On January 17 the U.S. Supreme Court upheld oregon's assisted-suicide law, which lets physicians help terminally ill patients end their lives (Psychiatric News, March 3). The decision paves the way for any other state that wants to adopt a similar law, and a few are considering it.
“Booth Gardner, who was a two-term governor in Washington state, has said that he will lead an initiative effort in Washington on assisted dying,” Len Eddinger, senior director of legislative and regulatory affairs for the Washington State Medical Association, told Psychiatric News.
“There has been a bill in the Vermont legislature for the last several years that would allow physician-assisted suicide,” Steve Larose, executive secretary of the Vermont Psychiatric Association, commented.
“Yes, we do have a bill such as Oregon's, it's AB 651 (Berg, Levine), California's Compassionate Choices Act,” Randall Hagar, director of government affairs for the California Psychiatric Association, told Psychiatric News. “The bill passed our Assembly on strict party-line votes last June,” he said, but it failed to make it out of the Senate Judiciary Committee after discussions in June of this year.“ It never reached the Senate floor because there were key issues that remained unresolved between the authors and a powerful committee chair,” Hagar noted. “Those concerns had to do with whether or not the bill had adequate protections in it to protect patients from coercion.”
Hagar said that according to a representative of Assembly Rep. Patty Berg, who co-authored the bill, she and co-author Rep. Lloyd Levine intend to reevaluate their options regarding the bill in the coming months, but both“ remain committed to the issue.”
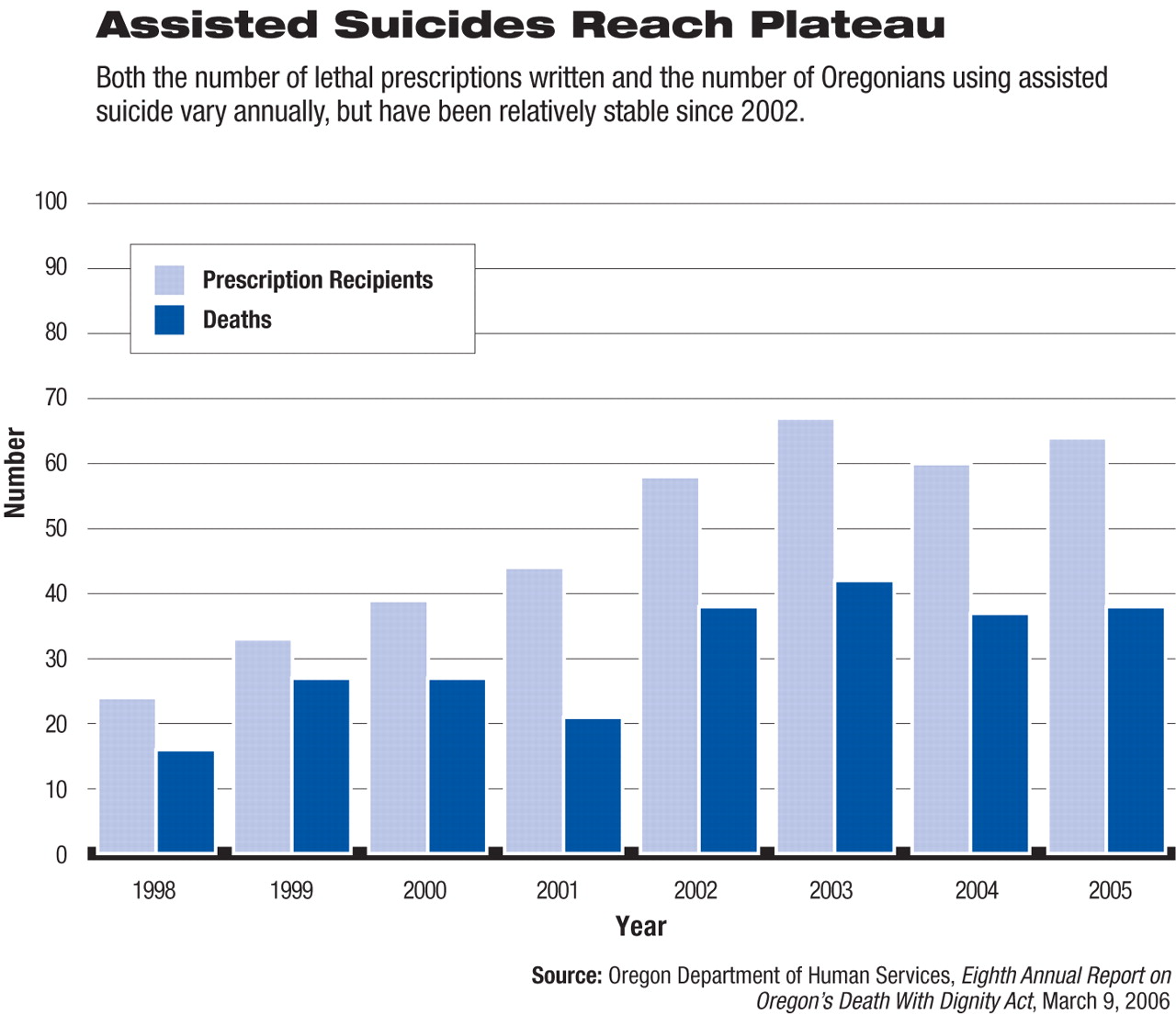
Although the future of assisted suicide in these and other states is far from clear, what is more evident is the impact that Oregon's assisted-suicide law has had on that state's clinicians and terminally ill patients since it took effect on November 5, 1997.
