The road to mental health reform may be paved with the best of intentions, but when the potholes get bigger after the repairs, people start to wonder.
North Carolina is bumping along through another upheaval in its public mental health system as citizens, patients, legislators, psychiatrists, and mental health professionals try to recover from the previous upheaval.
Legislators and policymakers shook up the system about seven years ago, but the resulting reforms proved at least as problematic as the conditions they were intended to cure.
“We tried to fix it, and we broke it,” said one legislator, according to news reports.
Now the state is trying again to pick up the pieces and patch together a functional system.
Until 2001, North Carolina's system tied four large psychiatric hospitals scattered across the state with 39 area mental health, developmental disability, and substance abuse programs, supplemented by contracts with private agencies.
“The clinic-based area programs were local, safety-net operations with state funding,” Debra Dihoff, M.A., executive director of the North Carolina branch of the National Alliance on Mental Illness and a former executive in the system, told Psychiatric News. Many were overwhelmed by growing caseloads after Medicaid and managed care were introduced.
The state was late in adopting many of the changes developed in public mental health and managed them badly in the process. It mishandled the Medicaid transition, and staffing, record-keeping, and physical-plant problems in the hospitals drew the attention of the Department of Justice in 2001.
Faced with a system on the verge of collapse, the Office of the State Auditor produced a report in 2000.
Among other things, the auditor's report called for cutting 667 beds from the 2,400-bed state hospital system, developing specialized outpatient services for targeted populations, and creating a separate developmental-disabilities division.
The most significant change, however, came in the creation of local management entities (LMEs) to administer, fund, and oversee—but not provide—services in each county. In theory, psychiatrists, social workers, psychologists, and other clinicians would leave the shrinking state system and reassemble into private-practice groups. Proponents argued that privatization would be more efficient and less costly and permit more rapid innovation than the public system.
Children, the elderly, the severely mentally ill, and substance-using populations would receive state-funded treatment, while others would use the county-based community support services.
Psychiatric Input Overlooked
“[The plan] didn't look too bad, but it left out a lot of input from professional groups,” said Stephen Kramer, M.D., a professor of psychiatry at Wake Forest University School of Medicine and president of the North Carolina Psychiatric Association, in an interview.
The auditor's report was handled at arm's length by politicians, said Marvin Swartz, M.D., a professor of psychiatry and chief of the Division of Social and Community Psychiatry at Duke University. “There was no visionary leader with influence.”
Gov. Mike Easley (D) employed a delegating management style and had little personal interest in mental health, Swartz said. State legislators had a poor grasp of the complexity surrounding mental health and simply said: “Fix it—just tell us what you want.”
Whatever its intentions, the new system didn't work, said Swartz, who served as a consultant to the state auditor.
“Implementation was poor,” Swartz said. “There were not enough people or knowledge or cash flow to implement a plan that was poorly designed.”
“It was supposed to be budget neutral, but funding was inadequate before the reforms and more inadequate afterward,” said Kramer.
Privatization also exacerbated an existing shortage of psychiatrists, said Swartz. Psychiatrists had always been “loss leaders” in the state system. Not all the work they did with complex patients was reimbursable, but cost-shifting under the area programs kept the system in balance. That couldn't be sustained with the reforms.
There was another factor as well. “People who work in the public sector are not entrepreneurs,” said Swartz. “Some former public psychiatrists joined provider groups, but many left the field or the state because their income stream became too uncertain.”
