Women with a history of depression are at greater risk of postpartum depression than are women without such a history, and psychiatrists need to be sensitive to this association, suggest findings from a study to be published in the October American Journal of Psychiatry.
Researchers found that about one in seven women was identified with and treated for depression in a period spanning 39 weeks prior to pregnancy and 39 weeks after pregnancy.
In addition, in more than half of the women who were diagnosed with depression before pregnancy, the depression reoccurred later in the pregnancy or after the baby was born.
Patricia Dietz, Dr.P.H., lead author of the report, said the study underscores the need for continuity of care before, during, and after pregnancy for women of childbearing years. Dietz is an epidemiologist with the Centers for Disease Control and Prevention.
“Because depression can be a chronic condition, we found reoccurrence happened during pregnancy as well as during the postpartum period,” Dietz told Psychiatric News.
In the study, Dietz and colleagues analyzed the prevalence of depression and treatment types received for depression among members of the Kaiser Permanente Northwest health plan. They used a validated algorithm to identify members with at least one pregnancy between January 1, 1998, and December 31, 2001.
Women with a pregnancy ending in one or more live births and continuously enrolled from 39 weeks before pregnancy through 39 weeks after pregnancy were eligible. Maternal depression was identified from the medical records. Depression treatment included antidepressant medication and/or “mental health visits.”
Treatment for depression was defined as receiving at least one dispensing of antidepressant medication identified through pharmacy records or at least one mental health visit identified through electronic medical records with a depression or dysthymia diagnosis.
They found that among 4,398 continuously enrolled women with eligible pregnancies ending in live births, 678 (15.4 percent) had depression during at least one pregnancy phase.
Of women identified with depression during the 39 weeks following pregnancy, 54.2 percent had depression diagnoses either during or preceding pregnancy.
“For clinicians, this means asking women during the initial prenatal care visit about any previous experiences with depression,” Dietz told Psychiatric News. “If a woman reports previous experiences, then the clinician should begin a dialogue with the patient regarding her mental health and check in with her throughout the pregnancy and at the six-week postpartum visit to assess how she is doing.
