Several studies conducted since the 1980s have demonstrated the efficacy of psychoeducational family interventions for the treatment of schizophrenia. For patients whose families received these interventions, the relapse rate at one year ranged from 6 to 12 percent, compared with 41 to 53 percent for patients who received routine care (
1,
2,
3 ). At two years the relapse rates were 17 to 40 percent for the intervention groups, compared with 66 to 83 percent for the control groups. Recent meta-analyses have shown that among patients with schizophrenia whose families receive psychoeducational interventions, relapse rates are reduced fourfold at one year and twofold in the subsequent year, compared with rates for patients who receive usual care (
4,
5 ). In addition, research findings are consistent with the possibility that these interventions reduce the disability of patients with schizophrenia (
6,
7,
8 ) and ameliorate family burden (
9,
10,
11 ).
Differences in clinical outcome between usual treatment for schizophrenia and treatment that includes psychoeducational interventions are so impressive that, as pointed out by McFarlane and colleagues (
2 ), "they are some of the most substantial and consistent empirical effects achieved by any treatment in the mental health field." Even though a large number of randomized controlled trials have examined the effectiveness of psychoeducational interventions, very few studies have looked at the impact on clinical and social outcomes of patients with schizophrenia of psychoeducational interventions provided in real-world settings by ordinary staff (