The bulk of that information comes from the Oregon Department of Human Services-Health Services, which is legally required to monitor compliance with the law, collect information about patients and physicians who participate in physician-assisted suicide, and publish an annual statistical report. Linda Ganzini, M.D., a professor of psychiatry at Oregon Health and Science University, and her colleagues have also published studies on the subject.
Which Physicians Take Part?
Those physicians who are in the front line of dealing with patients who want assisted suicide are mostly family practitioners, oncologists, and internists, according to the Eighth Annual Report on Oregon's Death With Dignity Act, published in March by Oregon's Department of Human Services-Health Services.
However, under the Oregon assisted-suicide law, not just the attending physician but a consulting physician must agree on a patient's diagnosis and prognosis before he or she can be eligible for assisted suicide—that is, the patient must be diagnosed with a terminal illness that will lead to death within six months. Moreover, if either the attending or consulting physician believes that the patient's judgment is impaired by depression or another psychiatric disorder, then that patient must undergo a mental health evaluation, Darcy Niemeyer explained in an interview. Niemeyer oversaw the Eighth Annual Report on Oregon's Death With Dignity Act. She was assisted by epidemiologists Richard Leman, M.D., and Melvin Kohn, M.D., and by statistician David Hopkins.
The mental health evaluations can be conducted by either psychiatrists or psychologists, Niemeyer noted, although “so far, all physician-assisted-suicide evaluations have actually been performed by psychiatrists, and all have been for evaluation of depression.”
And just as patients' mental health can influence their desire for assisted suicide, patients' requests for assisted suicide can influence the mental health of physicians who are asked to participate, Ganzini and her coworkers reported in the May/June 2004 Journal of Palliative Medicine.
Semistructured interviews were conducted with 35 Oregon physicians who had received assisted-suicide requests from patients. The interview results revealed that the physicians often felt unprepared and experienced apprehension and discomfort before and after getting requests. The physicians were especially concerned about adequately managing patients' suffering, not wanting to abandon patients, and not completely understanding patients' preferences, especially when they did not know the patients well.
On the other hand, regardless of whether they prescribed lethal medications for assisted-suicide patients, the physicians did not express major regrets about their decisions and indicated that requests for assisted suicide helped them discuss crucial end-of-life issues with patients.
Who Requests Assisted Suicide?
Indeed, a number of end-of-life issues have propelled patients to request assisted suicide since the law went into effect, the Oregon report reveals. The concerns of greatest importance to patients have been loss of autonomy, decreasing ability to participate in activities that make life enjoyable, and loss of dignity.
Concerns of lesser importance included a loss of control over body functions, fear of being a burden to family and friends, inadequate pain control, and the financial implications of treatment.
And as to why patients with amyotrophic lateral sclerosis (ALS) in particular have sought assisted suicide, a study conducted by Ganzini and colleagues and published in the September 2002 Journal of Pain and Symptom Management offers some insights.
Information was gathered on how 50 patients with ALS felt during the months before they died—for example, whether they were depressed, felt hopeless, or were in pain and how much social support they had—and whether they wanted assisted suicide.
One-third of the ALS patients discussed the option of assisted suicide during the last month of life. Hopelessness at the start of the study predicted a desire for assisted suicide later on. A major depressive disorder at the start of the study, however, did not. (This finding is at odds with one reported by William Breitbart, M.D., chief of the psychiatry service at Memorial Sloan-Kettering Cancer Center, in the December 13, 2000 JAMA. That study found that hopelessness and depression contributed to terminally ill patients' desire for a hastened death.)
By the end of 2005, 390 individuals in Oregon had obtained lethal prescriptions, and 246 had used them to die, according to the report on Oregon's Death With Dignity Act. Although there are year-to-year variations in the characteristics of patients who used assisted suicide, certain demographic patterns have become evident. Males and females were equally likely to use it. Divorced and never-married persons were more likely to use it than were married or widowed individuals. A higher level of education has been strongly linked with its use. Patients with certain types of terminal illnesses, such as ALS, AIDS, and cancer, are especially likely to take advantage of it.
Oregon's health department does not track the persons who wanted assisted suicide yet were screened out after getting a mental health evaluation, Niemeyer explained. However, the department does track those who are not eliminated after a mental health exam. Thus, data show that out of the 246 individuals who died by assisted suicide by the end of 2005, 212 (86 percent) had not received a mental health evaluation before-hand, yet 34 (14 percent) had. And the reason why the 86 percent had not gotten such an evaluation was because their attending and consulting physicians did not think that their judgment was marred by mental illness; the reason that the 14 percent had received such an evaluation was because their attending and consulting physicians suspected that their judgment might be impaired.
Of 67 patients who wanted to use assisted suicide, but were given pain control, anti-depressant medication, referral to a hospice program, or other substantive help, 46 percent changed their minds, Ganzini and her team reported in the February 24, 2000 New England Journal of Medicine.
In contrast, only 15 percent of 73 patients for whom no substantive intervention was made changed their minds. (A new study finding by Breitbart and his group, and shared with Psychiatric News, complements these results. They have found that treating depression helps reduce patients' desire for a hastened death.)
Even with these insights, though, a lot about the impact of Oregon's assisted-suicide law on Oregon clinicians and terminally ill patients is not publicly available. “That is why, once again, we call for open and impartial review of anonymous assisted-suicide cases in Oregon,” N. Gregory Hamilton, M.D., an Oregon psychiatrist, argued in a letter published in the June American Journal of Psychiatry.
The “Eighth Annual Report on Oregon's Death With Dignity Act” is posted at<www.Oregon.gov/DHS/ph/pas/docs/year8.pdf>.▪