“It is also important to note that approximately half of the women who were diagnosed with depression during pregnancy and approximately half of the women who were diagnosed during the postpartum period did not have a previous diagnosis in the study period,” she said. “Therefore, clinicians should be aware that depression can be experienced by any of their patients, not just those women with a previous history of depression. Asking women a two-question screen can be an efficient way to identify women with depression, as some women may be reluctant to discuss it with their prenatal care provider.”
Dietz said the two questions are: During the past month, have you been bothered by feeling down, depressed, or hopeless? During t he past month have you often been bothered by little interest or pleasure in doing things?
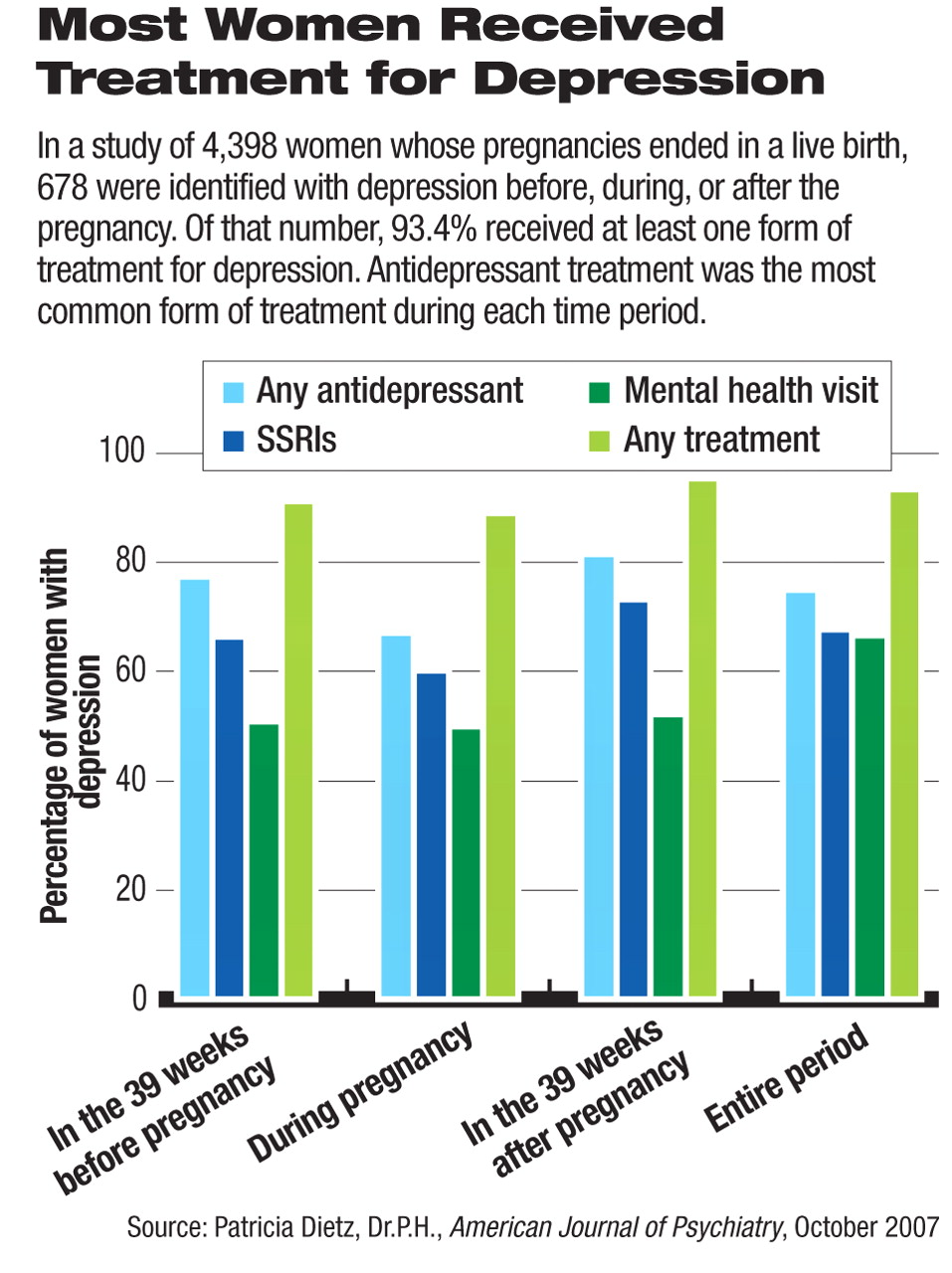
The study also offered what looks like good news: the vast majority of women with depression in this large regional health plan received some form of treatment for depression, either medication or mental health visits (see chart).
“We were encouraged that over 93 percent of women with a depression diagnosis during the study period received some kind of treatment, which suggests that women similar to those at Kaiser Permanente Northwest will seek treatment when diagnosed,” Dietz said.
“We did not know what level of antidepressant use during pregnancy we would find in this study because we were not aware of any previously published percentages of antidepressant use among depressed pregnant patients,” Dietz said. “Given women's general reluctance to use any type of medication during pregnancy, we had expected to see an increase in the use of mental health visits during pregnancy, which we did not.”
More predictably, however, treatment with antidepressants during pregnancy was lower than it was prior to pregnancy (77 percent) or after pregnancy (81.5 percent).
APA president-elect Nada Stotland, M.D., who reviewed the study, said it underscores the need for clinicians to keep up with the ever-changing literature on the treatment of depression during pregnancy. She noted that APA and the American College of Obstetricians and Gynecologists will soon release a brief summary of the literature along with an outline for making treatment decisions.
“Clinicians need to remember that childbearing age encompasses a wide range of ages, and women in all kinds of life situations can become pregnant,” Stotland said. “Most pregnancies are not planned. Many women are on antidepressants. Not uncommonly, women discover that they are pregnant only after having taken medication for the first, crucial weeks and months of pregnancy.
“Therefore the possibility of pregnancy should be taken into account whenever postpubertal and premenopausal women are treated for depression. That does not mean that medication should be withheld; it means that clinicians should discuss the possibility of and implications of pregnancy when discussing treatment options.”
“Clinically Identified Maternal Depression Before, During, and After Pregnancies Ending in Live Birth” will be posted online at<ajp.psychiatryonline.org> under the October issue. ▪