Addiction Severity Index composite scores
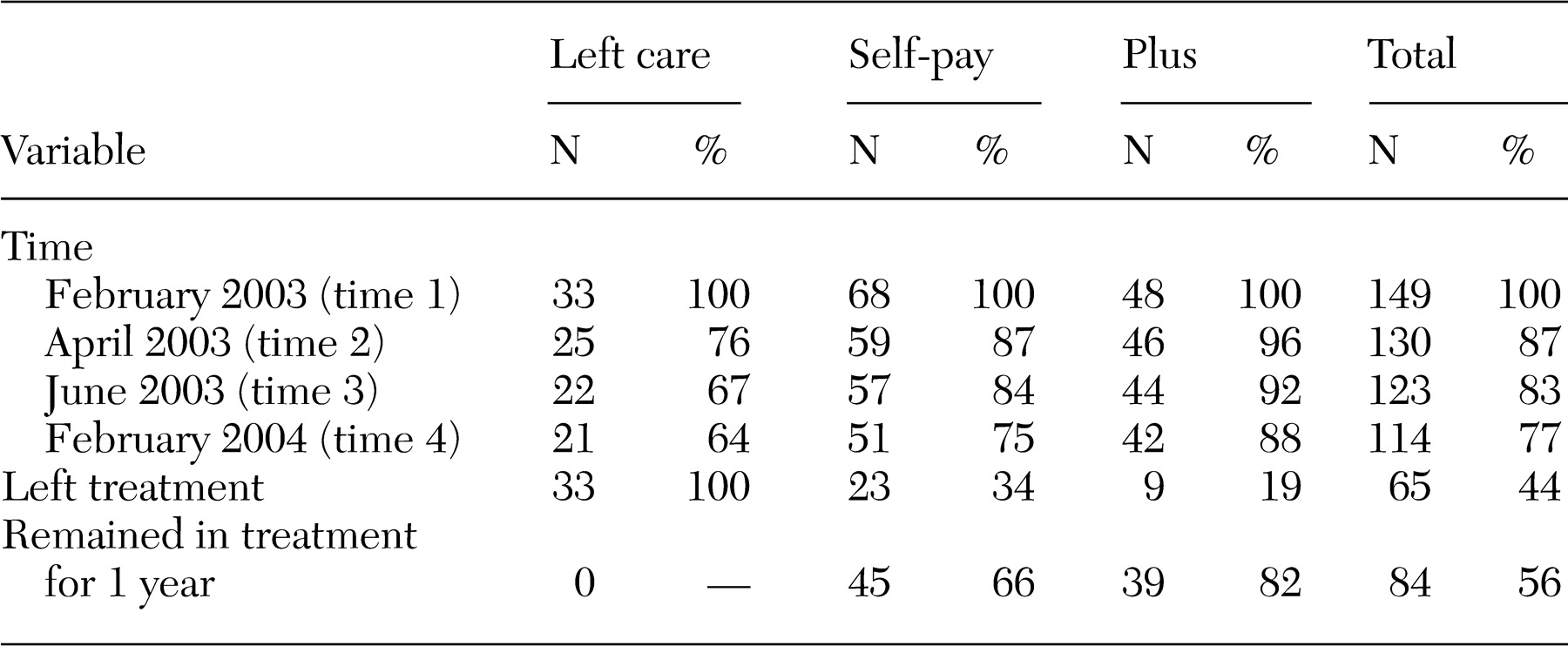
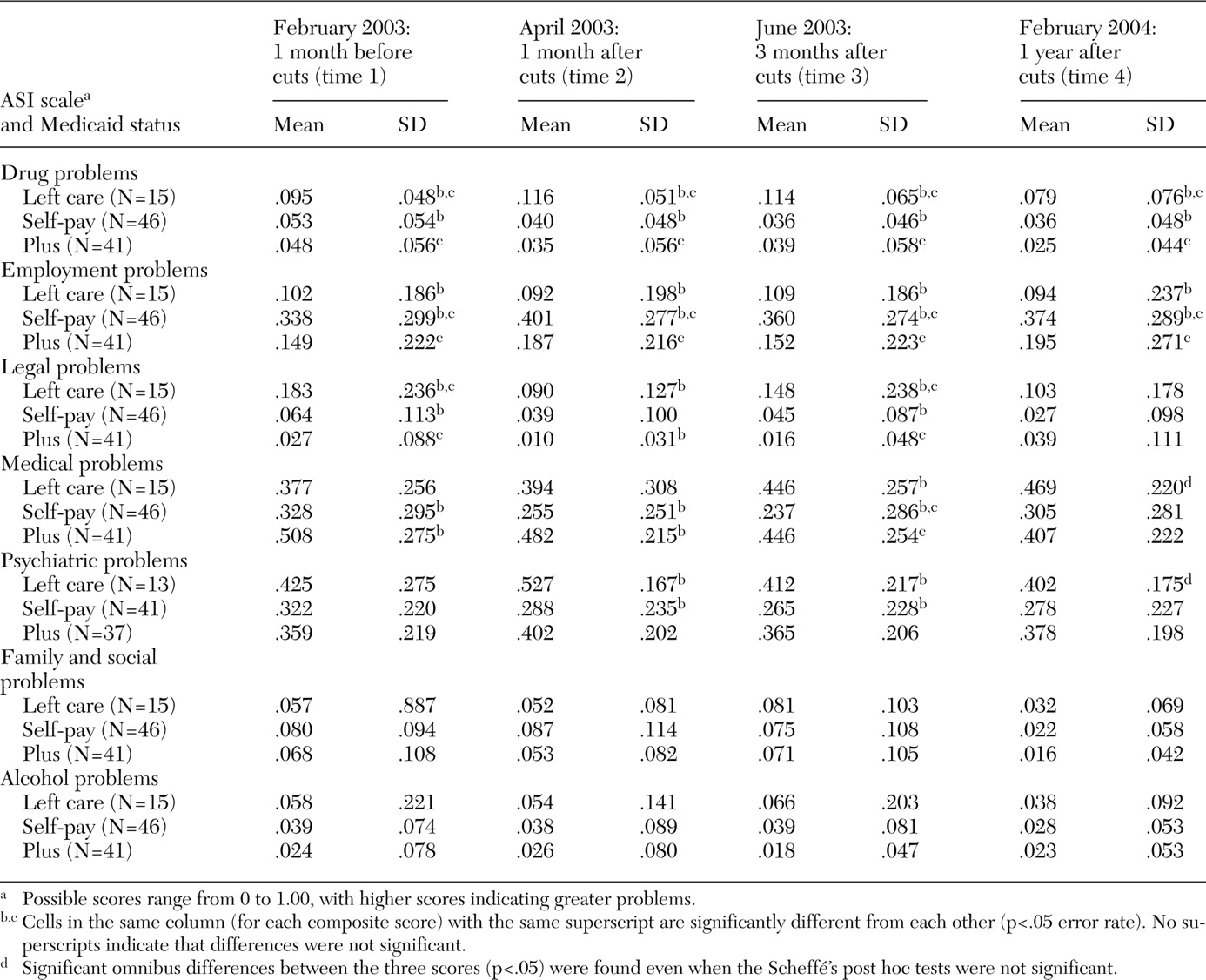
Table 2 presents the ASI composite scores by Medicaid group. A multivariate analysis of variance (MANOVA) examined the significance of three effects: a Medicaid effect (a between-participants effect examining differences across Medicaid groups), a time effect (a within-participants effect examining increases or decreases over time), and a Medicaid group by time interaction (rates of change differing by group). Four univariate tests and the post hoc analyses were performed with a controlled type I error rate of .05 for each composite score. Participants with complete data at all four time points for each scale were included in the analysis (15 in the left-care group, 46 in the self-pay group, and 41 in the Plus group). Some data were missing on the psychiatric subscale for 11 participants.
