The latest round of results from the national institute of Mental Health's STAR*D (Sequenced Treatment alternatives to relieve Depression) trial underscore the difficult challenge clinicians and patients face with depression that does not respond to an adequate course of antidepressant therapy.
Two new articles from STAR*D investigators, appearing in the September American Journal of Psychiatry, detail the results from levels 3 and 4 of the complex study. While far from encouraging, these reports indicate that remission is still possible, even after a patient fails to achieve the elimination of nearly all symptoms after taking as many as three rounds of antidepressant therapy.
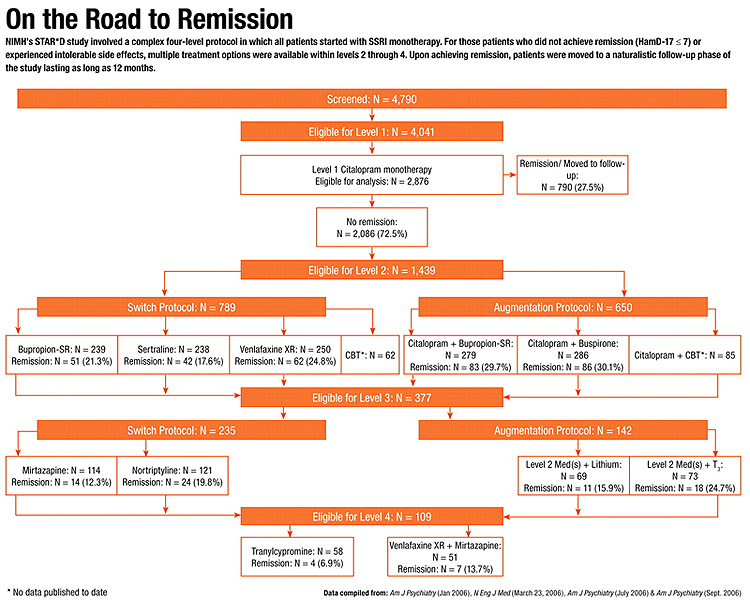
Perhaps more important, the collective reports from STAR
*D's four levels (see
chart below) may provide clinicians and their patients with the study's greatest legacy: a“ road map” of sorts showing them how to navigate the multi-drug route through depression treatment on the way to remission.
In an editorial accompanying the reports, Marcia valenstein, M.D., an assistant professor of psychiatry at the University of Michigan School of Medicine concludes that STAR*D “has provided important evidence applicable to clinical decision making by ordering treatments by relative efficacy or tolerability at specific therapeutic junctures.” However, future studies, she added, must build on STAR*D's accomplishments.
“The STAR*D program has provided the best quantitative data available on the likely result of moving through a rational sequence of treatments for patients who do not achieve remission from firstline SSri treatment,” said Darrel regier, M.D., M.P.H., director of APA's Division of research and executive director of the american Psychiatric institute for research and education.
“These additional studies show that some patients, unresponsive to previous treatments, do eventually improve, thereby increasing overall response and remission rates,” regier told Psychiatric News. according to the six reports of STAR*D results published to date (more data remain to be analyzed and published), a total of 1,191 (41.5 percent) of the original 2,876 patients in the four-level STAR*D analysis achieved remission.
The six-year, $35 million STAR*D project was designed to study the types of patients most likely to be seen in everyday clinical practice: those likely to have comorbid disorders, including additional medical diagnoses and the possibility of more than one axis i disorder. The protocol aimed to determine what the “next best steps” are for that majority of depression patients (70 percent on average) who find either inadequate relief or intolerable side effects with the first medication they try.
In the first of the two current AJP articles, STAR*D investigator andrew nierenberg, M.D., an associate professor of psychiatry at Harvard Medical School and Massachusetts General Hospital, and his colleagues report on outcomes of patients in the augmentation pathway of the study's level 3.
Each of the 142 patients in the level 3 augmentation pathway had previously failed to achieve remission or encountered unacceptable side effects with 12-14 weeks of citalopram monotherapy in level 1, and a second treatment option in level 2.
To augment each patient's medication regimen from level 2, patients were randomly assigned to one of two level 3 options: either lithium or triiodothyronine (the thyroid hormone, T3). Treatment assignments and dosing were not masked to participants or their treating clinicians, and dosing was flexible.
Lithium was chosen, the report noted, because of preclinical data indicating that it increases the presynaptic formation, storage, and release of serotonin. It is thought that lithium may have a synergistic effect on the mechanism of action of serotonergic antidepressants. In addition, there is limited clinical trial evidence that lithium is effective in augmenting the therapeutic effects of tricyclic antidepressants.
There is also evidence that supplementation with thyroid hormone in patients with depression may be useful in boosting antidepressant efficacy, even if a patient's thyroid function is normal. Some have postulated that supplementing T3 may desensitize inhibitory 5-HT1a receptors; directly affect gene expression; and increase brain metabolism.
