Sertraline (Zoloft) may be an effective and safe treatment for major depressive disorder in children and adolescents. The finding comes from a report of two randomized controlled trials in the August 27 Journal of the American Medical Association.
The report from Karen Dineen Wagner, M.D., Ph.D., a professor of psychiatry and behavioral sciences and director of the division of child and adolescent psychiatry at the University of Texas Medical Branch in Galveston, and from the multinational Sertraline Pediatric Depression Study Group, represents the largest positive medication treatment trial in pediatric depression published to date. Only three other similar clinical trials have been published in peer-reviewed journals, two showing efficacy of fluoxetine (Prozac and generics) and one showing efficacy of paroxetine (Paxil).
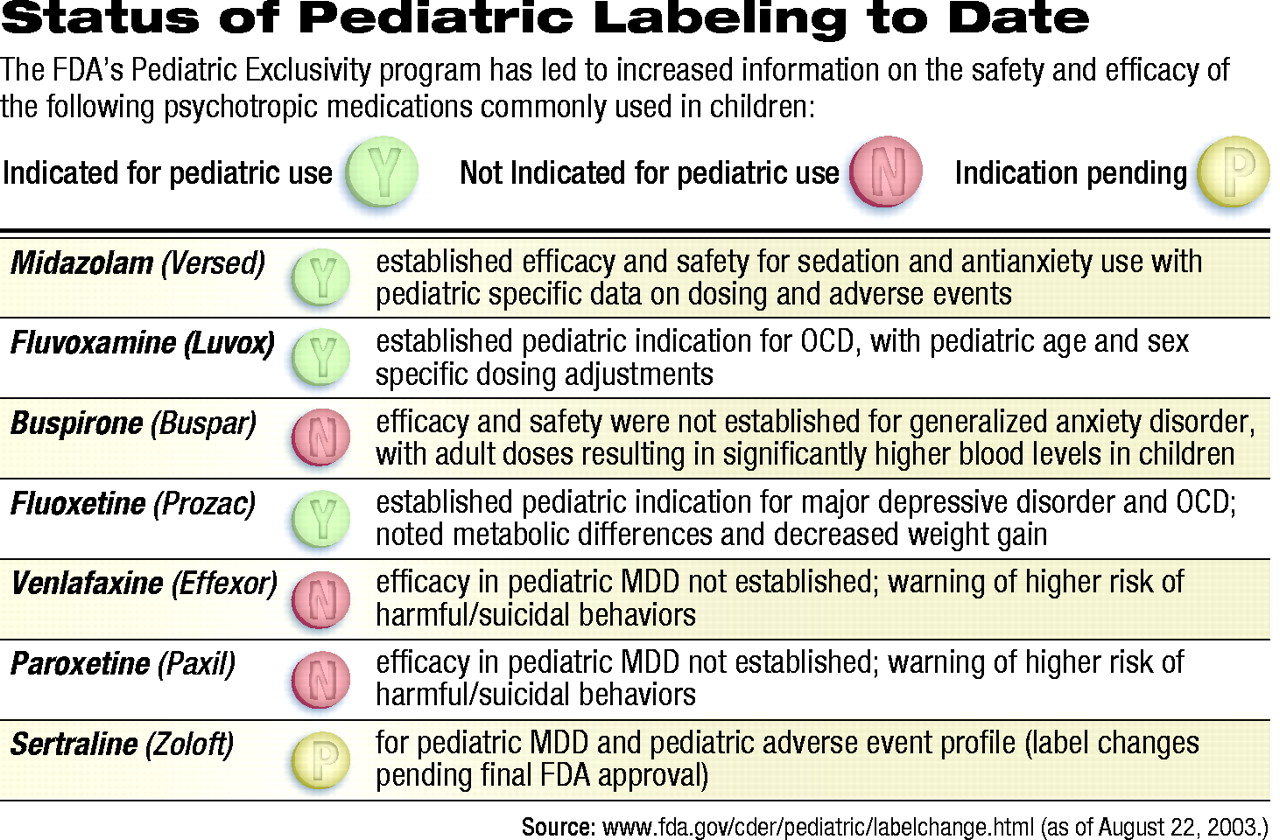
Prozac remains the only antidepressant to carry a pediatric indication approved by the Food and Drug Administration (FDA).
Use of antidepressants in pediatric depression has been controversial for some time, but became more so in June when the FDA, along with the British Medicines Control Agency, issued formal warnings to physicians advising against the use of paroxetine in children and adolescents.
