicidology in Santa Fe, N.M., last April to discuss the latest findings from the study.
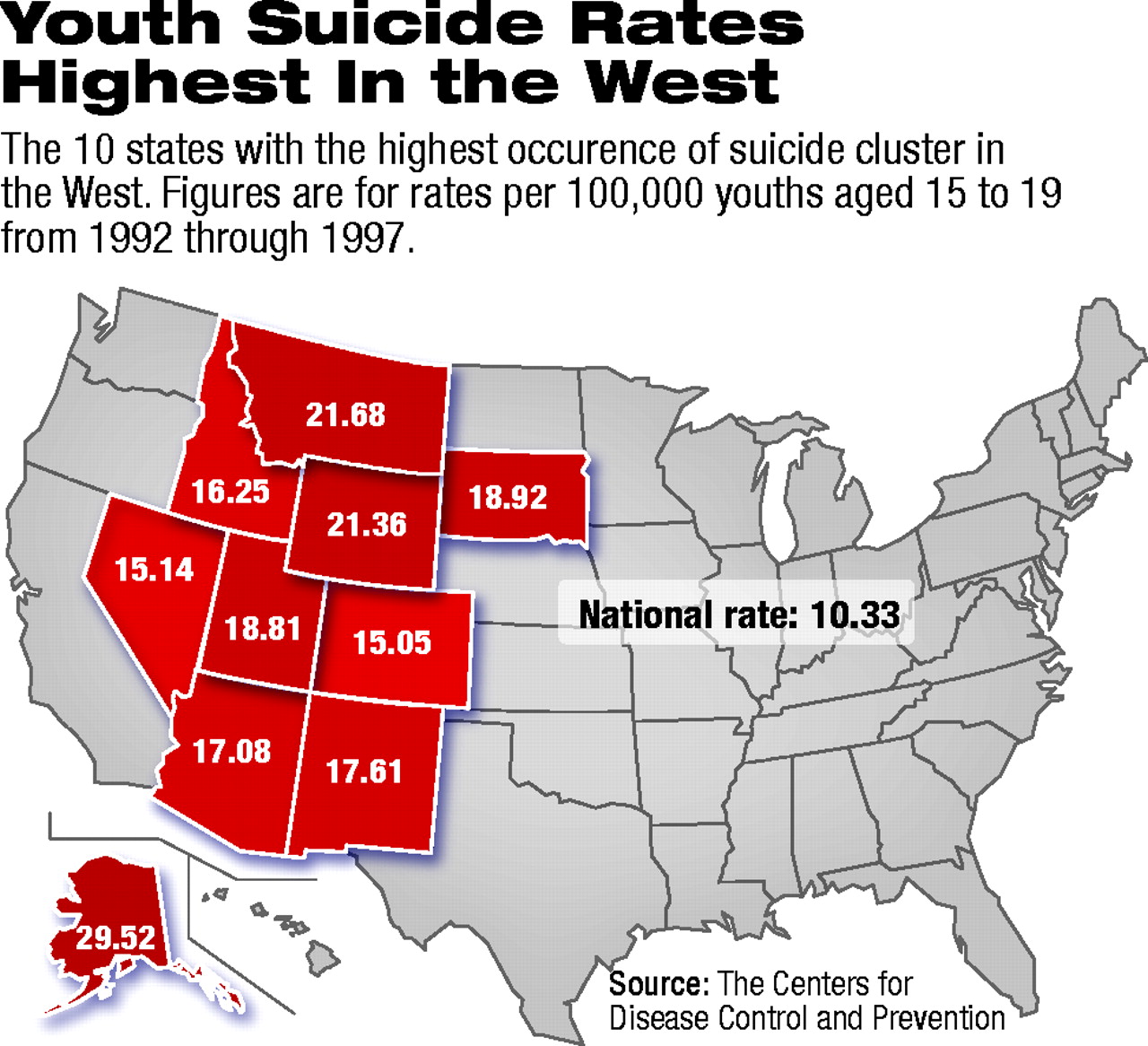
Rocky Mountain States such as Utah had higher rates of youth suicide than other states in the early to mid-1990s (see map below).
The researchers began their quest to learn about the risk factors for youth suicide by examining government agency data for 151 youth aged 13 to 21 who committed suicide in Utah between 1996 and 1999.
Gradually, Gray and his colleagues pieced together information about the youngsters’ lives from statewide databases of the medical examiner’s office, department of human services, and juvenile justice system. The researchers also searched computerized school records.
The data from this initial phase of the study appeared in the April 2002 issue of the Journal of the American Academy of Child and Adolescent Psychiatry.
Falling Through the Cracks
From the medical examiner’s office, Gray learned that 90 percent of the 151 youth who had committed suicide were male, and more than half had used a firearm. Toxicological studies revealed that just 3 percent of the youth had a psychotropic drug in their system at the time of death, yet 24 percent had an illicit drug in their systems when they committed suicide, according to Gray.
Gray and his colleagues were able to obtain school records on 126 of the 151 youth in the sample and found that just 57 percent were enrolled in or had graduated from a school at the time of their death.