7,
12,
13,
14,
15 ). Therefore, it is not clear to what extent these interventions are able to ameliorate patients' disability (
6,
8,
16 ) when they are provided in clinical settings or to what extent the interventions are able to reduce the burden of care and improve the relationships between service users, their families, and mental health service providers (
17 ).
In this article we present the results of the second phase, which was aimed at exploring the impact of the intervention on patients' personal and social functioning and relatives' burden and perceived support.
Results
Sample description
The 34 professionals from 17 public mental health centers (14 psychiatrists, ten nurses, three psychologists, four rehabilitators, and three social workers) selected 71 families of consumers with schizophrenia, of which 42 were randomly allocated to the intervention group and 29 were assigned to the control group.
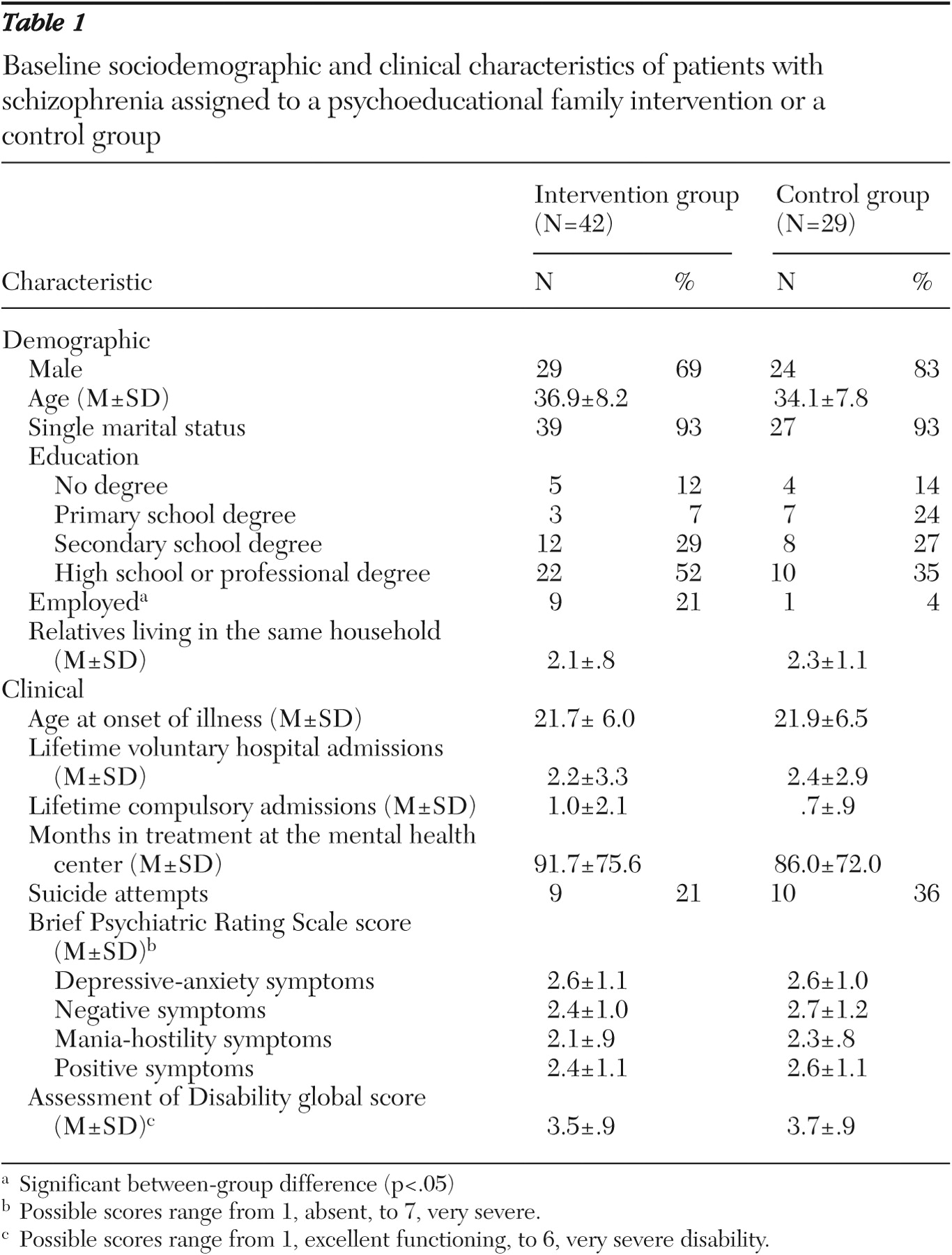
Patients' sociodemographic and clinical characteristics at baseline are reported in
Table 1 . For both groups of patients, the average score on the BPRS subscales corresponded to a mild level of symptoms and the AD global score corresponded to moderate-marked impairment in social and occupational functioning.
In the six months before the study, 11 patients in the intervention group (26 percent) had attended information sessions on schizophrenia and psychotropic drugs, 12 (29 percent) had received individual psychotherapy, and 22 (52 percent) had participated in a rehabilitative program. The respective figures for the control group were nine (31 percent), eight (28 percent), and 16 (55 percent). All patients were taking antipsychotic drugs.
