It is certainly no surprise to learn that the majority of antidepressant, anticonvulsant, and antipsychotic medications dispensed to Georgia Medicaid enrollees in 2001 were for “off-label” indications. However, some patterns of off-label prescribing revealed in a new study are at once intriguing and reassuring, while others may be unexpected.
“We had expected that the prevalence of off-label use of psychotropic medications would be high before we started doing the analysis,” Hua Chen, Ph.D., told Psychiatric News. Chen, an assistant professor of pharmacy at the University of Houston College of Pharmacy, and her colleagues examined patterns of prescribing for antidepressant, anticonvulsant, and antipsychotic medications among patients enrolled in the Georgia Medicaid program in 2001. Their report appeared in the June Journal of Clinical Psychiatry. As part of Chen's doctoral dissertation, the study had no external sources of funding.
Chen reviewed the computerized Georgia Medicaid administrative claims files containing pharmacy, physician, hospital, and nursing home claims to identify Medicaid enrollees who were at least 18 years old as of January 1, 2001, and filled a prescription for any drug in the three classes in 2001. For an enrollee's prescription to be included in the analysis, the patient had to be continuously eligible for Medicaid for 24 consecutive months from January 1, 2000, through December 31, 2001. Chen's team imposed this requirement to allow the inclusion of diagnoses that preceded the prescription use in determining the on- or off-label status of each prescription.
To define off-label prescribing, Chen started with the definition outlined in U.S. Food and Drug Administration (FDA) standards. According to the FDA, off-label prescribing is “the use of a prescription drug for an indication, dosage form, dose regimen, population, or other use not mentioned in the approved labeling.” Due to limitations in the state Medicaid claims database, however, the team did not consider off-label use related to dosage limits, duration of time, or route of administration. In addition, prescribing an antidepressant, anti-convulsant, or antipsychotic for monotherapy, although it is solely labeled for adjunct therapy, was also not considered as off-label use.
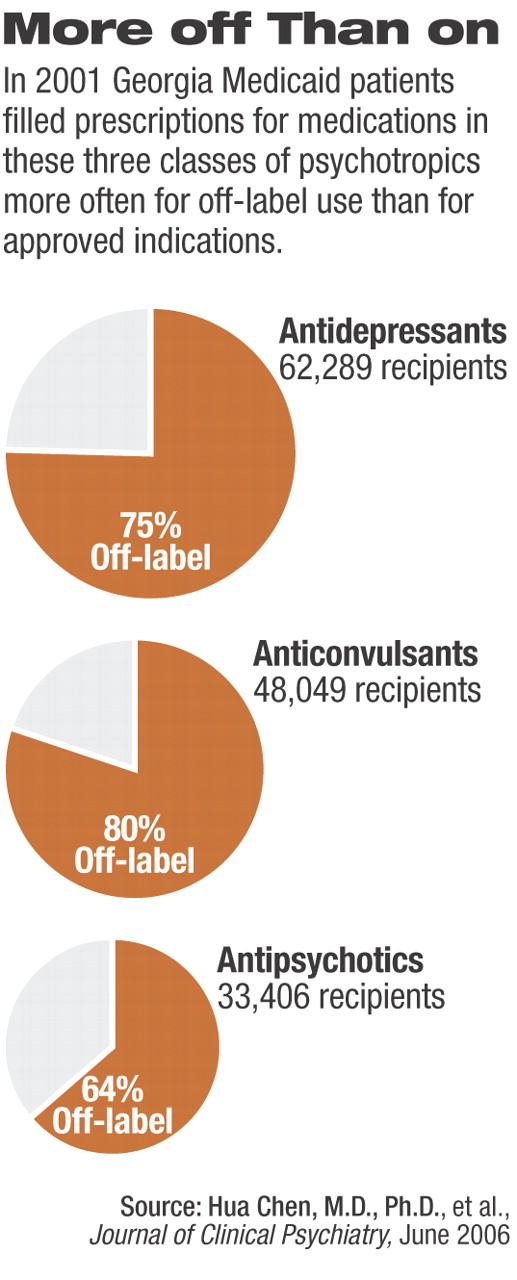
To determine whether a prescription was given for an on- or off-label use, diagnostic codes from the International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) were identified for each indication approved for each antidepressant, anticonvulsant, and antipsychotic medication prescribed. Any prescription for a medication filled during 2001 was categorized as off-label if none of the ICD-9-CM codes listed for the patient during the 24-month study window could be matched with an approved indication for the drug the patient had been prescribed. The overwhelming majority of prescriptions for antidepressants, anticonvulsants, and antipsychotics were dispensed for offlabel indications, according to Chen (see chart below).
