A committee charged by the New Mexico state legislature with developing recommendations for state regulations governing psychologist prescribing has issued its report.
The report, containing the group’s final recommendations, was written by a joint committee of physicians appointed by the New Mexico Medical Board and psychologists appointed by the New Mexico Board of Psychologist Examiners.
Although the report signals a significant step forward in the process of implementing the nation’s only psychologist prescribing law (Psychiatric News, April 5, 2002), it contains sets of both majority and minority recommendations, suggesting just how far regulators may still need to go to reach a final set of rules.
The legislation, signed by former New Mexico Gov. Gary Johnson on March 5, 2002, went into effect on July 1 of last year.
The law (HB 170) charged the two state boards with hammering out the nuts and bolts of implementing the controversial legislation. Pending the final recommendations of the joint committee, progress reports were to be filed on December 1, 2002 and 2003, advising the governor and legislature “on the progress made and any problems encountered in implementing the provisions of this act.”
The committee’s work was indeed complex and involved key issues including the defining of a curriculum for programs aimed at teaching psychologists to prescribe, the details of how the two stages of clinical practicums would be formally supervised, designation of a national certification exam, adoption of a list of drugs that psychologists would be permitted to prescribe, and potential limitations on prescribing to special populations.
The report noted that while representatives of the psychology and medical boards appointed to the committee made “every effort. . .to arrive at a consensus in all decisions,” it acknowledged that a “thoughtful minority opinion is included in the final report.”
The joint committee was co-chaired by psychologist Timothy Strongin, Ph.D., and Albert V. Vogel, M.D., associate dean emeritus for clinical affairs and a professor of psychiatry at the University of New Mexico School of Medicine and APA Area 7 Trustee.
The Psychiatric Medical Association of New Mexico (PMANM) supports the report’s minority opinion and recommendations, which were developed by Robert Bailey, M.D., head of child psychiatry and chief of staff at the University of New Mexico’s hospital.
The state of New Mexico, the minority opinion began, “is about to conduct an experiment—an experiment never before attempted to determine whether psychologists with minimal additional training can safely, competently, and independently prescribe.”
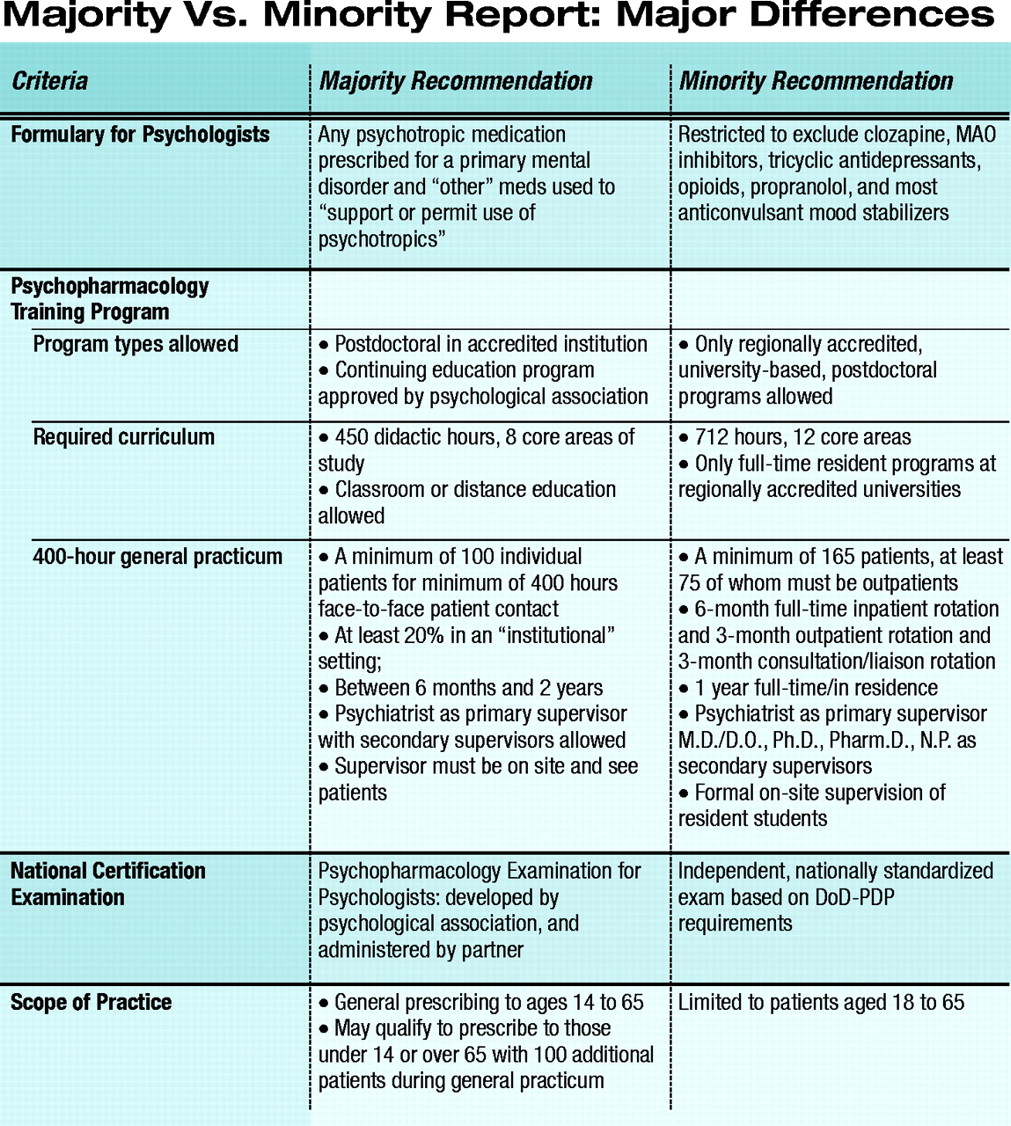
Source: Final Report of the Joint Committee for HB170: Prescriptive Authority to Psychologists Act of 2002; New Mexico Board of Psychologist Examiners and New Mexico Medical Board; September 19, 2003According to the minority report, the majority recommendations, while adhering to the minimum letter of the law, are vague and contain numerous areas of concern, including few restrictions on the formulary psychologists would be permitted to prescribe, how psychologists will be trained, what national certifying exam should be designated by the state, and limitations on psychologists’ prescribing scope of practice (see chart).
