Why are prescription drugs cheaper in Canada than in the United States?
With congressional debate intensifying about the merits of Canadian drug reimportation, health policy analysts are addressing the obvious question (see story above).
At an AARP-sponsored International Forum on Prescription Drug Policy in June, Tom Brogan, president of Brogan Inc.—a Canadian consulting firm that deals with pharmaceutical issues—described the establishment of Canada’s Patented Medicine Prices Review Board (PMPRB) and discussed differences in drug-pricing policies and coverage between Canada and the United States.
Related information is available in “Prescription Drug Prices in Canada” by David Gross, published in June by AARP’s Public Policy Institute and available at www.aarp.org/ppi.
Universal Coverage
Through a program called Medicare financed by the federal and provincial governments, Canada offers universal coverage for acute-care hospital and physician services.
Canada’s Medicare does not provide coverage for outpatient prescription drugs, but the provinces typically provide drug coverage for elderly, disabled, and low-income residents. Public insurance plans in Canada pay for about 44 percent of total prescription-drug spending; private plans cover 34 percent, and patients pay the remaining 22 percent out of pocket.
In 1987 the Canadian government established the PMPRB as part of a package of initiatives to encourage pharmaceutical research and development (R&D).
For 18 years prior to the PMPRB’s establishment, the government encouraged drug-price competition by allowing generics manufacturers to obtain a license and pay a nominal royalty to the patent holder to sell versions of patented drugs.
The package included a law that mandated a seven- or 10-year period of market exclusivity during which generic drugs could not enter the market. Canadian drug manufacturers agreed to double the ratio of R&D to sales in Canada from 1987 to 1996.
Brogan said that before the legislation, the ratio had been between 3.5 percent and 4.5 percent.
The PMPRB was intended to prevent “excessive” increases in patent-drug prices that might result from the manufacturers’ new rights to market exclusivity.
What Does the PMPRB Do?
The PMPRB uses four guidelines in determining whether a drug price is excessive:
• For most new patented drugs, the cost of therapy may not exceed the highest cost of therapy with existing drugs used to treat the same disease in Canada.
• For breakthrough drugs and those that offer a substantial improvement, manufacturers can charge the median of the prices charged for the same drug in countries listed in the PMPRB’s “Regulations.”
• Price increases after a product launch can not exceed the rate of increase in Canada’s Consumer Price Index.
• The price can never exceed the highest price for the drug in the countries listed in the “Regulations.”
The PMPRB can order a company it deems out of compliance with the guidelines to reduce the price and also relinquish double any “excess” revenues it may have received from sales of the drug.
