In 1996, through PL 104-262, Congress mandated that the Department of Veterans Affairs (VA) maintain its capacity to provide for the specialized treatment and rehabilitative needs of disabled veterans.
The legislation came about because the VA was moving to a capitation model of distributing funds throughout its health care system. Advocates and others were concerned that veterans with costly illnesses and disabilities might be shortchanged because of the cost advantage in treating other kinds of patients.
Each year since then, the Committee on the Care of the Seriously Mentally Ill (SMI committee), which Congress mandated to monitor and advise on the care of the groups specified in the legislation, and the VA have disagreed about whether the VA has maintained capacity for veterans with serious mental illness (Psychiatric News, February 7).
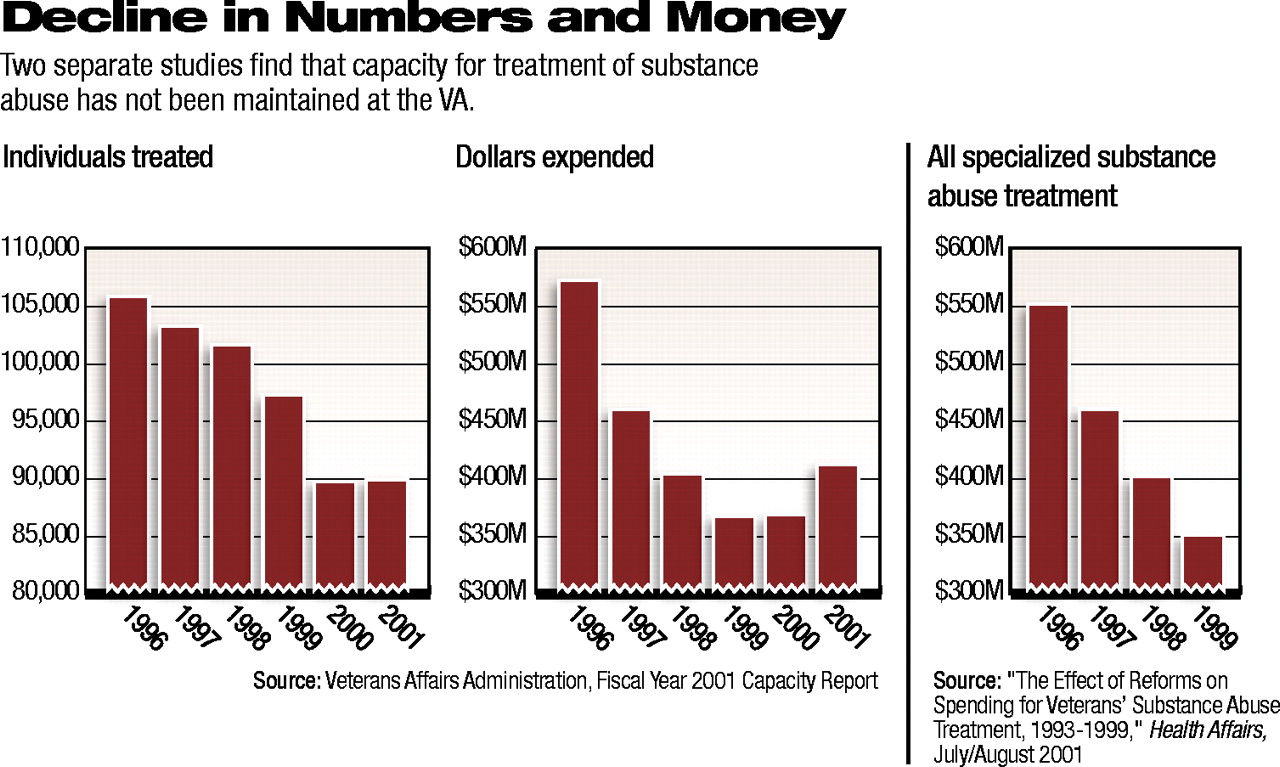
Both the committee and the VA agree, however, that capacity for substance abuse treatment has not been maintained.
Data found in the FY 2001 Capacity Report (released October 2002) show a decline in the number of individuals treated for substance abuse and in the dollars spent (see charts).
In “The Effect of Reforms on Spending for Veterans’ Substance Abuse Treatment, 1993-1999,” in the July/August 2001 Health Affairs, Shuo Chen, Todd Wagner, and Paul Barnett examined the effect of these trends.
The authors are, respectively, research associate at the Health Economics Resource Center (HERC), Veterans Affairs Palo Alto Health Care System; health economist at HERC; and director of the HERC.
The authors noted that the VA, which provides health care to more than 3 million veterans, is the nation’s largest provider of substance abuse treatment.
They claimed that “spending for VA substance abuse treatment declined precipitously from 1993 to 1999.” Their figures, while somewhat different from those in the capacity report, also show a decline. And, they noted, “While total spending for VA health services rose 10 percent between 1993 and 1999, the amount spent on substance abuse treatment declined by 41 percent.”
The most dramatic change, however, was similar to that which took place in the mental health system as a whole during the same period.
Chen and colleagues wrote, “The VA sought to expand the number of veterans served by 20 percent and to decrease the average per-patient expenditures by 30 percent [over a five-year period].”
Managed care was to bring about the transformation. According to information in the August 2002 Psychiatric Services, “By October 2000, inpatient substance abuse treatment beds were almost eliminated at VA facilities. The number of residential beds more than doubled from 1994 to 2000, but this increase was not enough to fully offset the 91 percent decrease in inpatient substance abuse beds.”
The net result of the two trends, according to the authors, is a system that is about half the size of the former system and that has moved from relying primarily on medical inpatient beds to relying almost exclusively on lower-cost residential beds in nonmedical settings.
Opinions vary about the results and implications of these changes. Chen and colleagues wrote that although the number of patients who received specialized substance abuse treatment changed little between 1993 and 1999, they accounted for a “dwindling proportion of all VA patients,” since the total number of persons receiving health care in the VA increased greatly, from 2.7 million in 1993 to 3.4 million in 1999.
Larry Lehman, M.D., chief consultant for mental health services at the VA, agreed that the number of patients receiving specialized care for substance abuse has not kept pace with the increase in the number of veterans receiving care. He added, however, that the recent “surge” in patients was accounted for by those in priority groups 7 and 8, who, for the most part, do not use VA substance abuse care.
He also told Psychiatric News that the capacity report summarizes only those expenditures for substance abuse patients treated in specialized substance abuse programs who meet the criteria for “serious mental illness.” According to Lehman, “Expenditures for the treatment of all substance abuse patients, whether in specialized programs or not, has not gone down. Almost all acute inpatient care for substance abuse patients takes place in nonspecialized settings.”
According to Chen, there is evidence that patients entering specialized VA substance abuse programs are “sicker than ever.” Between 1990 and 1997, the proportion of people in those programs with a comorbid psychiatric diagnosis increased from 29 percent to 40 percent.
Lehman responded to Psychiatric News that the increase could also represent a “significant improvement in diagnostic accuracy.” From 1989 to 1995, the VA undertook an initiative to diagnose and treat comorbid disorders.
Finally, according to the August 2002 Psychiatric Services, “the proportion of substance abuse treatment programs that had patients on waiting lists rose from 68 percent to 75 percent for inpatient programs and from 58 percent to 80 percent for residential programs.”
Former APA President Joseph T. English, M.D., testified before the House Appropriations Subcommittee on VA-HUD and Independent Agencies on VA appropriations for Fiscal 2004 (see article).
English also urged continuation of the VA Substance Abuse Fellowship Program as a means of ensuring a well-trained professional workforce that can implement new treatment knowledge. ▪
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.