The minority recommendations fault the majority for “ignoring” the “only substantial test of psychologist prescribing” to date, the Department of Defense Psychopharmacology Demonstration Project (DoD-PDP), conducted between 1991 and 1997.
That program consisted of one year of intense classroom training and one year of supervised clinical experience in inpatient, outpatient, and consultation-liaison rotations.
“Despite a much longer and far more intensive training program than that being proposed by the committee majority,” the minority report states, “the DoD-PDP psychologists achieved knowledge comparable to that of a third- or fourth-year medical student,” a conclusion drawn by an independent review of the DoD-PDP program by the American College of Neuropsychopharmacology (ACNP) in 1998.
Also, the majority recommendations appear largely to exclude psychiatric expertise in the process of readying psychologists to prescribe, according to the minority opinion, despite the fact that “psychiatrists are currently the largest national source of psychopharmacologic expertise” and the source of “the majority of clinical wisdom regarding psychotropic medications.”
Also excluded from the processes of developing a curriculum, admissions criteria, standards for supervision of the clinical and general practicums, and the designation of a national certifying examination were nurse practitioners, physician assistants, and clinical pharmacists, all of whom already have prescribing authority in New Mexico.
Points of Contention
The minority opinion concluded that rather than basing the committee’s recommendations on a sound evidence base—including the DoD-PDP experience, the ACNP’s independent review of that program, and the experience of practicing psychopharmacologists, as well as existing nonphysician health care providers with prescriptive authority—the majority recommendations give “far too much weight to the guidelines promoted by the American Psychological Association.”
The majority recommendations call for psychopharmacology training programs that are based on a continuing education (CE) model—but only CE programs accredited by the American Psychological Association.
The minority opinion, however, points out that “psychologist training does not include sufficient education in medical subjects such as physiology, pathology, pharmacology, physical examination, or clinical and laboratory assessment; in other words, education for psychologist prescribing cannot be continuing education because there is nothing to continue from.”
The minority opinion also notes that by allowing CE-modeled programs, the majority recommendations make “no explicit requirement for face-to-face assessment during didactic programs.”
The minority recommendations favor a much more stringent model program, based upon the DoD-PDP, based in regionally accredited university settings where students study full time, in residence. The minority-favored program is nearly twice as long (712 hours in 12 core areas, compared with 450 hours in eight core areas), and involves much more intense clinical practicums.
Besides relying on the psychological association’s guidelines for curriculum development and content, the majority recommendations favor the Psychopharmacology Examination for Psychologists, developed by the psychological association, as the national certifying exam required by the law. In addition, the recommendations would allow the psychological association to designate the passing score for the exam and potentially change that score in the future without consultation with state regulators.
The minority calls for a nationally standardized exam developed by an independent, interdisciplinary team to include, in time, prescribing psychologists as the pool of certified practitioners grows.
Safe Scope of Practice?
The minority opinion would limit prescribing psychologists to treating only adult patients aged 18 to 65. The majority recommendations would allow candidates to prescribe to patients aged 14 to 65, and they could qualify to prescribe to patients under the age of 14 or over the age of 65 by prescribing to an additional 100 child and adolescent or geriatric patients during their practicum. This, the minority opinion concluded, “is unconscionable.”
In addition, the minority recommendations would significantly limit the formulary of medications available for prescribing by psychologists. Of particular note, no anticonvulsant mood stabilizers would be allowed to be prescribed. The minority noted that the law expressly prohibits psychologists from treating patients for nonpsychiatric medical disorders.
How, the minority ask, could a psychologist “prescribe valproate to a patient with bipolar disorder and partial complex seizures without violating [that clause of the law] or (intended or not) becoming involved in the treatment of primary somatic conditions?”
Lastly, but perhaps most importantly, the majority recommendations would seemingly allow a psychologist to prescribe a psychotropic medication to a patient against the advice of his or her medical doctor. The recommendations state “the primary health care practitioner and the prescribing psychologist do not need to agree about a particular treatment strategy.” If this occurs, the psychologist would be required only to document why he or she adopted a treatment strategy not agreed to by the primary care provider.
Noting that this would be “contrary to established medical practice, and dangerous,” the minority would give the medical provider’s judgment precedence over that of the prescribing psychologist.
Next Steps
The joint committee’s report has been forwarded to each of the full boards for consideration. The psychology board is designated to issue its full response first—it could adopt the majority recommendations or modify them with any of the minority opinions.
Following the psychology board’s action, the medical board will decide what it will do with the report. At some point the two boards must reconcile discrepancies and forward the recommendations to the governor and the legislature.
After a required public comment period, a rules hearing must be held.
At press time, both boards were expected to consider final approval of the recommendations sometime this month, with a rules hearing to occur in time to target formal implementation of the regulations soon after the first of the year.
The report is posted on the Web at www.nmpsych.org/report_hb_170.htm. ▪
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.