A link between several types of psychotropic medications and violent behavior toward others has been documented in a recent study.
The medications most strongly linked to violent behavior were the smoking-cessation aid varenicline and antidepressants, regardless of class.
The association was made by Thomas Moore, Joseph Glenmullen, M.D., and Curt Furberg, M.D., Ph.D. Moore is a senior scientist for drug safety and policy at the Institute for Safe Medication Practices (ISMP) in Horsham, Pa. The ISMP is a nonprofit organization that educates health care providers and the public about safe medication practices. Glenmullen is a clinical instructor of psychiatry at Harvard Medical School, and Furberg is a professor of public health sciences at Wake Forest University.
In a study published in the December 15, 2010, PloS One, the researchers used 2004 to 2009 data from the Food and Drug Administration (FDA) Adverse Event Reporting System. They found that during the study period, 780,169 serious adverse events of one kind or another had been reported for 484 drugs, and that of those serious adverse events, 1,937 had been acts of violence. They defined a violent event as any case report containing one or more of the following items: homicide, physical assault, physical abuse, homicidal ideation, or violence-related symptom, but not more ambiguous descriptions such as crime, aggression, belligerence, or hostility.
The researchers then set out to see whether any of the 484 drugs had been disproportionally linked with the acts of violence. To be “disproportionally linked,” a drug had to be associated with at least five cases of violence, to have at least twice as many cases of violence associated with it as expected given the volume of overall adverse events reported for it, and statistical analysis had to indicate that the violence cases associated with it were unlikely to have occurred by chance.
The researchers found that 324 of the 484 drugs (67 percent) had no link with violence cases and that 86 of the drugs (18 percent) had links with only one or two cases of violence. However, 31 of the drugs (6 percent) were found to be disproportionally linked with violence cases. These drugs included varenicline, 11 antidepressants, three drugs for attention-deficit/hyperactivity disorder, and five hypnotics/sedatives.
Moreover, of the 484 drugs evaluated, varenicline had the largest number of violence cases, the highest proportion of violence cases (PRR = 18.0), and the highest statistical probability that the violence cases associated with it were not by chance (x2 = 5,172df = p<0.01).
Thus “varenicline had the strongest association with violence by every measure used in this study,” Moore and his colleagues pointed out. “In addition, antidepressant drugs showed consistently elevated risk, even when compared with antipsychotics and mood stabilizers. . . .”
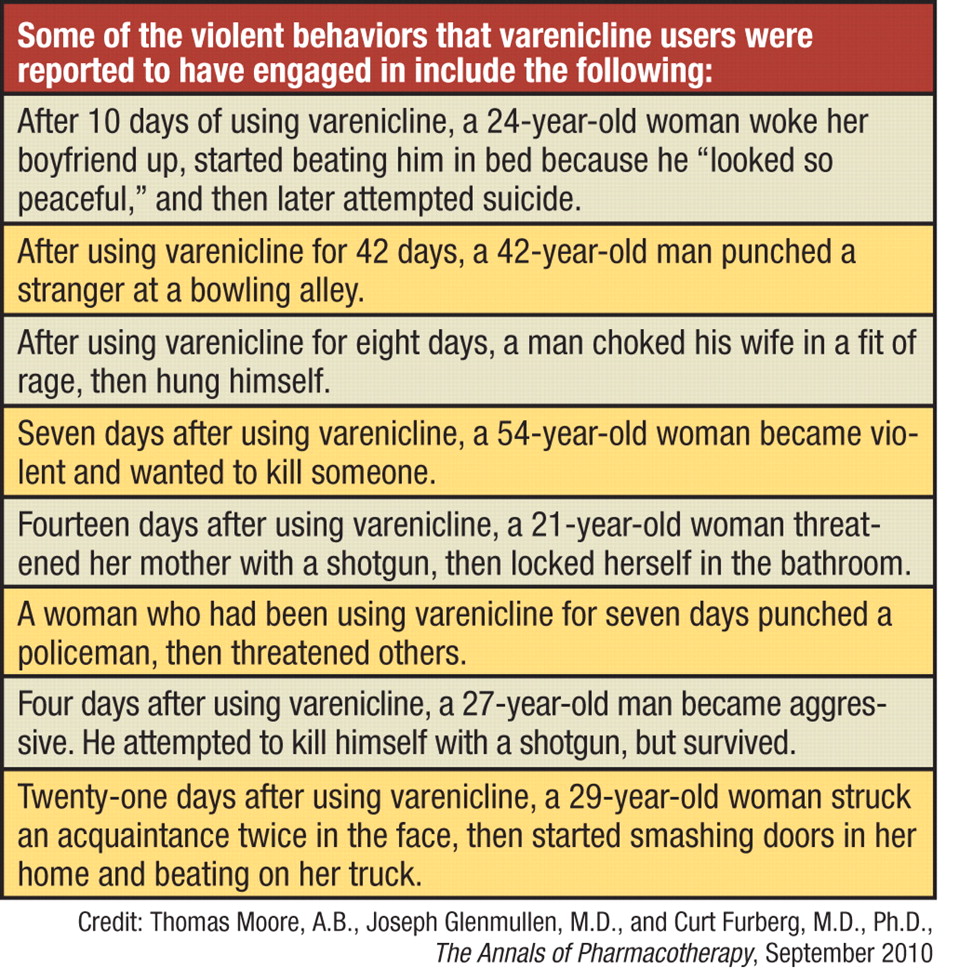
Just because these drugs have been linked with cases of violent behavior does not prove that they actually promoted such behavior. Yet some of the varenicline-linked violence cases that Moore and his colleagues scrutinized suggested to them that there might be a causal connection. For example, the individuals in question started displaying psychiatric symptoms a few days after they had begun taking varenicline. They appeared to direct their violence senselessly, that is, at anybody who happened to be near them, and once they stopped taking varenicline, they stopped engaging in violent acts.
As Moore told Psychiatric News, both an earlier study his research group conducted and one by FDA researchers “noted that the onset of adverse effects for varenicline frequently occurs before the subject stops smoking,” implying that it is varenicline, not nicotine withdrawal, that prompts violent behavior. Still another reason to believe that it is the medication, not nicotine withdrawal, that leads to violent behavior is that “varenicline has a seven-day dose-escalation period prior to setting a target date to stop smoking,” Moore noted.
This study is “a preliminary review of adverse events . . . that indicate a risk of violence toward others,” Darrel Regier, M.D., M.P.H., director of APA's Division of Research and executive director of the American Psychiatric Institute for Research and Education, told Psychiatric News. “[Also the findings come] from a historically difficult database to interpret—FDA adverse event data. . . . There is clearly a need to conduct prospective studies [to see whether the findings can] be confirmed. The same was true for the proported risk of suicidality associated with antidepressants.”
“This seems to be a reasonably good study with a high number [of medications evaluated] and a lot of double-checking,” Paul Fink, M.D., an expert in the study of violent behavior and a past APA president, commented. “I can tell you that as a psychiatrist who has practiced for a long time, I was unaware that [varenicline and antidepressants] had been linked with violence toward others. . . . Psychiatrists and mental health professionals need to be aware of this association.”
The study had no outside funding.