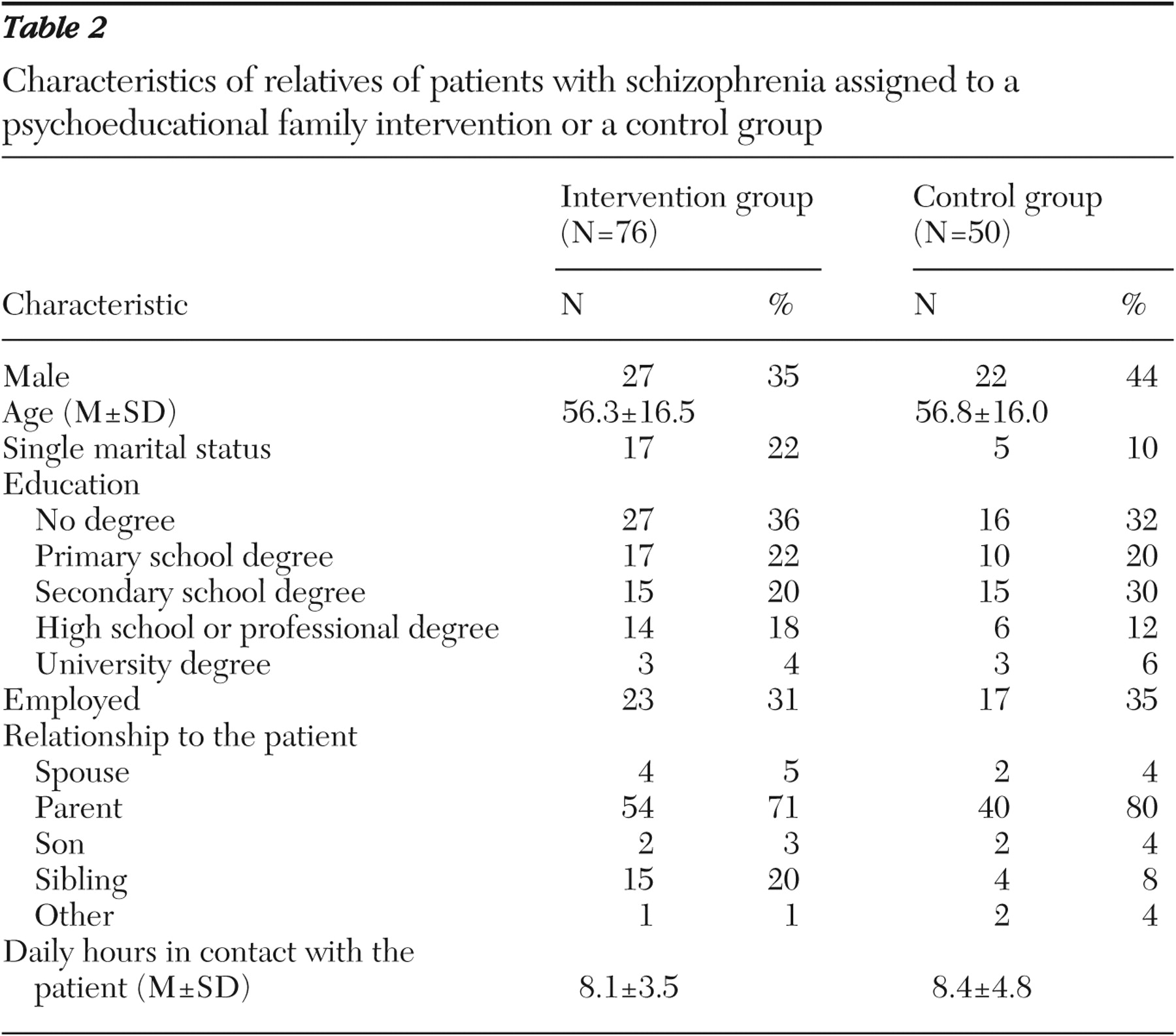
Patients' relatives were mostly parents or siblings. As shown in
Table 2 in one-third of cases they were currently employed. In the six months before the study, 45 relatives (59 percent) in the intervention group and 30 relatives (60 percent) in the control group had attended supportive meetings with professionals, and 18 (24 percent) and 21 (42 percent), respectively, had participated in information sessions on schizophrenia and drug treatment.
The only statistically significant difference at baseline between the two patient groups was in employment status—nine patients in the intervention group (21 percent) were employed, compared with one patient (4 percent) in the control group ( χ 2 =4.5, df=1, p<.05).
Attrition rate
In the intervention group six of the 42 families (14 percent) left the study. In three cases relatives cited lack of time or interest, in one case a family member experienced a psychotic breakdown, in another case the family believed that the treatment was too demanding for the patient, and in another case the patient died from a physical illness. The families who dropped out differed from the other families only in regard to patients' mean±SD score on the BPRS mania-hostility subscale, which was significantly higher for those who dropped out (2.9±1.5 compared with 2.0±.7; F=6.5, df=1 and 40, p<.02).
