The lowest-income group of Medicare beneficiaries without any coverage for prescription drugs could save an average of 17.4 percent over their current out-of-pocket spending when the new prescription-drug discount card program begins next year.
But savings that individual beneficiaries will reap from the program—which will be in effect until the new Medicare-sponsored prescription coverage begins in 2006—will vary considerably, according to a study in the April Health Affairs.
Study author Juliette Cubanski said the study was an attempt to bring precision to savings estimates that have been predicted by the government and others.
What the study also demonstrates, however, is the high degree of uncertainty that surrounds such estimates—both for individuals and for the program as a whole.
“We attempted to be as specific as possible in our estimates and to present different scenarios for average out-of-pocket spending for subgroups of beneficiaries,” Cubanski told Psychiatric News. “But as this program moves forward, there are a number of factors that will vary from one beneficiary to another that will influence how much they will actually save as individuals.
“It will depend on how many drugs they use, how often, and whether they use generic versus brand-name drugs,” she said. “The bottom line is that there is real uncertainty, not just in the aggregate but for individuals. Individual beneficiaries will want to do a careful analysis of their own situation.”
Cubanski is a doctoral candidate in the Program in Health Policy at Harvard University and a researcher in the department of health care policy at Harvard Medical School.
Psychiatric Drug Savings Estimated
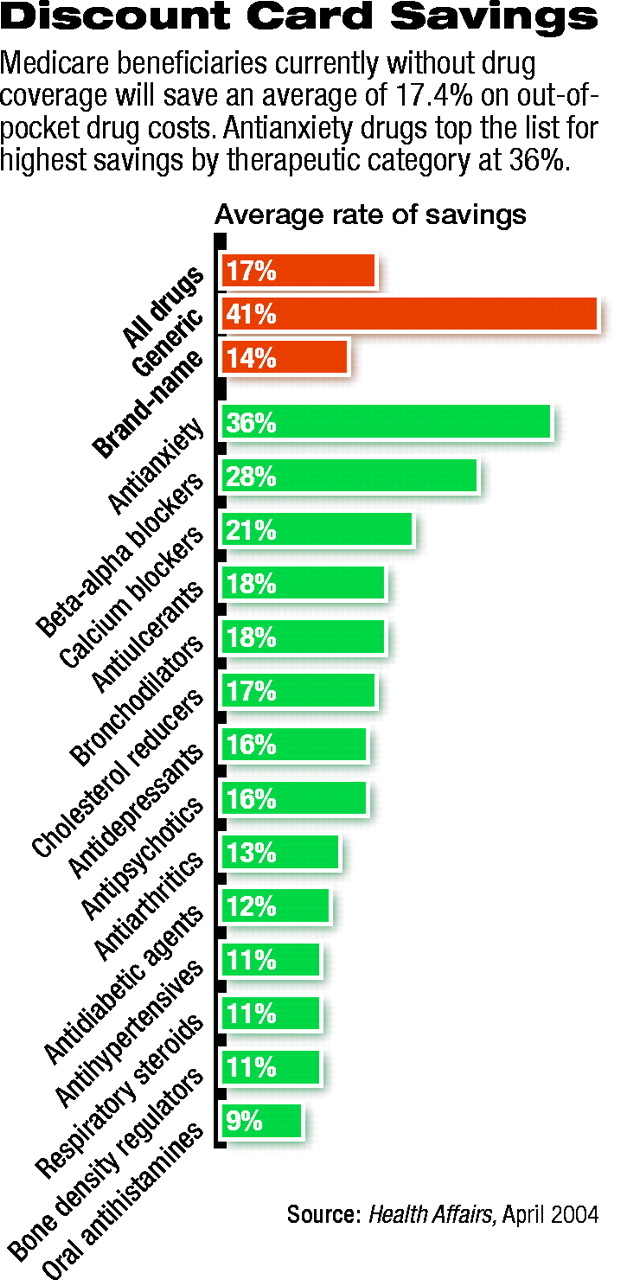
Cubanski and colleagues also estimated percentage savings for beneficiaries currently without any coverage for a number of therapeutic drug categories, including antidepressants and antipsychotics.
Beneficiaries using both of those categories of drugs are estimated to have an average rate of savings of 16 percent over current out-of-pocket costs (see chart).
Analysis included only noninstitutionalized beneficiaries who reported no prescription drug coverage for calendar year 2000. Other categories included beta/alpha blockers and antianxiety medications, calcium blockers and antiulcerants, bronchodilators and cholesterol reducers, antiarthritics and oral diabetes medications, antihypertensives and respiratory steroids, and bone-density regulators and oral antihistamines.
Cubanski cautioned that the range of therapeutic categories considered was narrow and that estimates are subject to multiple variables.
Study co-author Richard Frank, Ph.D., has done extensive health services and economics research on issues affecting patients with mental illness, and Cubanski said they hope to look in a more rigorous way at the implications of the new Medicare reform bill for that category of beneficiaries.
Poorest to See Greatest Benefit
So what can be said with any reasonable certainty about the new discount drug card program?
Clearly, the poorest beneficiaries stand to save money. Those with incomes under $10,000 a year and no current coverage will reap an average savings of 1.8 percent of income, compared with 0.2 percent of income for those earning $40,000 or more.
The poorest beneficiaries will be especially helped by an annual $600 subsidy that isn’t included in the savings estimates, Cubanski said.
Overall, beneficiaries without current prescription coverage are estimated to save about $117. Of that, savings on generic drugs will be higher (41 percent) than on brand-name drugs (14 percent), but brand-name drugs will account for a bigger share of the total savings ($83 of the total $117 in savings).
Aggregate savings from the prescription discount card program are especially difficult to predict in light of uncertainty about the size of the discounts and program participation rates, Cubanski said.
If the lowest estimates of overall discounts and enrollment are used, beneficiaries will see only $74 million in savings. Under alternative assumptions, savings of $1 billion could be achieved if 75 percent of noncovered seniors enroll and receive an average discount of 23 percent.
“The wide range in these numbers indicates that any single estimate of the potential economic impact of the Medicare-approved discount card program is subject to substantial uncertainty, even after actual program enrollment figures are known,” Cubanski said.
In the study, Cubanski and colleagues estimated savings for beneficiaries from discount cards in three stages. First, they estimated average discounts for each of 61 high-volume prescription drugs (49 brand name, 12 generic) offered by seven existing discount prescription card programs. Average discounts were calculated for each drug by comparing the average of the seven card-program prices with average retail price estimates for people paying cash for each of the drugs.
In the second stage, the authors analyzed prescription-drug spending and use patterns reported by Medicare beneficiaries without drug coverage, based on calendar year 2000 data from the Medicare Current Beneficiary Survey Cost and Use file.
Finally, expected out-of-pocket savings were estimated by comparing the estimated average discount rate for each drug with data on out-of-pocket spending. These were extrapolated to estimate individual and aggregate savings on all drugs by all Medicare beneficiaries currently without drug coverage.
Cubanski said physicians can encourage patients to use the discount card programs, but should not overstate their expected savings.
“We found that the savings from the discount card program are modest,” she said. “Certainly, saving something is better than nothing, and to that extent doctors may have a role in encouraging their patients to seek out support from the discount card program as one avenue of paying for prescriptions they need.” ▪
Under the first phase of the new Medicare prescription drug benefit, beneficiaries taking antidepressants or antipsychotics should save an average of 16 percent over current out-of-pocket costs.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
To download the citation to this article, select your reference manager software.
There are no citations for this item
View Options
View options
Get Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.