Patients in level 3 who had augmented citalopram with buspirone or sustained-release bupropion in level 2 discontinued the augmenting agent without tapering. Lithium or T3 was added to the patients' assigned level 2 antidepressant.
Lithium was initiated at 450 mg per day, then increased after one week to 900 mg per day. T3 was initiated at 25 mcg per day for the first week, then increased to 50 mcg per day. Patients were allowed to take anxiolytics and sedative hypnotics, but other psychotropic medications were not permitted by the protocol.
The primary outcome measure was remission, defined (throughout every level of the protocol) as a score of 7 or less on the 17-item Hamilton Depression Rating Scale (HamD-17). Baseline scores on the HamD-17 and other measures indicated that the patients beginning treatment in level 3 on average“ had a moderate degree of symptom severity...[with] very poor life satisfaction and function.”
The overall mean duration of level 3 treatment was 9.6 weeks out of the possible 14. Mean daily doses at exit were 860 mg for lithium and 45.2 mcg for T3. Serum lithium levels were only obtained in 39 of 69 participants (57 percent) taking the drug, with the mean blood level being 0.6 meq/liter—on the low end of the recommended therapeutic range of 0.6 meq/liter to 1 meq/liter.
Remission Becoming Elusive
Overall, 15.9 percent of the group augmenting with lithium achieved remission compared with 24.7 percent of those augmenting with T3. There were no significant differences between the two groups taking the different augmenting agents. In addition, no statistically significant differences were found in the proportion of patients achieving remission based on what level 2 agent they were augmenting.
Few participants experienced serious adverse events. More patients taking lithium reported significant side effects compared with those taking T3; however, the difference was statistically significant only for the frequency, not intensity or burden, of side effects. Significantly more patients taking lithium withdrew from the study because of side effects.
The researchers noted that the “modest remission rates observed with lithium augmentation may have been due to the low doses used as a result of limited toleration of side effects. Nevertheless, these results probably reflect what clinicians can expect with lithium augmentation in actual practice.”
They concluded that the two augmenting agents were statistically effective, yet noted that “T3 has slight [numerical] advantages over lithium in effectiveness and tolerability. T3 also offers the advantages of ease of use and lack of a need for blood level monitoring.”
Level 4: An MAO-I vs. Combo Rx
The second STAR*D article appearing in this month's AJP, with Patrick McGrath, M.D., co-director of the Depression Evaluation Service at New York State Psychiatric Institute as the lead author, details outcomes of the 109 patients who entered level 4 of the protocol.
Each of these patients failed to achieve remission or was unable to tolerate adverse events with their level 3 switch or augmentation protocol medications.
In level 4, patients discontinued their previous antidepressant therapy and were switched to either the monoamine oxidase inhibitor tranylcypromine or a combination of venlafaxine-extended release and mirtazapine. Again, treatment was open label.
Tranylcypromine was initiated at 10 mg per day for the first two weeks, followed by increases of 10 mg per day each week until a target dose of 60 mg per day was reached. All patients taking tranylcypromine completed a two-week washout of their level 3 medications prior to their first dose in level 4.
For the combination treatment, venlafaxine XR was started at 37.5 mg per day for the first week and titrated up to a target of 300 mg per day after week eight. Mirtazapine was initiated at 15 mg per day and increased to 45 mg per day after week eight.
McGrath and his colleagues reported that remission rates did not differ significantly, with 7 percent of subjects taking tranylcypromine reaching remission compared with 14 percent of patients taking the venlafaxine XR/mirtazapine combination. However, the percentage of reduction in depressive symptoms was significantly greater for patients taking the combination therapy (25 percent compared with 6 percent for tranylcypromine.)
“Though remission rates were modest for either tranylcylpromine or the combination treatment, the response to the medications was adequate enough to justify either as a treatment alternative,” McGrath said in a press release.
However, Valenstein noted in her editorial that “unless a drug produces a very large benefit, its placement later in a trial sequence frames much of the subsequent discussion. Drugs used later can be discussed only in the context of `down-line' options.” Yet, she added, those“ down-line” options in the study protocol should not be viewed as“ last resort” options.
While the full impact of the massive volume of STAR*D data will not likely be determined for some time, many are hopeful the study will advance the treatment of depression in multiple clinical settings.
Noting that 40 percent of STAR*D participants were followed in their primary care settings, Frank DeGruy, M.D., a professor and chair of family medicine at the University of Colorado Health Sciences Center, wrote in a second accompanying editorial that “STAR*D and a few confirmatory studies should make it possible for primary care clinicians themselves to push care decisions to the third or fourth step before seeking a consultation.”
However, rather than resulting in an overall decrease in consultation between psychiatry and primary care, DeGruy added, the result would likely be“ the seeking of consultations for more complicated patients and even more difficult problems.”
Both articles, as well as the two accompanying editorials, are posted at<www.ajp.psychiatryonline.org>.▪