In the control group three of the 29 families (10 percent) refused the six-month evaluation. In two cases the families moved to other geographic areas, and in one case the patient refused despite having previously agreed to the follow-up assessment. The families who did not participate in the follow-up differed from those who did in the number of hours of close contact with the patient, which was higher among the families who did not participate (13.8±6.2 compared with 7.7±4.2 hours; F=10.1, df=1 and 48, p<.003).
Outcome measures at six months
Thirty-six patients in the intervention group completed the 18 sessions required over the six-month period. In the control group, 26 patients were reassessed at six months. Medication dosages for these groups during the study period were as follows: haloperidol, 12 patients in the intervention group (33 percent) and four in the control group (15 percent) (mean dosages of 4.2±2.5 and 3.8±1.6 mg); for risperidone the respective figures were eight (22 percent) and seven (27 percent) (3.2±2.3 and 4.1± 1.4 mg); for olanzapine, eight (22 percent) and four (15 percent) (19.4±8.6 and 12.5±6.4 mg); for clozapine, six (17 percent) and four (15 percent) (300±151.6 and 337.5±205.6 mg); for fluphenazine, three (8 percent) and three (12 percent) (1.0±.2 and 2.2± 2.4 mg); and for quetiapine, three (8 percent) and one (4 percent) (533.3± 230.9 and 800.0 mg). In the control group three patients (11 percent) received chlorpromazine (31.7±16.1 mg) and one patient (4 percent) was treated with perphenazine (5.0 mg).
In regard to psychological interventions, nine patients in the intervention group (25 percent) and three in the control group (12 percent) received individual psychotherapy; for group therapy, the respective figures were four (11 percent) and two (8 percent). In addition, ten patients in the intervention group (28 percent) and nine in the control group (35 percent) received social skills training; the respective figures were 14 (39 percent) and six (23 percent) for participation in a socialization group.
