A significant amount of research indicates that ethnic minorities are less likely to receive many effective, new, or high-cost health technologies, including prescription medications. This research includes small data sets examining the use of newer and more-expensive atypical antipsychotic drugs, which show that both Hispanic Americans and African Americans have been much less likely to receive prescriptions for the newer, costlier agents compared with European Americans.
A new study released last month by Johns Hopkins Bloomberg School of Public Health researchers shows that the gap has closed between Americans of Hispanic and European descent. And while Americans of African descent have made significant gains in prescription parity, there is still a troublesome gap.
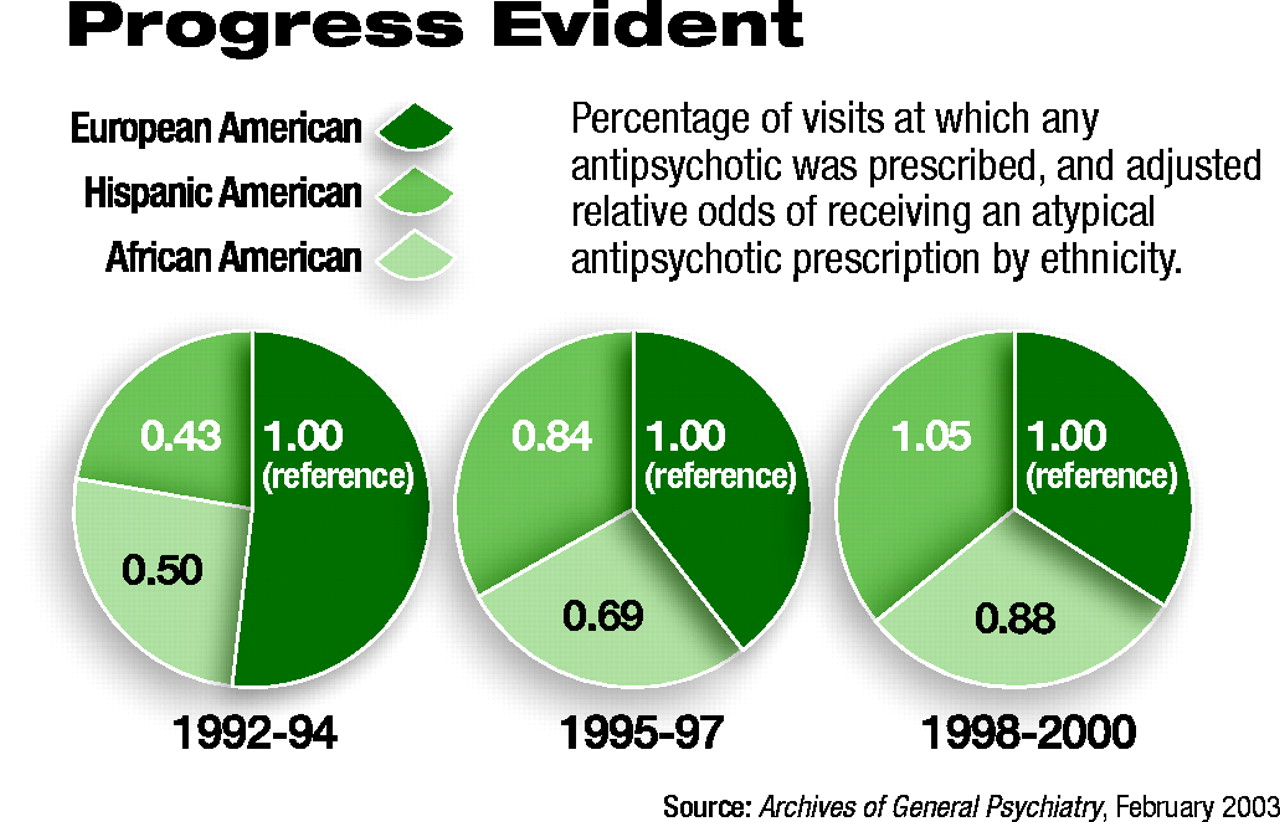
“I think the take-home message here,” lead author Gail L. Daumit, M.D., assistant professor of medicine and health policy management at Hopkins’ Welch Center of Prevention, Epidemiology and Clinical Research, told Psychiatric News, is that compared with white Americans, African Americans were half as likely, and Hispanic Americans about 40 percent as likely, to have been prescribed an atypical antipsychotic for diagnoses made from 1992 to 1994.
