During the past decade, two clinical trials, one in Australia and one in North America, have been launched to answer an important question: If young people experiencing prodromal schizophrenia symptoms are treated with an antipsychotic medication, will it delay their succumbing to schizophrenia or perhaps even prevent it?
Although preliminary results from the Australian trial, headed by Patrick McGorry, M.D., Ph.D., executive director of the ORYGEN Research Center at the University of Melbourne, suggest that the answer might be yes, final results have not yet been published (Psychiatric News, June 3, 2005).
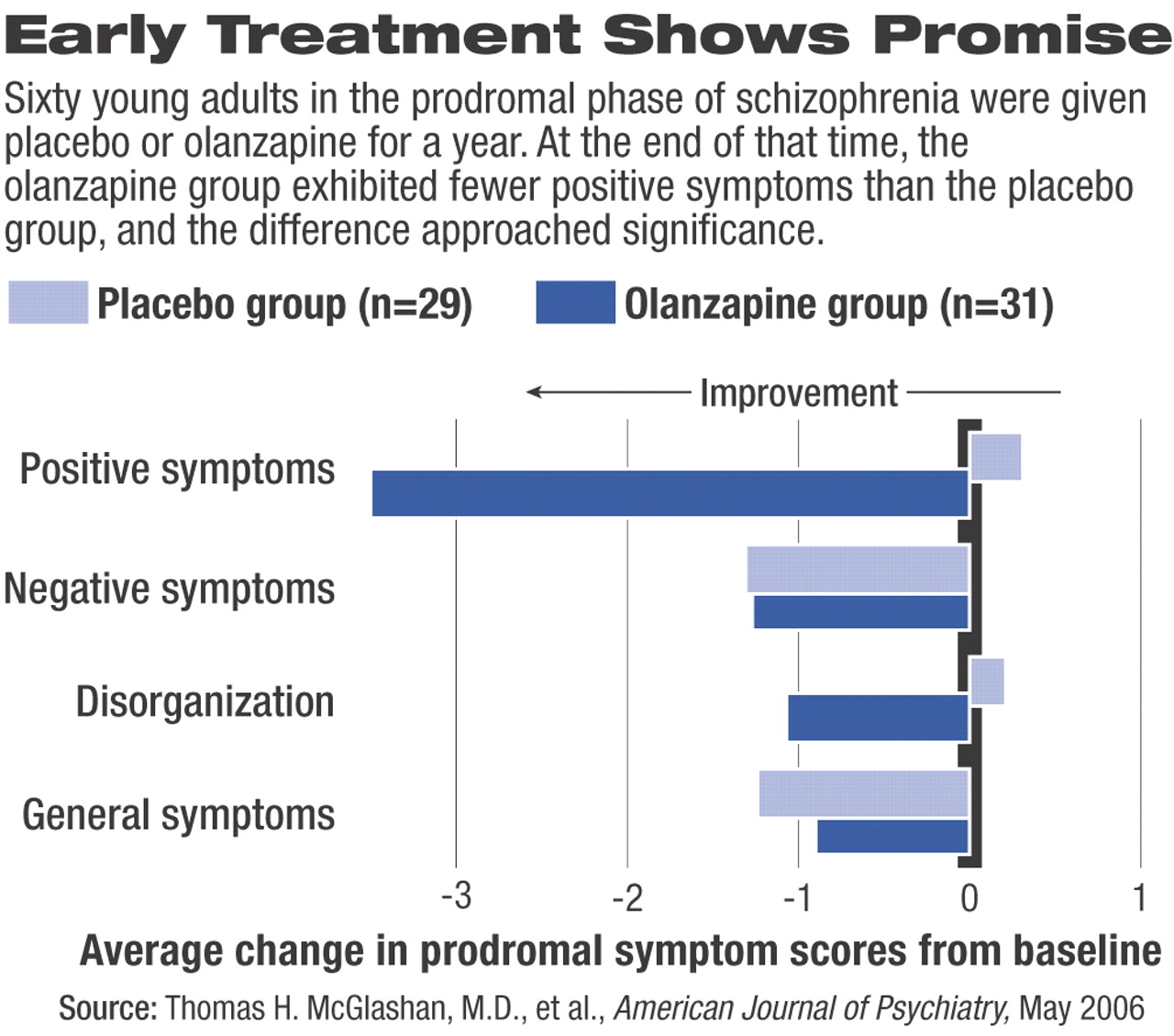
In contrast, final results from the North American trial, headed by Thomas McGlashan, M.D., a professor of psychiatry at Yale University, appear in the May American Journal of Psychiatry. But unfortunately, they do not provide a clear answer to the question.
In 1997 McGlashan and his coworkers started recruiting young adults at high risk of developing schizophrenia for their study. They eventually identified 60 subjects, with an average age of 16 years. For a year, 31 of the subjects received the antipsychotic drug olanzapine (5 mg to 15 mg daily), and 29 of the subjects were given a placebo. The investigators monitored the mental health of both groups not only during the treatment year, but also during the year after treatment had stopped. The scientists then compared the mental health outcomes of both groups.
During the treatment year, they found, 11 out of the 29 controls—38 percent—converted from a prodromal state to psychosis, compared with only five of the 31 getting medication—16 percent. The difference, however, was not statistically significant.
Moreover, only 17 of the 60 subjects—nine from the treatment group and eight from the placebo group—remained in the study during the year after treatment ended. Of the nine treatment subjects, three developed psychosis, and of the eight placebo subjects, two did. These numbers and rates were too small for meaningful comparisons.
Nonetheless, the difference between the treatment group and the placebo group with regard to treatment-year conversion to psychosis was “nearly significant,” McGlashan and his group pointed out in their report. Also,“ the hazard of conversion [during the treatment year] among placebo patients was about 2.5 times that among olanzapine-treated patients, which also approached significance.”
If more subjects had remained in the trial during the year following treatment, the researchers reasoned, they might have had enough statistical power to demonstrate that olanzapine can thwart the transition to psychosis. Thus, the researchers concluded that more clinical trials—especially trials with more subjects and with longer assessment periods—need to be undertaken to determine whether antipsychotic treatment can really influence the transition.
Even if such trials do demonstrate that antipsychotic treatment can keep patients' prodromal symptoms from evolving into full-blown schizophrenia, it will still be necessary to explore whether the effect is true prevention or simply a delay in illness development. At this juncture, McGlashan and his group suspect that it is a delay. One reason, they write, is that if olanzapine were “truly preventive, we would expect to find few, if any, former olanzapine patients converting [to psychosis during the year following treatment]. In fact, three of nine patients (33.3 percent) did convert.”
The study was funded by Eli Lilly and Co., the National Institute of Mental Health, and the Tapscott Chair in Schizophrenia Studies at the University of Toronto.
“Randomized, Double-Blind Trial of Olanzapine Versus Placebo in Patients Prodromally Symptomatic for Psychosis” is posted at<http://ajp.psychiatryonline.org> under the May issue. ▪