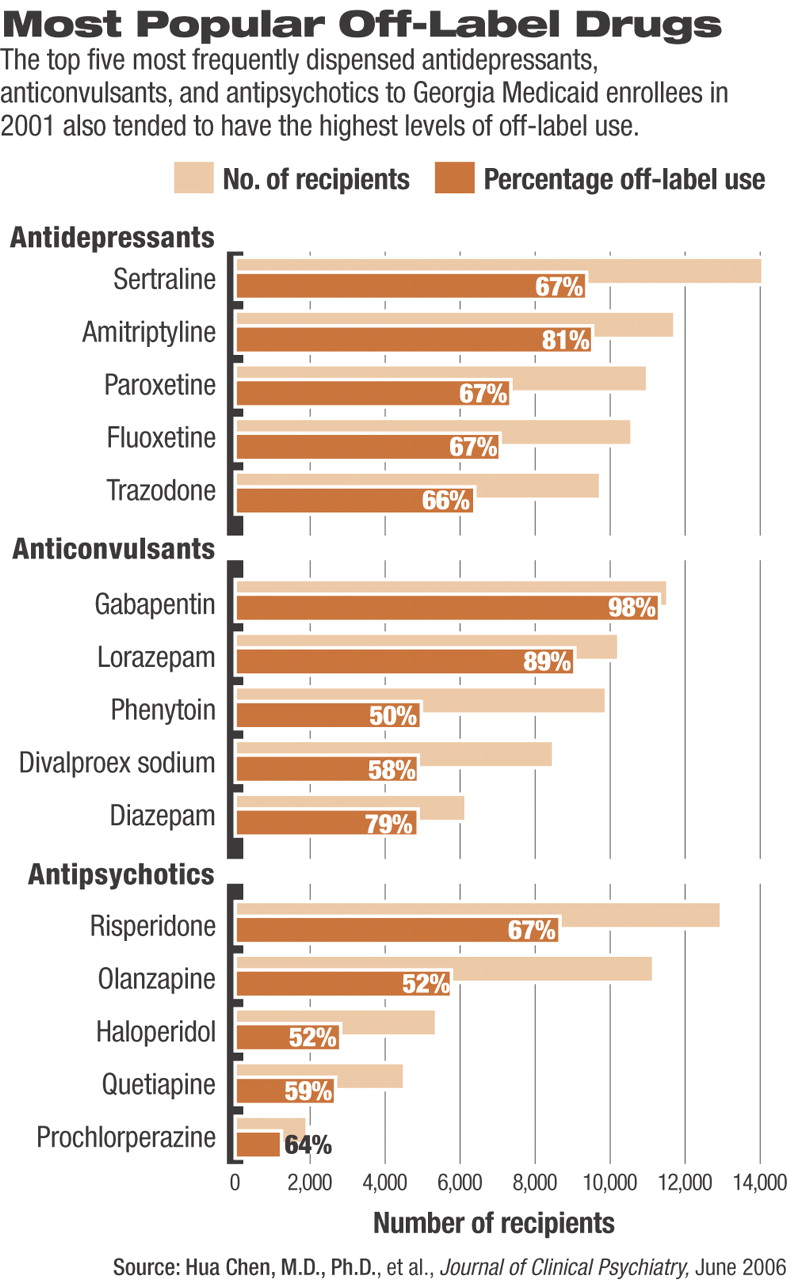
Antidepressants were the most commonly prescribed psychotropic medication, and 75 percent of those prescriptions were for off-label uses, according to the study. Sertraline (Zoloft) was the most commonly prescribed overall; it was prescribed off-label nearly 67 percent of the time. Amitriptyline, the second most common antidepressant prescribed for this population, had the highest level of off-label prescriptions, 81 percent.