By 1997, the odds had begun to improve for both minority groups, and by 2000, Hispanic Americans were just as likely, and African Americans about 84 percent as likely, to get these newer drugs compared with white Americans.
“I think this strongly supports or confirms that the initial ethnic gap or disparity [in prescribing of atypical antipsychotics] had essentially closed for Hispanics and nearly closed for African Americans by the close of the decade,” Daumit said.
Largest Data Set Used
While previous research had hinted at the racial and ethnic disparity in prescribing atypical antipsychotics, the sample sizes of data sets were small, limiting the generalizability of their conclusions.
Daumit and her colleagues in the department of psychiatry and behavioral sciences at Johns Hopkins used data from two large, national surveys: the National Ambulatory Medical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS), both conducted by the National Center for Health Statistics at the Centers for Disease Control and Prevention.
“These two surveys are important for people with severe mental illness, because so many of them are likely to be found in urban areas and be seen at tertiary-care centers—at least we think so,” Daumit said.
The combined surveys include visits to private offices, freestanding clinics, community health centers, local government clinics, health maintenance organizations, and hospital outpatient departments. Excluded from the samples are visits to federally employed physicians and institutional settings, such as the Veterans Health Administration.
For the NAMCS, visit information is recorded by physicians for all patient contacts during one randomly assigned week of the year. For the NHAMCS, visits are recorded for four weeks. Basic patient sociodemographic data as well as diagnosis and treatment information are collected.
Daumit’s group looked only at physician visits during which an atypical antipsychotic medication was prescribed. Study medications included the atypicals clozapine, risperidone, olanzapine, and quetiapine.
From 1992 to 2000, 5,032 visits were recorded at which an atypical was prescribed. White patients accounted for 68.9 percent of visits, followed by African Americans at 20.6 percent, and Hispanic Americans with 10.5 percent of visits.
Diagnostic Differences
The most common diagnosis recorded was a psychotic disorder, with African Americans and Hispanics having a higher percentage of visits in this category than whites.
Daumit said that while other studies have suggested that there is no difference in the prevalence of psychotic disorders between the three racial/ethnic groups, “historically, in the clinical setting, African Americans have been significantly more likely to be diagnosed with a psychotic disorder than European Americans. Whites have been more likely to get an affective disorder diagnosis.”
With that in mind, Daumit said, “I tried to argue that it makes it all the more important to look at all diagnoses together in our data. Given the issue of variable safety of antipsychotics between these groups, it brings up some interesting questions.”
African Americans, for example, are thought to be more susceptible to tardive dyskinesia, favoring the prescription of an atypical drug over a typical, older neuroleptic, Daumit noted. However, they are also potentially more susceptible to changes in glucose and lipid metabolism that have been associated with certain atypical antipsychotics, she said.
“So the issue is,” Daumit asked, “what really is going on in the mental health practitioner’s mind in terms of the tradeoffs between those factors?” A notable limitation of the study, she acknowledged, was that the researchers were not able to separate out the individual drugs to see whether any prescribing patterns were notable within the atypicals themselves.
Also confounding the results, she said, was their inability to account for different routes of administration of medications. Several studies have indicated that African Americans are more likely to receive depot—that is, long-acting—forms of antipsychotics. If so, she said, then they would receive fewer prescriptions for antipsychotics over the course of their physician visits, potentially skewing the data and partially accounting for the remaining gap evident at the end of their study in 2000.
Daumit added that further studies need to take these variables into account and to look at patient preferences. It is possible, she suggested, that some of the remaining gap may be tied to individuals’ preferences for remaining on an older, typical antipsychotic that they are satisfied with.
“Clearly, more research needs to be done in this area; however, what we do have is at least encouraging,” Daumit concluded.
When it comes to atypical antipsychotics, prescribing-pattern disparities between Hispanic and European Americans have largely disappeared. The same cannot be said about African Americans.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.