Brogan told the audience, “Overall the system has worked fairly well, partly due to the transparency of the rules.”
The PMPRB likely has brought about some positive changes for Canadian residents, or at least has prevented some negative consequences.
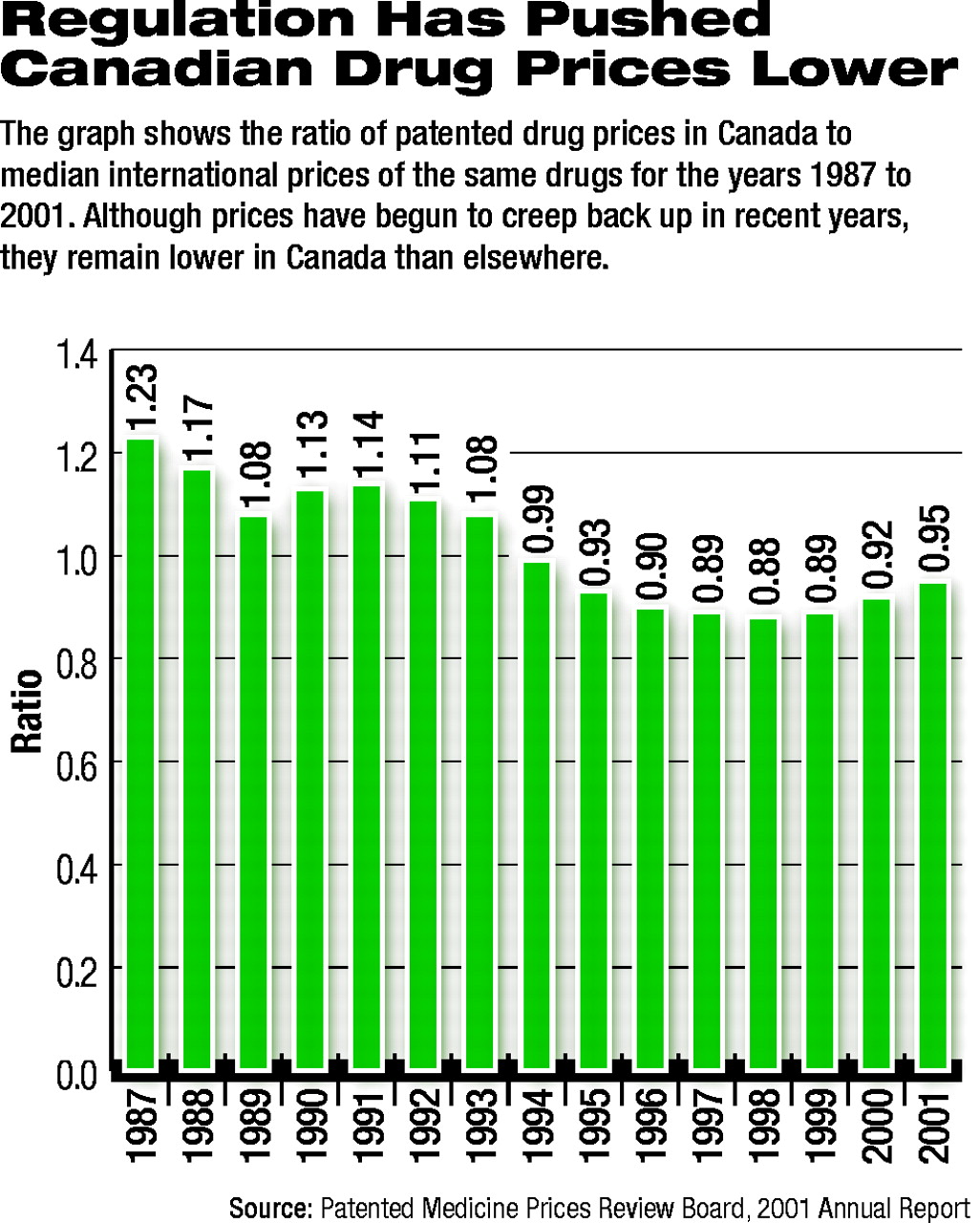
Canadian drug prices have declined in relationship to median international prices for patented drugs (see graph). In 1987, the ratio was 1.23, and in 2001 it was .95.
Gross wrote that Canadian pharmaceutical prices rose faster than U.S. prices prior to 1987, but rose at near zero rates or actually declined each year from 1992 to 2001.
Gerard Anderson and colleagues wrote in the May-June Health Affairs that average annual growth in per capita spending on pharmaceuticals was 4.8 percent in Canada between 1990 and 2000 and 6 percent in the United States between 1990 and 1997.
Brogan told the audience that many provinces have established their own cost-containment measures, so Canadian drug prices are affected by factors other than the PMPRB.
Brogan said, however, that overall pharmaceutical spending is being driven by a demand for new drugs, the number of people using multiple medications, and the aging of the population.
Price controls, such as those exercised by PMPRB, can affect cost, but cannot ultimately contain the growth in expenditures.
The impact of cost-containment measures on R&D is not clear. Canadian drug manufacturers nearly doubled the ratio of R&D spending to sales from 1987 to 1996, as they had promised. The figure went from 6.1 percent of sales in 1988 to 11.7 percent in 1995. However, it then dropped to 9.9 percent in 2001.
By contrast, according to Gross, in 2001 R&D spending by U.S.-based pharmaceutical companies was about 18 percent of sales in 2001.
Pierre Beausejour, M.D., chair of the Board of Directors of the Canadian Psychiatric Association, told Psychiatric News, “Every country is looking at every other country for the magical answer about how to control drug prices.”
He pointed out that inequities in access and other disparities also exist in Canada, because each province sets its own eligibility standards for prescription-drug coverage and determines its own methods for cost containment.
Beausejour noted that investment in R&D declined when pharmaceutical companies were no longer required to maintain a certain percentage of R&D to sales.
An article in the next issue will examine factors that impact the relationship between spending on R&D and drug prices.
A transcript of the AARP forum is posted on the Web at www.kaisernetwork.org/health_cast/hcast_index.cfm?display=detail&hc=882. ▪
Cost-containment measures in Canada show limited success in restraining prescription drug prices, but demand for pharmaceuticals continues to accelerate.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
To download the citation to this article, select your reference manager software.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.