Compliance with interventions was rated regular for 31 patients in the intervention group (94 percent) and 23 in the control group (96 percent).
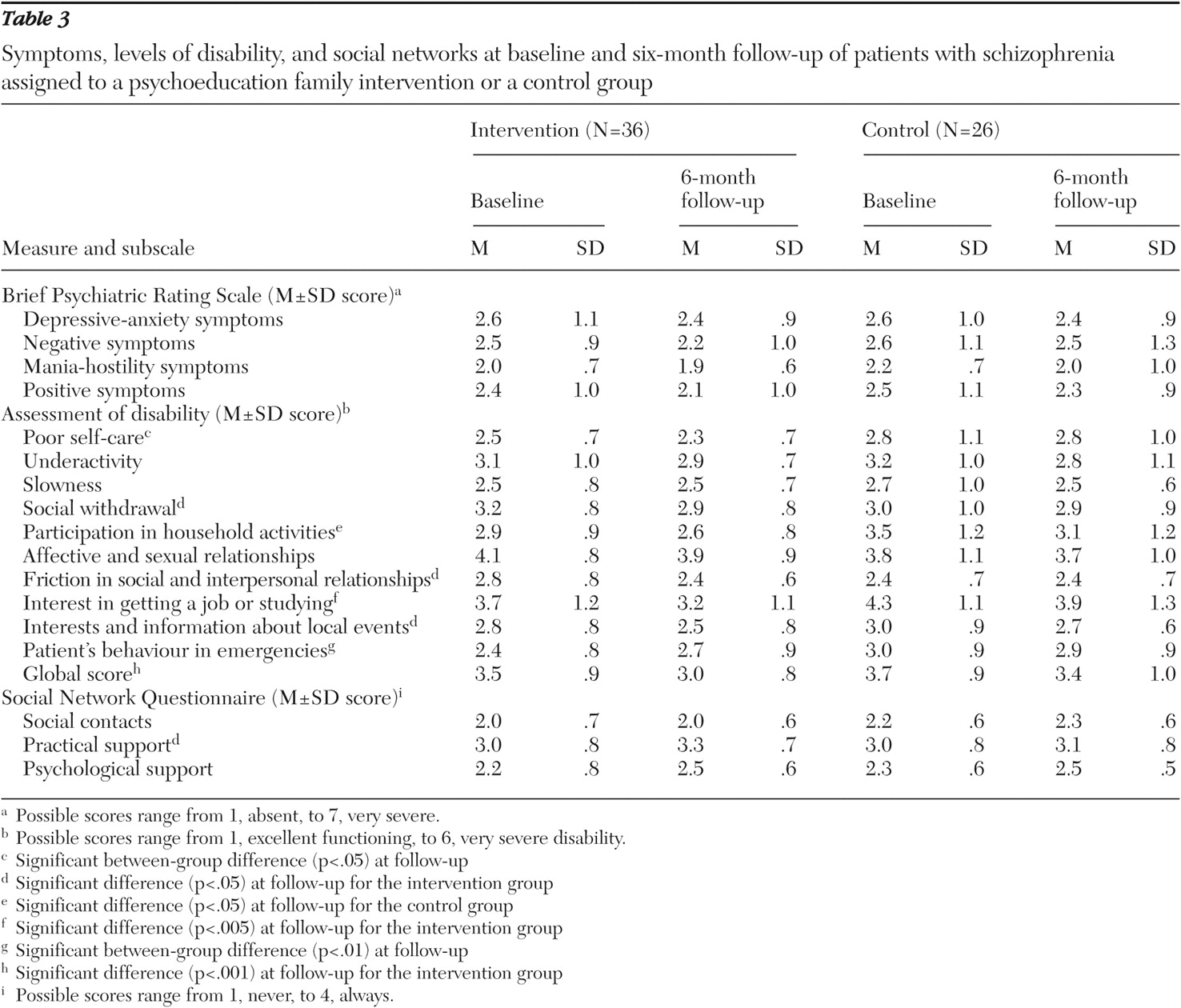
At follow-up, compared with patients in the control group, those in the intervention group demonstrated lower levels of disability in self-care (F=5.4, df=1 and 60, p<.05) and in behavior in emergencies (F=7.1, df=1 and 57, p<.01). In the intervention group, a statistically significant improvement was found in global levels of disability, as well as in social withdrawal, interest in getting a job or studying, social interests, and management of friction in social and interpersonal conflicts (
Table 3 ).
In the intervention group, 17 patients (47 percent of those followed up) had poor or very poor global functioning at baseline, compared with nine (25 percent) at follow-up (z= -3.3, p<.001). Social withdrawal was either moderate or severe for 13 patients (36 percent) in the intervention group at baseline, compared with seven (19 percent) at follow-up (z=-2.1, p<.03). Difficulties in managing friction in social and interpersonal relationships were noted for seven patients (19 percent) in the intervention group at baseline and for two (5 percent) at follow-up (z=-2.4, p<.01). Difficulties in maintaining interests were found for 23 patients (64 percent) in the intervention group at baseline and for 14 (39 percent) at follow-up (z=-2.0, p<.05).
In the intervention group, 27 patients (75 percent) stated at follow-up that their social relationships had improved during the previous six months, whereas at baseline 21 patients (58 percent) reported such improvement (z=-2.1, p<.03). In addition, 29 patients in the intervention group (82 percent) felt that they had someone to take care of them in case of illness at follow-up, compared with 23 patients (63 percent) at baseline (z=-3.07, p<.002).
In the control group, the only statistically significant improvement in patients' personal or social functioning was in participation in household activities, which was very poor for six patients (23 percent) at baseline and for four (15 percent) at follow-up (z=-2.0, p<.05).