The most pronounced differences were seen in the drug problems composite score. A multivariate effect was observed for time (Wilks' lambda=.900; F=3.59, df=3, 97, p=.016), indicating a decline in drug problems over the year: time 1, mean score of .057±.056; time 2, mean score of .049 ±.058; time 3, mean score of .049±.060; and time 4, .038±.054. A significant multivariate Medicaid group difference was observed (F=17.40, df=3, 99, p=.001). No significant time by Medicaid group interaction was found. Mean scores suggest that the left-care group had greater drug problems over the full year than the other two groups. Drug problems for this group were higher than those of the other two groups at time 1 because they were being detoxified from methadone. These scores increased at times 2 and 3 before decreasing at time 4. Even though some patients reported using alcohol to ease their withdrawal symptoms, the alcohol problems composite score was not affected significantly by time or Medicaid group.
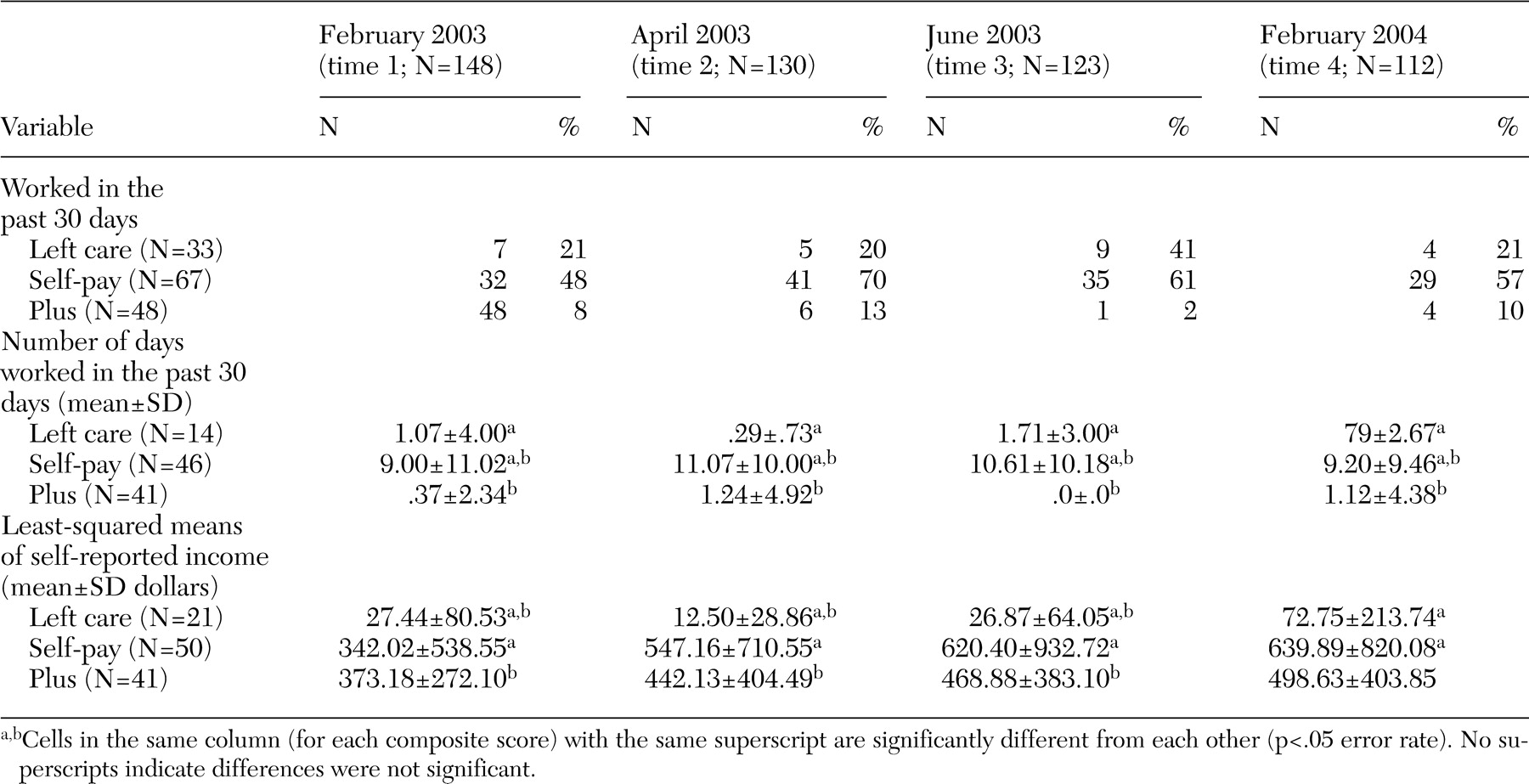
The multivariate repeated-measures effect for the employment problems composite score showed no significant time or interaction effects. A significant multivariate Medicaid group difference was found (F=11.39, df=2, 99, p<.001), suggesting that for the four points in time there was a difference in the overall level of employment problems between the three groups. Patients who chose to pay out of pocket reported greater problems with employment than those in the left-care group or those covered by Plus. This finding suggests that employment was a major cause for concern among those attempting to pay the $300 per month for methadone treatment.
