Children with autism and children with fragile X syndrome display some of the same cognitive and behavioral symptoms such as language impairment, deficits in social interactions, and rigid, repetitive patterns of behavior. Moreover, a number of children with fragile X syndrome meet full criteria for autism. Thus one might ask: Do youngsters with autism and those with fragile X also share the same brain abnormalities?
Apparently not, researchers have found in a study reported online November 1, 2010, in the Archives of General Psychiatry. The lead researcher was Fumiko Hoeft, M.D., Ph.D., an instructor in psychiatry and associate director of neuroimaging applications at Stanford University.
The study cohort included 165 boys aged 1 to 4—63 with autism, 52 with fragile X, and a control group of 50 children (31 typically developing and 19 with delayed development). MRI was used to view the subjects' brains and to compare the brain patterns of the three groups.
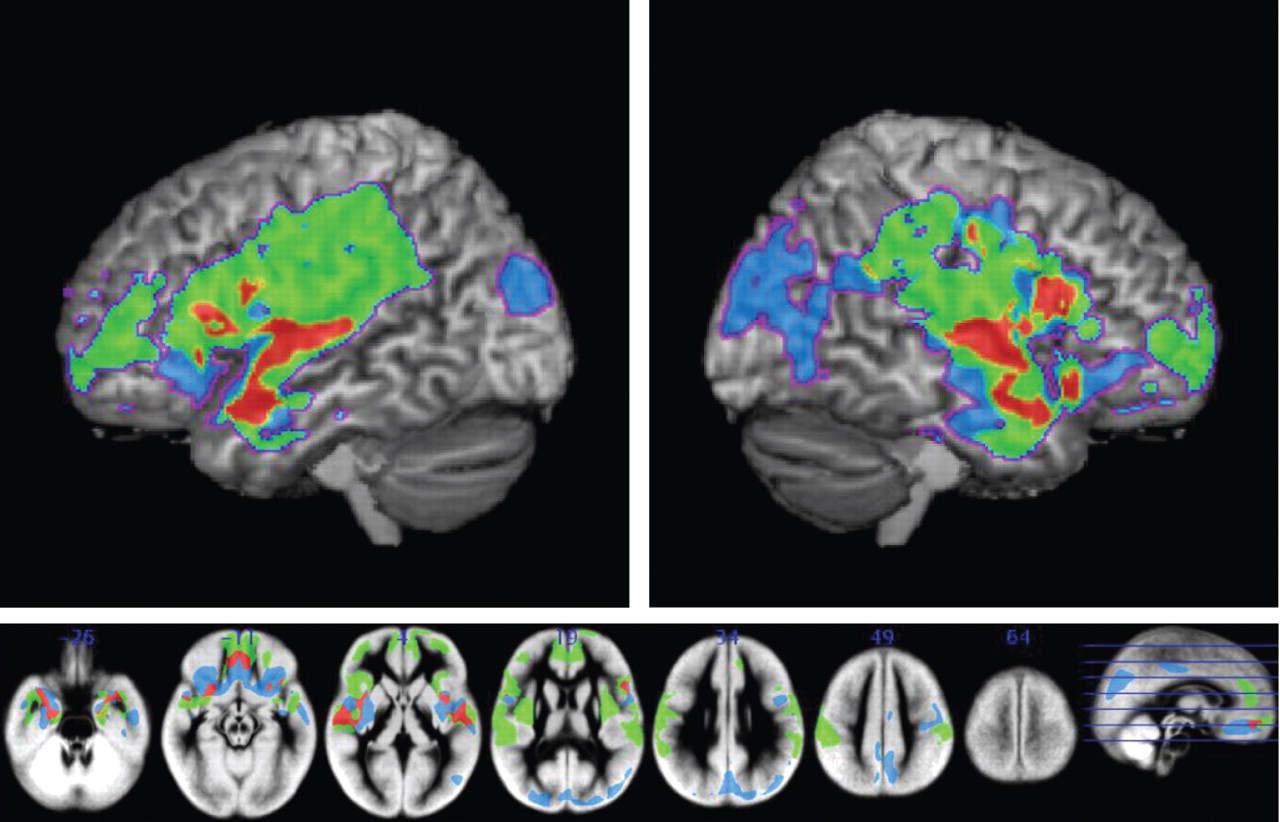
The frontal and temporal gray and white matter regions often implicated in social cognition were aberrant in the autism and fragile X groups compared with the control group. However, these differences were in opposite directions for the fragile X and autism groups relative to the control group. In general, greater volume was seen in the autism group than in the control group, whereas the control group in turn had greater volume than the fragile X group did. In general, the overall brain structure pattern of autism subjects resembled that of controls more than the brain structure of fragile X subjects did.
The finding that in spite of their shared cognitive and behavioral symptoms, children with autism and children with fragile X syndrome possess distinct neuroanatomical profiles surprised Hoeft. “I was expecting to find similar structural brain patterns,” she told Psychiatric News.
The results may have clinical implications, she also pointed out. “People often try to use symptom-specific treatments and sometimes similar treatments for fragile X and autism. If one day we can use this brain imaging information to tailor treatment for each disorder and even each individual, then it may be more effective.”
Hoeft said she is now “hoping to identify ‘novel’ subtypes in these disorders that may, for example, predict outcome, but aren't that obvious by looking just at patterns of behavior or other external and currently available measures.”
The new findings may also lead to a better understanding of the neurodevelopmental pathways in autism and fragile X syndrome, Hoeft and her colleagues noted in their study report. For example, the fragile X syndrome is known to be due to the absence of a particular gene—the FMR1 gene—on the X chromosome. Researchers might eventually be able to determine how the missing gene could lead to the abnormal brain patterns identified in children with fragile X syndrome.
The study was funded by the National Institutes of Health, NARSAD, and the Canel Family Fund.