Family burden, social network, and professional support
Fifty-seven relatives in the intervention group completed the 18 sessions required over the six-month period. In the control group, 43 relatives were reassessed at six months. As shown in
Table 4, at follow-up the average level of family burden significantly improved in both the intervention and control groups. In the intervention group, 29 relatives (51 percent) reported having had to always or often neglect their own hobbies at baseline, compared with 12 (21 percent) at six months (z=-2.6, p<.01). Twenty-six relatives (46 percent) in the intervention group reported crying and feeling depressed at baseline, compared with 16 (28 percent) at follow-up (z=-2.5, p<.02), and 32 (56 percent) reported being worried about the future of other family members at baseline, compared with 22 (39 percent) at follow-up (z=-2.4, p<.02). Twelve relatives (21 percent) in the intervention group reported at baseline feeling embarrassed when they were in public places with the patient, and five (9 percent) reported such feeling at six months (z=-3.4; p<.001).
In the control group 14 relatives (32 percent) reported at baseline that they had to neglect their own hobbies, compared with 12 (28 percent) at follow-up (z=-2.0, p<.05), and ten (23 percent) reported having to neglect their job activities at baseline, compared with three (7 percent) at follow-up (z=-3.0, p<.003). Fifteen relatives in the control group (35 percent) felt unable to bear the situation any longer at baseline, compared with nine (21 percent) at follow-up (z= -2.1, p<.04), and 20 (47 percent) reported worrying about the future of other family members at baseline, compared with 13 (30 percent) at follow-up (z=-2.6, p<.008).
Relatives' social contacts and perceived help in emergencies involving the patient significantly improved in the intervention group. At follow-up 25 relatives (44 percent) stated that they had been contacted by relatives and friends, compared with 15 (26 percent) at baseline (z=-2.9, p<.003), and 31 (54 percent) reported that they could rely on friends in critical situations at follow-up, compared with 22 (39 percent) at baseline (z=-2.4, p<.02). Moreover, 25 relatives (44 percent) reported a significant improvement in social relationships in the previous six months at follow-up, compared with ten (18 percent) at baseline (z=-2.3, p<.02).
In the control group practical social support significantly improved over the six-month period. In particular, 23 relatives (53 percent) stated at follow-up that they could rely on someone for demands, compared with 16 (37 percent) at baseline (z=-.2.8, p<.005).
Relatives' perception of the level of professional support significantly increased only in the intervention group. In particular, 53 relatives (93 percent) stated at follow-up that they had received information by professionals on how to cope with patients' disturbing behavior, compared with 37 (65 percent) at baseline (z=-4.4, p<.001). Twenty-four (42 percent) felt confident about receiving professional help in case of emergencies, compared with 16 (28 percent) at baseline (z=-2.5, p<.01), and 53 (93 percent) reported a high level of professional help provided to the patient by psychiatrists at follow-up, compared with 48 (84 percent) at baseline (z=-2.0, p<.04).
Discussion
This is the first controlled trial in a routine clinical setting of a psychoeducational family intervention for schizophrenia carried out in Italy. An important feature of the study was the random allocation of the families to an intervention or a control group. The adoption of a waiting list led to a condition similar to clinical routine and ensured that all recruited families received the intervention in a reasonable period.
The intervention was implemented by two professionals at each center who had limited expertise in behavioral family interventions (
19 ), which reflects the limited resources currently available in Italy to implement evidence-based treatments in clinical settings. Such limitations make it very difficult to train a majority of mental health professionals in these interventions. The high level of staff attendance suggests that a modular training program could facilitate the dissemination of psychoeducational intervention in routine clinical settings when the professional resources are scarce.
The inclusion criteria—a
DSM-IV diagnosis of schizophrenia and cohabitation with one adult relative—permitted recruitment of a broad sample. In addition, patients with co-occurring conditions, such as alcohol or drug abuse and physical illness, were not excluded. Thus the sample was representative of the heterogeneity of patients with schizophrenia in Italy (
21 ).
The study focused on the impact of the intervention on functional outcomes of schizophrenia, in particular patient's personal and social functioning and social network. Such a focus addresses a frequently emphasized weakness of clinical trials involving patients with schizophrenia, which often use relapse as the outcome variable, whereas consumers and their families are more concerned about such issues as housing, employment, and social relationships (
25,
26,
27,
28 ).
