Congress approved an historic and controversial new Medicare reform package intended to modernize the 38-year-old entitlement program and contain costs by making it more competitive, while offering for the first time a benefit providing coverage for prescription drugs.
After weeks of speculation about whether the hotly contested legislation would emerge at all, a House-Senate conference committee forged an agreement just a week before the Thanksgiving recess, followed in rapid succession by House and Senate approval. President Bush signed the legislation in early December.
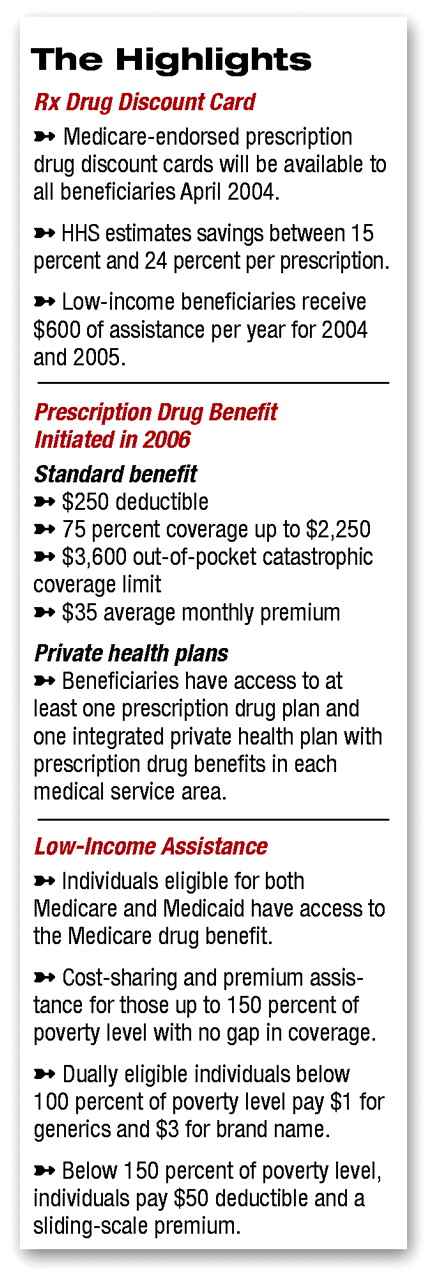
The legislation initiates a drug benefit for Medicare beneficiaries in 2006. The agreement provides protections for low-income individuals, including coverage of those eligible for both Medicare and Medicaid—a category encompassing many psychiatric patients.
The bill does not include mention of psychotropic drugs, but APA and the National Alliance for the Mentally Ill were successful in persuading legislators to include nonbinding “report” language—provisions in the explanatory report that accompanies the legislation—protecting beneficiary access to psychotropic medications. These include but are not limited to those used to treat specific mental illnesses such as schizophrenia, attention-deficit/hyperactivity disorder, bipolar disorder, and depression.
The bill also blocks a scheduled decrease of 4.5 percent in physician payment for 2004, replacing it with a 1.5 percent increase and providing another 1.5 percent increase in 2005. APA, along with the American Medical Association and more than 100 other national medical specialty societies and state medical societies, strongly lobbied for the change.
APA also lobbied for ending the program’s historic 50 percent coinsurance for outpatient psychiatric services. While that provision remains in effect, APA secured a letter from more than 40 members of the House of Representatives in support of phasing out the discriminatory copay, according to APA’s Division of Government Relations.
The conference agreement received the endorsement of the AARP. “This bill will help millions of people, especially those with low incomes and high drug costs,” the AARP stated. “It will strengthen Medicare by adding this long-overdue benefit and preserving the basic structure of the Medicare program.”
Yet the bill has also been the subject of heated criticism—that it adds layers of complexity to the program with little guidance for beneficiaries on how to navigate the new benefits, that the actual benefits will be far less substantial than many beneficiaries expect and need, and that privatization of the program will disrupt the universality of costs and benefits that has been the hallmark of Medicare.
Also controversial is a provision in the law that allows importation of prescription drugs from Canada—and from nowhere else—but with the caveat that imported drugs must be certified as safe by the secretary of Health and Human Services.
The safety certification is considered “the poison pill” of the provision, because no HHS secretary—including current secretary Tommy Thompson—is likely to commit to guaranteeing safety of imported drugs. The provision is considered a windfall for the pharmaceutical industry, which has opposed importation of price-controlled drugs.
Now, as in the past, the Food and Drug Administration will likely continue to look the other way when individuals import small amounts of prescription drugs, but pharmacies and managed care organizations will be unable to import large quantities.
“The reality is that [the safety certification] will never happen because the secretary is never going to guarantee safety,” said Bryan Anderson, press secretary to Rep. Gil Gutknecht (R-Minn.). Anderson told Psychiatric News that the Medicare reform law is actually more restrictive than a previous law that allows for importation of drugs from 25 industrialized countries with HHS certification of safety.
Gutknecht was sponsor of the Pharmaceutical Market Access Act of 2003 (HR 2427), which would allow importation of drugs from 25 industrialized countries—to take advantage of price controls in Europe and elsewhere—without the requirement of safety certification by the HHS secretary. That bill passed the House with bipartisan support.
Within hours of the 54-44 Senate vote on the Medicare reform bill, Senate Democratic leader Tom Daschle introduced legislation to repeal several of the bill’s most controversial provisions and to allow the importation of lower-priced prescription drugs from Canada and Western Europe.
“This debate is not over; it’s just beginning,” said the South Dakota Democrat.
APA Medical Director James H. Scully Jr., M.D., told Psychiatric News that while APA had supported some of the Medicare bill’s provisions and opposed others in accordance with APA policy, the Association took no position on the overall package. He underscored the bill’s complex nature and still-to-be-determined ramifications.
“While the sweeping changes in Medicare embodied in the bill are inevitably controversial, and even supporters concede the bill is far from perfect, passage was strongly supported by the AMA and a large coalition of health organizations, including many specialty societies, together with patient groups such as AARP,” Scully said in a member update posted on APA’s Web site.
APA’s Division of Government Relations will provide detailed analysis of the legislation in the coming weeks.
The AMA hailed passage of the Medicare reform bill. AMA President Donald J. Palmisano, M.D., called the vote “an important victory for Medicare patients and their physicians” and said seniors and other beneficiaries had much to cheer about.
“Seniors will receive a long-overdue prescription drug benefit, and the neediest of Medicare’s patients will have no premium or deductible as well as access to medications at little cost,” Palmisano said. “This historic legislation enhances patients’ continued access to care by halting physician payment cuts. The House vote provides a 1.5 percent increase in payment for the next two years. For next year, this is a 6 percent turnaround at a time when physician practice costs are on the rise.”
He added, “Patients also will benefit from a comprehensive package to strengthen health care in rural and underserved areas. This plan will reduce payment disparities in parts of the country where physician services are in great need and short supply.” ▪