Gray explained that some of the youngsters had moved from place to place with their families and had not registered with the school district in their new location.
The researchers also discovered that 63 percent of the 151 youngsters who committed suicide had had previous contact with the juvenile justice system. Of the 95 youth with a juvenile justice record, more than half were charged with truancy or possession of marijuana or alcohol. Aggressive behavior landed a third of the 95 youth in the juvenile justice system, Gray said.
When Gray compared the juvenile justice contacts of the suicide completers with those of all Utah youth of the same age and gender, he found an association between contact with the juvenile justice system and suicide. “We found that the more offenses a youth commits, the greater the risk of suicide,” he said.
Gray characterized the suicide completers with juvenile justice contact as living at home with their parents and committing a number of minor offenses over a period of several years—a time lag that allows for identification and treatment of at-risk youth, Gray pointed out.
Barriers to Treatment
But before they could intervene, the researchers wanted to learn more about the suicide completers. So they went to the people who knew them best—their parents, siblings, and friends. In parent interviews, the researchers learned that 65 percent of the parents identified their son or daughter as having a psychiatric diagnosis. Most had a mood disorder and/or a substance use disorder.
Yet earlier data had shown that just 1 percent were actively receiving public mental health treatment at the time, and just 3 percent were taking a psychotropic medication at the time of death. Gray wondered why the majority of the suicide completers weren’t in treatment.
When asked to identify the barriers to treatment for their children who committed suicide, parents most frequently cited three factors: their children believed nothing could help them, they were reluctant to admit they had problems, and they perceived seeking help as a sign of weakness. Siblings and friends listed the same problems and added one more—the suicide completers did not know where to go for help.
Acting on his discovery that juvenile justice contact may be associated with suicide, Gray set out to learn more about the adolescents who entered the juvenile justice system in Utah.
Along with his colleagues, he administered the Youth Outcome Questionnaire (YOQ) to the parents of 719 youth who entered the juvenile justice system over a one-month period in 1999.
He found that many of the youth had serious mental health problems: 49 percent had YOQ scores indicating the need for outpatient treatment, and 17 percent scored high enough to need inpatient treatment.
From an analysis of the YOQ scores, Gray learned that “the greater the number of offenses, the worse the mental health.”
Last year Gray and his colleagues decided to take what they had learned from the suicide completers and their loved ones and apply it to at-risk youth.
Using the risk factors they pinpointed in their research—repeated contacts with the juvenile justice system and poor mental health as indicated by high YOQ scores—they began a pilot intervention study to prevent youth suicide in the Salt Lake City area. With the close collaboration of the juvenile justice system, the researchers have begun screening and intervening with at-risk youth.
Here’s how it works: the researchers, working from a list of adolescents provided to them by the Third District Juvenile Court in Salt Lake City, match adolescents who have similar YOQ scores and ages, as well as the same number of offenses. A flip of the coin determines who enters the study intervention and who receives treatment as usual in the community.
As part of the intervention, the youth receive a psychiatric evaluation and are treated for any mental health problems at the University of Utah Division of Child and Adolescent Psychiatry outpatient clinic. In addition, a treatment team is assigned to work with each adolescent. “As a team, we also address any educational issues and help the adolescent to function better within the community,” said Gray.
That the adolescent buys into his or her treatment plan is important, but not necessary, he added. “Even if the teen says, ‘I don’t want any more of this,’ we keep working with the family, as long as we have the parents’ cooperation.”
“Our motto is, ‘within 72 hours, we get someone into your home,’ ” Gray said, referring to the other aspect of the intervention, an intensive in-home training program for parents of at-risk youth.
The in-home program is the result of a successful collaboration between the Utah Youth Suicide study and Utah Youth Village Families First in Salt Lake City.
Families of at-risk youth may have trouble setting limits with their children, Gray explained, or can’t manage their behavior at all. While the treatment team is working with the teen and his or her parents to set limits, a Families First staff member enters the home each day—first, to help with the day-to-day family functioning—and then to provide parents with the skills they need to better manage their adolescents.
“They don’t march in and start telling parents what to do,” Gray remarked, referring to the in-home service. “They might help with the dishes or drive the young person to his soccer match—they learn everything they can about how your family works, and then they counsel you about the best way to manage your children.”
So far, there are more than a dozen families participating in the intervention study, according to Gray, and the researchers have received positive feedback from both parents and children. Preliminary data on the intervention will be available next year.
“We provide the kids with rapid access to psychiatric treatment, in-home support, and case management,” said Gray. “We’re giving the kids and parents what they need to succeed.”
More information on the study can be obtained by contacting Michelle Moskos, Ph.D., M.P.H., by e-mail at [email protected]. ▪
Researchers in the University of Utah’s division of child and adolescent psychiatry have joined forces with the state juvenile justice system and a community parent-training program to help reduce the risk of suicide among troubled youngsters.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
To download the citation to this article, select your reference manager software.
There are no citations for this item
View Options
View options
Get Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.