APA continued its campaign for strong patient protections that allow open access to medically necessary psychotropic medications in the new Medicare Part D drug benefit with testimony last month before the Senate's Special Committee on Aging.
If the Centers for Medicare and Medicaid Services (CMS) fails to adopt“ a common-sense continuity of care approach” to assisting low-income and disabled elderly individuals through the mandated transition from Medicaid drug coverage to the Medicare Part D benefit, “the clinical consequences for the individual are serious indeed,” testified Carl Clark, M.D., chief executive officer of the Mental Health Center of Denver and an assistant professor of psychiatry at the University of Colorado School of Medicine.
Clark testified on behalf of APA, the American Association for Geriatric Psychiatry, the National Association of State Mental Health Program Directors, and several other consumer and professional groups concerned with mental health care.
The focus of the March 3 hearing was made clear at the outset by Sen. Gordon Smith (R-Ore.), chair of the Committee on Aging. “I strongly believe that our ability to transition the 6.4 million Americans who are the poorest and most vulnerable citizens in the Medicare/Medicaid system will ultimately prove the overall success or failure of this new program,” Smith said.
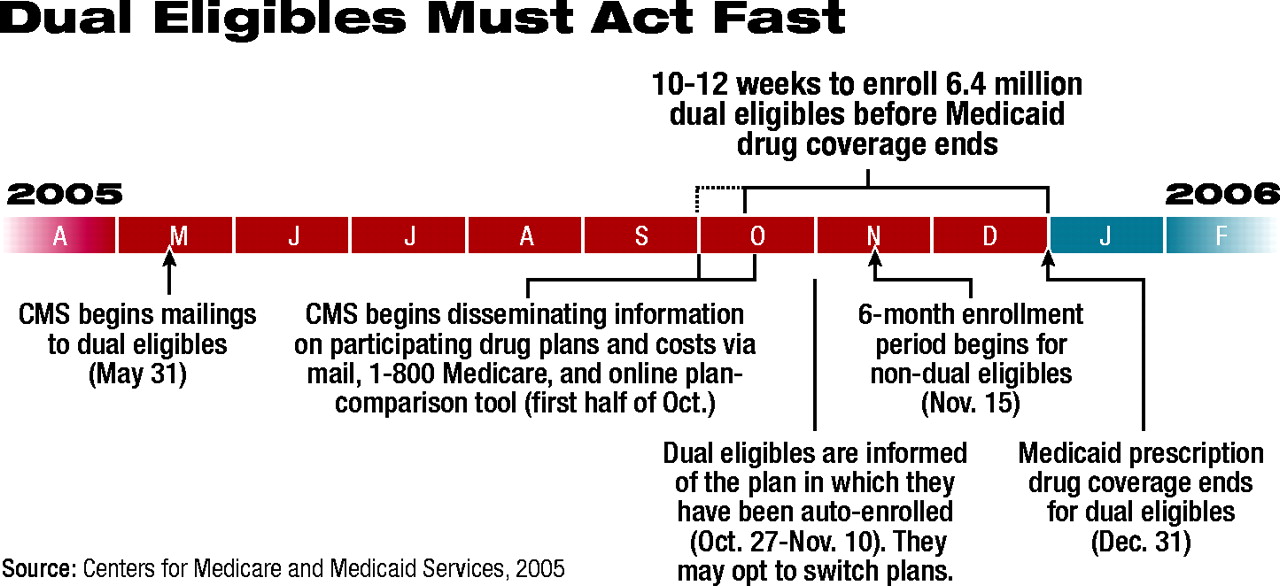
The Medicare Modernization Act (MMA) of 2003, which established the Medicare Part D drug benefit, mandates that prescription drug coverage for dualeligible patients—those eligible for both Medicare and Medicaid due to low income and disability or age—be moved from the state/federal partnership, Medicaid, to the federally funded Part D benefit on January 1, 2006.
Under Part D, all Medicare beneficiaries, including dual-eligibles, will have a choice of at least two prescription drug plans (PDPs) that have contracted with CMS to offer coverage to Medicare beneficiaries in particular geographic regions across the country. Each PDP will design its own benefit structure and drug formulary, based upon a final rule promulgated by CMS and a series of guidance documents issued by the agency (Psychiatric News, February 4, March 18).
The purpose of the hearing, Smith said, was “to determine if improvements are critical to the successful implementation of the Medicare drug benefit, and whether adequate safeguards have been built into the system to protect the poorest and most vulnerable—the dual eligibles.”
The committee's ranking minority member, Sen. Herb Kohl (D-Wis.) added,“ As long as this law goes forward in its current form, it is critical that, when these low-income seniors and disabled beneficiaries are switched to Medicare, that we get it right. If we do not, they face disruptions in drug coverage that could pose serious harm to their health.”
The crux of the problem, many at the hearing agreed, lies in seemingly inadequate patient protections during the transition, in particular for individuals who have been stabilized and maintained on certain medications that have been covered by their state Medicaid program but may not be covered by the PDP that administers their Part D benefits under Medicare.