Off-label use of anti-depressants was strongly associated with being elderly, with those aged 65 and older being 5.1 times more likely to get an off-label prescription for an antidepressant than those under age 65. Males were 1.5 times more likely than females to get an off-label prescription for an antidepressant. Interestingly, patients with renal failure were 1.4 times more likely than those with no renal problems to use an antidepressant off-label—a finding that was true of all three drug categories. Chen and her team were surprised to find that renal failure was the only common factor that increased patients' odds for off-label prescribing of antidepressants, anticonvulsants, and antipsychotics.
Anticonvulsants, although second of the three drug classes in terms of total prescriptions filled, had the highest percentage of off-label use (80.12 percent). That, Chen told Psychiatric News, was partly driven by the finding that an exceedingly high percentage of prescriptions (98.04 percent) for gabapentin (Neurontin) were filled for off-label uses. While the researchers would have expected a majority of gabapentin prescriptions to be off-label (the drug is approved for use only in patients who have epilepsy with partial seizures or who have postherpetic neuralgia), Chen said her group was surprised by the finding that nearly all gabapentin prescriptions were off-label.
In general, factors associated with increased odds of being prescribed an off-label anticonvulsant again included being aged 65 or older (odds ratio 4.5), along with being white (odds ratio 1.7) and having a prescription for a newer generation anticonvulsant versus an older drug (odds ratio 7.6). Off-label use of anticonvulsants was also associated with several nonseizure disorders, including schizophrenia (odds ratio 1.7), connective tissue disorders (odds ratio 1.5), major depressive disorder (odds ratio 1.4), liver disease (odds ratio 1.4), and diabetes (odds ratio 1.2).
Chen noted that she and her colleagues were also surprised by the relatively high percentage of antipsychotics—specifically “the expensive atypicals”—that were prescribed off-label. Just over 50 percent of prescriptions were for olanzapine (zyprexa) (the most expensive psychotropic medication during 2001) were off-label, while over 65 percent of prescriptions for risperidone (Risperdal) were off-label (see chart on page 16). Chen and her colleagues were surprised to find that those aged 65 and older were 5.2 times more likely to be dispensed an off-label antipsychotic prescription than those under the age of 65. Other factors associated with off-label prescribing of antipsychotics included being white (odds ratio 1.9). Several nonpsychotic disorders were associated with increased odds of being prescribed an off-label antipsychotic, including cyclothymic disorders (odds ratio 3.9), mental retardation (odds ratio 2.5), major depressive disorder (odds ratio 2.1), Alzheimer's disease (odds ratio 2.1), and paralysis (odds ratio 2.2).
“We aren't really able to say whether the off-label uses documented in our study were appropriate or not,” Chen said. “Off-label scripts are commonly written to control certain symptoms, for example, using antipsychotics or anticonvulsants to manage aggressiveness,” Chen explained. ICD-9-CM coding, however, “was designed mainly for identifying diseases, rather than symptoms, and most symptoms may not be coded for billing purposes.”
Some generalizations can be made, Chen said. It would be generally inappropriate, she said, to use a mood stabilizer as monotherapy for a patient with schizophrenia or an atypical antidepressant as monotherapy for a patient with nonpsychotic depression. Yet many of the trends noted appear to be plausibly appropriate, such as using anticonvulsants for patients with pain disorders or using antipsychotics for youth with more severe behavioral disorders such as attention-deficity/hyperactivity disorder with conduct disorder or intermittent explosive disorder.
Chen told Psychiatric News that the study findings “can be generalized to almost all Medicaid populations. Although there are minor differences in benefit designs across Medicaid plans, they all have relatively comprehensive coverage on psychotropic medications, and pharmacy benefit management tools have not been extensively used to control psychotropic drug costs in Medicaid, according to a recent study published on Health Affairs.
But the findings are not generalizable to the general population, she noted. “The prevalence of off-label prescribing estimated from our study is slightly higher than the estimates derived from the general population because Medicaid plans tend to have a more generous coverage than commercial insurance on psychotropic medications, especially on antipsychotic drugs, and Medicaid covers a majority patients with severe mental disorders.”
“Off-Label Use of Antidepressant, Anticonvulsant, and Antipsychotic Medications Among Georgia Medicaid Enrollees in 2001” is posted at<www.psychiatrist.com/abstracts/200606/060615.htm>.▪