Fewer Psychiatrists Available
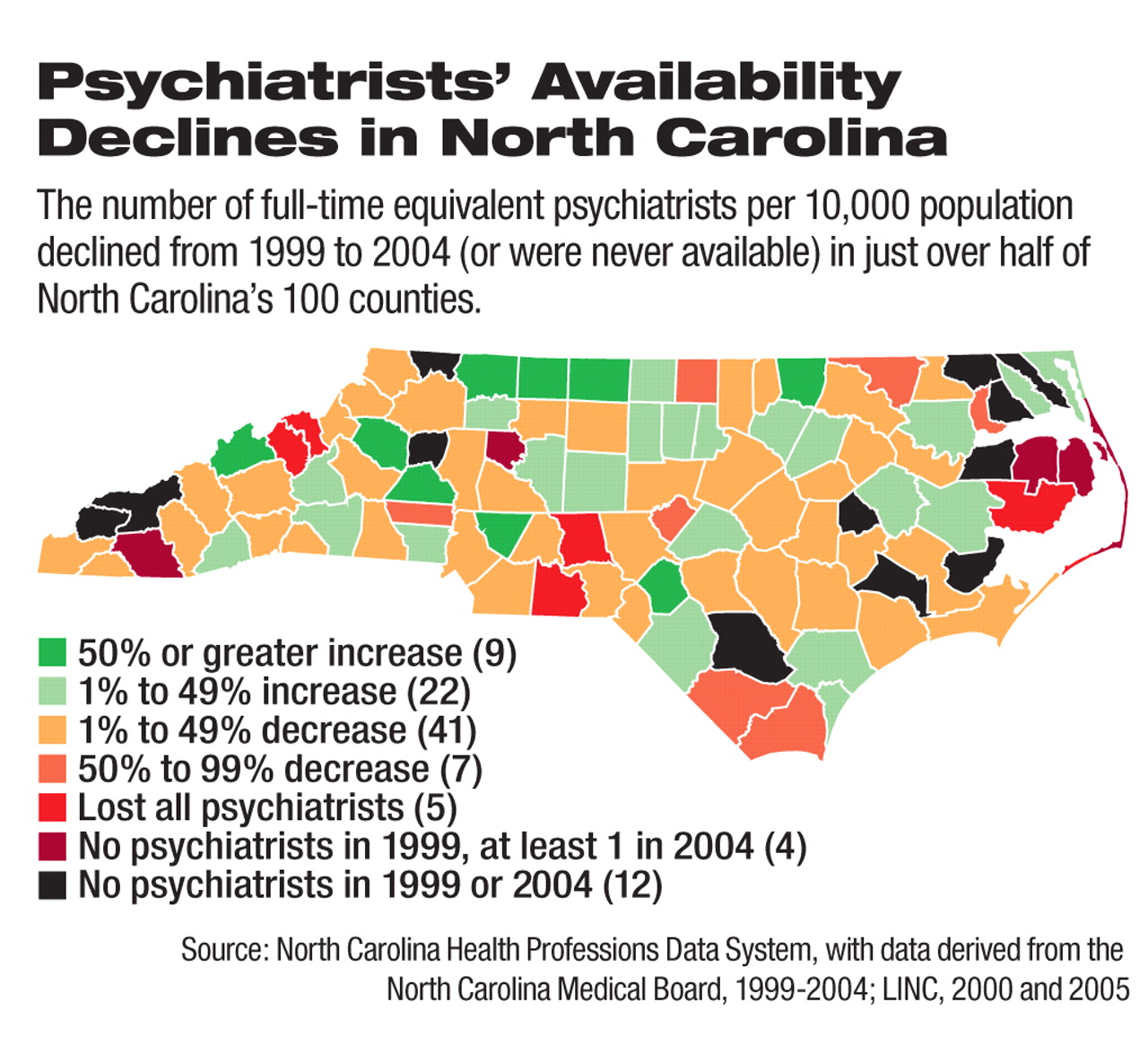
The supply of psychiatrists declined in about half of North Carolina's 100 counties during the period, according to a report by Swartz and his colleagues.
“Between 1999 and 2004, five counties lost all their psychiatrists, 48 counties experienced a decline in their supply relative to population growth, and 12 counties had no psychiatrists in either 1999 or 2004,” they wrote.
The role of psychiatrists was undercut further because of the“ quasi-fraudulent” system that developed in the early years of reform.
Provider organizations were paid a flat $61-an-hour fee to provide services, regardless of who treated the patient. Some (although not all) dispatched low-level (and low-paid) paraprofessionals to perform ill-defined“ community support” services and pocketed the difference. The state had no mechanism to monitor these practices until the system went hundreds of millions of dollars over budget, said Swartz.
“The mental health plan did not carry clear lines of accountability,” said Vicki Smith, M.S., executive director of Disability Rights North Carolina, in an interview. “It was built on the assumption that all entities would do the right thing. You have to build community capacity first, but they didn't do that.”
It's a Long and Winding Road
“I wouldn't say reform failed, but it certainly has taken longer than expected to get it right,” said psychiatrist Michael Lancaster, M.D., who in January was named codirector of the state's Division of Mental Health, Developmental Disabilities, and Substance Abuse Services.
Service definitions from the Centers for Medicare and Medicaid Services were approved only in 2006, two years later than expected, said Lancaster. The wholesale privatization of the system was clearly too radical, he said.“ You need a public/private partnership to maintain a safety net.”
Community support, said Lancaster, was intended to get people connected with services, build skills, and promote recovery, not serve as a substitute for long-term outpatient care.
“But community support became the norm, and the paraprofessionals were providing the maximum amount of services, whether they were needed or not,” he said. “The money drove everything. Overutilization of community support meant other services weren't developed.”
Now the division requires preauthorization for services other than outpatient treatment and requires national accreditation for providers to weed out the marginally qualified.
“We've seen a decrease in the use of community support and increase in other services,” said Lancaster. He pushed in 2004 for the state to stop divesting the public system and halt the outflow of professionals, but the process was hard to stop, he said.
Legislative support will help. The state now offers psychiatrists a tuition-loan repayment program even if they are not working in federally approved health professional shortage areas. Lawmakers authorized funds last spring for 30 mobile treatment teams, 30 psychiatrists, and 30 walk-in clinics, along with expanded telepsychiatry services. Money has been allocated to develop inpatient beds in community hospitals, said Lancaster.
Perhaps because they have no other choice, most observers of the system hold out hope that the future will bring needed improvements.
“There are many naysayers who feel the system is irrevocably broken, but I don't feel that way,” said Swartz. The legislature has made a“ down payment” to get the system back on its feet, he said, while consumers, professionals, and others continue to pressure the politicians.
“I'm less concerned about the 'why' than in moving forward and ensuring that there is an accountability mechanism now,” said Smith.
Dihoff expects consolidation of the local management entities and consequent improvement in efficiency, accompanied by development of family- and peer-support approaches.
“We have funding now for clinics and mobile teams, although they will take two years to put in place,” said Lancaster. “We want to improve recruitment and retention, move treatment closer to home and families, and have institutions focus on the most severe cases.”
Information about the North Carolina Division of Mental Health, Developmental Disabilities, and Substance Abuse Services and its programs is posted at<www.ncdhhs.gov/mhddsas/>.▪