“The medical literature,” Clark testified, “indicates that a very large percentage of patients forced to switch medications will fail. Typically, this means rapid decompensation into psychiatric crisis—usually within a matter of days. To stabilize the patient again requires an emergency-room admission, followed by a potentially lengthy stay in a hospital. Of course, there is the ever-present threat of suicide during this terrifying downward spiral.”
The hearing's “star witness,” however, disagreed with Clark's position. CMS Administrator Mark McClellan, M.D., Ph.D., testified that the agency's final rule implementing Part D had been carefully structured to ensure that continuity of care was not an issue.
Formularies Being Monitored
“We are paying close attention to make sure that all new drug formularies have access to all medically necessary treatments at the best possible price,” McClellan said. Formularies must “recognize the special needs of many of our beneficiaries, such as those with mental illnesses, those with HIV/AIDS, and those who have been stabilized on very specific and sensitive drug regimens.”
CMS regulations, he argued, require each PDP to submit a specific“ transition plan” outlining how the PDP will deal with patients who are taking a drug prior to January 1, 2006, that is not on the plan formulary and how that patient is to be transitioned to a medication that is covered by the PDP.
“In all these areas, we are looking for the adoption [by PDPs] of best practices,” McClellan noted. “There are good benefits being provided today to very vulnerable populations, and we want to bring in those best practices used, for example, in retiree plans or in current Medicaid plans, and use them with the Medicare population.”
McClellan added, “In fact, there are very good models out there, for example in Medicaid plans that use preferred-drug lists, [showing] how transitions can be effectively managed.”
The option that CMS has discussed with several states, McClellan testified,“ would involve filling a 90-day supply of medication [at the end of December], so that beneficiaries would have some access to their drugs through the first part of 2006.”
However, Kohl pressed McClellan to elaborate on what will happen on January 1, 2006, when a patient comes into the pharmacy to fill a prescription that has been covered by Medicaid, but is not under their new Medicare PDP.
“Senator,” McClellan replied, “we absolutely want to make sure they can continue to get access to the drugs they need.”
With further prodding, McClellan added that CMS had announced a plan ensuring that beneficiaries who come to a pharmacy and do not have a PDP drug card or know what plan they are enrolled in will still be able to get their prescriptions. “If they know their name, date of birth, and basic identifying information, then we'll be able to find them,” he said.“ The pharmacist will be able to tell them how much they have to pay, and they will be able to fill their prescription without a gap.”
“So you are saying,” Kohl pressed even further, “that in no case will they be turned away? They will be able to get their drugs?”
“What I'm saying, Senator, is that we are going to make sure that our beneficiaries have access to all the drug treatments they need without a gap,” McClellan replied.
Antidepressant Access Questioned
Smith questioned McClellan on the “inclusion of antidepressant medications and how they'll be treated within the guidelines.”
Those with mental illness, McClellan replied, are one group of beneficiaries whom CMS will be looking at closely to ensure that a formulary“ doesn't discriminate against some of the people who could most benefit from prescription drug coverage.” CMS, he said, “will be looking at whether or not plans are providing coverage for antidepressants that are similar to effective plans that exist today.”
New PDP formularies will also be compared with existing Medicaid plans'“ preferred-drug lists, and their access provisions, as well as for tiering approaches and the use of other [drug utilization management] tools.”
Most at the hearing, perhaps with the exception of McClellan, believed the transition as now planned will occur too quickly, giving the fragile dual-eligible population little time to understand their options.
“This population is not going to successfully navigate the Internet and 1-800 numbers,” said Tina Kitchin, M.D., medical director of the Oregon Department of Human Services (DHS). “They are going to need the assistance of others to help them navigate this transition. I don't know how [Oregon DHS] is going to do this within the given timeframe.”
McClellan testified that by mid-October, CMS will have data from the states identifying dual-eligible beneficiaries and will begin contacting them both by phone and by mail to inform them that they will be automatically enrolled by CMS and randomly assigned to a PDP in their geographic area. By December, beneficiaries and PDPs will be notified of those random assignments. So within a short period, all beneficiaries will have to be matched with appropriate PDPs. Beneficiaries will be able to change PDP assignment if they find that their randomly assigned plan does not meet their medication needs.
“Unfortunately,” Kitchin noted, “random assignment maximizes the chance that they will be in a plan that is not the best fit for them.”
When Smith asked those testifying what they would like to see in a“ technical corrections” bill aimed at fixing the MMA's flaws, all asked for a phased-in approach with a transition period of at least six months between the start of Part D coverage and the end of Medicaid coverage.
Kohl asked those testifying whether they believed McClellan“ understands [the timeframe concerns] or do you think they're not interested in a six-month transition?”
Clark replied, on behalf of APA, that he believed there indeed was a“ disconnect.” CMS is requiring PDPs to have a transition plan in place, he noted, “yet the reality is that the pharmacy plans aren't doing the transition. The providers are doing the transition. When CMS says there are good practices out there on how to transition people from one medication to another, well, I'm glad there are. But I think most providers don't know what those practices are.”