The well-validated assessment tools were administered by the same professionals who provided the intervention. In real-world trials, this is not regarded as detrimental, because it guarantees a condition more similar to clinical routine, where professionals are expected to evaluate their own clinical work (
26,
27 ). It should also be noted that most of the instruments used in the study were self-administered.
The main limitations of the study are the small sample and the relatively brief period of follow-up, which has prevented us from assessing the impact of the intervention on other outcome variables, such as return to work or achievement of independent life goals. The most impressive result of the study is the significant reduction in levels of personal and social disability among the patients, especially in interests and social relationships. This result, in line with those reported in randomized controlled trials by Montero and colleagues (
8 ) and Falloon (
6 ), may be at least partly related to the identification of individual goals that could reasonably be achieved in a few months, which in most cases concerned social activities; the focus on communication skills in family sessions; and the active involvement of family members in the management of the patient's disorder. As pointed out by Liberman and Liberman (
29 ), psychoeducational family interventions can be regarded as rehabilitative because they provide all family members, including the patient, with knowledge, skills, and support to function better in daily life and to achieve their own personal goals.
A significant improvement was observed in family burden in both the intervention and control groups. This improvement is in contrast with data reported by Mueser and colleagues (
1 ), Canive and associates (
30 ), and McDonnell and coauthors (
31 ), who found no reduction of burden in treated families compared with families in the control groups. The previous findings may be a result of special attention paid to families' needs by professionals in both the intervention and control groups as well as to the expectations about forthcoming treatment among families in the control group. Understanding the impact of the intervention on family burden and social resources will require long-term investigations.
In the intervention group the percentage of relatives who reported feeling embarrassed when they were in public places with the patient decreased significantly, from 21 to 8 percent at follow-up. This finding suggests a specific effect of the intervention on stigma perceived by the relatives, which may be related to improvement in the patient's competence and to information provided to relatives about the clinical characteristics and outcome of schizophrenia.
Another interesting finding is the significant increase in relatives' perception of professional support only among families who received the intervention. This finding reflects improvement in relationships with consumers and their families reported by the professionals, which is considered among the main advantages of the use of the psychoeducational intervention (
15,
19 ).
Conclusions
The results of this study suggest that psychoeducational interventions may have a significant impact on functional outcomes of schizophrenia, even when they are provided to patients and caregivers recruited in a real-world service setting. Further studies are needed to address additional issues, such as the long-term effects of psychoeducational interventions on the quality of life of persons with schizophrenia and their relatives.
Acknowledgments
This study was supported by grant 2-18-8 from the M. Lugli Foundation and from grant 1AL-F3 from Italy's National Institute of Health. The Family Intervention Working Group includes the following mental health center professionals: Michele Di Lella, M.D., Elisabetta Biscussi, Francesco Degl'innocenti, M.D., Rossella Bellini, Barbara Scandone, M.D., Matteo Folla, Emi Bondi, M.D., Giuseppina Robustelli Test, Luisa Gargiulo, M.D., Aniello Esposito, Francesco Bardicchia, M.D., Gennaro Cerullo, Grazia Favata, Annarita Sasso, Luisa Maresca, M.D., Giovanna Cavaliere, Vincenzo Delcuratolo, M.D., Maria Giannini, Luigi D'Ambra, M.D., Anna Malacarne, Floralba Gentile, Lucetta Casale, Mauro Raffaeli, M.D., Paola Innocente, Rosa Salmeri, M.D., Rosario Cantone, Mario Scordato, M.D., Graziella Campo, Riccardo Curreli, M.D., Silvana Miscali, Rita Di Nunzio, M.D., Lucia Matrella, Laura Pezzenati, Monica Prezioso, Stefania Lucania, M.D., Angela Scorzino, Cinzia Mameli, and Carla Sodde. The authors are grateful to Itzhak Levav, M.D., M.S., for comments on the initial draft.