The agencies cited a large data set (pooled from nine clinical trials) submitted by GlaxoSmithKline that revealed not only a lack of efficacy—in the opinion of both agencies— but also a potentially significant increase in harmful behaviors, including suicidal ideations and actions (Psychiatric News, July 18).
More recently, on August 22, Wyeth sent out a “dear health care professional” letter, reminding physicians that its brands of venlafaxine (Effexor and Effexor XR) are not approved for use in children and adolescents. In addition, the company advised it is voluntarily revising labeling for both medications to include a statement that “safety and effectiveness in pediatric patients have not been established” as well as a warning that clinical trials have noted increased reports of “hostility” and “suicidal ideations and self-harm.”
The report by Wagner includes data from two randomized controlled trials in 376 children and adolescents (aged 6 to 17) with DSM-IV-defined major depressive disorder of at least moderate severity.
Funded by Pfizer, the trials were undertaken at the request of the FDA under the provisions of pediatric exclusivity and the Best Pharmaceuticals for Children Act (see related article on page 16). Pfizer acknowledged it has received a letter from the FDA saying the company will “likely be able to add the pediatric safety data” to the Zoloft label; however, it was not clear that the company would receive a pediatric indication for the SSRI.
Study patients were randomly assigned to receive either sertraline (50 mg to 200 mg per day) or placebo for 10 weeks. The main outcome measures were the change from baseline on the Children’s Depression Rating Scale–Revised (CDRS–R) Best Description of Child total score and any reported adverse events.
Patients who received sertraline saw significantly more improvement in their CDRS–R scores than patients taking placebo (30.24 points vs. 25.83 points, respectively, at week 10). With “response” prospectively defined as a 40 percent reduction in the adjusted CDRS–R score by the end of the studies, 69 percent of those taking sertraline were classified as responders, compared with 59 percent of patients taking placebo.
Seventeen patients taking sertraline (9 percent) dropped out of the studies because of adverse events, compared with five patients taking placebo (3 percent). Within the overall study population, adverse events were defined as those that occurred in at least 5 percent of patients taking sertraline and with a rate at least twice that of patients taking placebo. In children (aged 6 to 11), reported events included insomnia (19.8 percent), diarrhea (15.1 percent), anorexia (10.5 percent), vomiting (9.3 percent), agitation (8.1 percent), and urinary incontinence (5.8 percent). Among adolescents (aged 12 to 18) events included vomiting (7.8 percent) and diarrhea (6.8 percent).
Seven patients taking sertraline experienced a serious adverse event (as defined by the FDA) compared with six patients taking placebo. Serious events included suicide attempt (two patients taking sertraline and two taking placebo), suicidal ideation (three sertraline, no placebo), and aggressive reaction (one sertraline, no placebo).
Patients taking sertraline lost an average of 0.8 pounds through the 10-week studies, compared with a gain of 1.7 pounds for patients taking placebo.
Clinical Significance
Wagner and her colleagues note that “the significance of the results is clinically as well as statistically relevant.”
With only three previous studies showing any benefit of SSRIs for pediatric depression, and no studies showing a benefit for tricyclic antidepressants, the current study’s treatment effect is “modest in comparison with that typically observed in adult studies,” according to the authors.
But in pediatrics, only one study—with fluoxetine—has shown a more robust effect with an antidepressant. That study, however, involved a significantly smaller group of children and adolescents.
Wagner and colleagues believe that one problem is the large placebo effect often seen in children. “Data suggest that the placebo response rate is at least as high in [the pediatric] age population [as it is in adults],” the authors noted. “Increased visit frequency and the attention associated with these visits may have an intrinsic component of therapy and is different from a ‘waiting period’ control, in which there is no interaction.”
Studies Should Be Expanded
The authors noted that while this study suggested that sertraline was slightly more effective, as well as more tolerable, in adolescents than in children, further studies need to be completed to determine whether that is true in the general population. They also noted that discontinuation of sertraline was not associated in these studies with a “withdrawal syndrome” like that often observed in patients taking paroxetine and venlafaxine.
“Nonetheless,” the authors concluded, “the results reported here support the conclusion that sertraline is an effective, safe, and well-tolerated short-term treatment.”
Amid recent controversy surrounding the use of antidepressants in children, two clinical trials suggest that sertraline may be an effective treatment option.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.