For the legal problems composite score, a significant multivariate difference was observed for time (Wilks' lambda=.860; F=5.40, df=3, 97, p=.002; time 1, mean score of .067±.138; time 2, mean score of .035±.088; time 3, mean score of .048±.119; and time 4, mean score of .043±.119) as well as a significant Medicaid group effect overall (F=9.94, df=2, 99, p=.001). There was a trend-level (p=.08) Medicaid by time interaction effect. At time 1, the left-care group reported more legal problems than the self-pay and Plus groups. The greater number of legal problems resulted from patients in the left-care group being more likely than those in the other two groups to be homeless and to have increased illegal activity. At times 2 and 3 the significant differences were between the left-care and the Plus groups. At time 4 no observable difference between the Medicaid groups was detected.
A significant multivariate repeated-measures effect for the family and social problems composite score was observed (Wilks' lambda=.789; F=8.64, df=3, 97, p=.001), indicating a decrease over time (time 1, mean score of .071±.099; time 2, mean score of .068±.098; time 3, mean score of .074±.105; and time 4, mean score of .021±.054). The greatest decrease was between times 3 and 4, indicating that during the period when methadone benefits were eliminated, patients reported strain in familial and social relationships. At one year, these issues appear to have resolved as the patient's social network adjusted to the changes.
No significant multivariate time effect or an interaction was found for the medical problems composite score, indicating that no systematic increase or decrease was observed. A significant multivariate Medicaid group difference was found (F=9.17, df=2, 99, p<.001). Scheffé's post hoc comparison tests suggest differences between the self-pay and the Plus groups. In the first four months after losing benefit coverage, patients who self-paid reported fewer medical problems than those in the Plus group. Patients in the Plus group had more medical problems than those in the other two groups, probably because many patients in the Plus group met qualifications for additional benefits because of disability.
A significant multivariate time effect was observed for the psychiatric problems composite score (Wilks' lambda=.856; F=6.26, df=3, 112, p=.001): time 1, mean score of .352±.228; time 2, mean score of .369±.227; time 3, mean score of .327±.223; and time 4, mean score of .336±.213. Psychiatric problems peaked at times 1 and 2 and then ameliorated somewhat at times 3 and 4. No time by Medicaid group effect was observed, but a significant Medicaid group effect was found (F=3.68, df=2, 114, p<.028). Significant differences were observed between the left-care group and the self-pay group. Patients in the self-pay group were more psychologically stable than those in the left-care group. Time 2 (one month after detoxification) showed the largest difference between the left-care group and the self-pay group. By time 4, the differences were not significant.
Risk behaviors and treatment seeking
Significantly more people in the left-care group (five of 20 patients, or 25 percent) reported injecting with previously used syringes than in the self-pay group (three of 51 patients, or 6 percent) or the Plus group (one of 42 patients, or 2 percent). Over the year, nine of 20 patients in the left-care group (45 percent) were homeless. This proportion was significantly higher than that found in the self-pay group (12 of 51 patients, or 24 percent) or the Plus group (one of 42 patients, or 2 percent) (F=9.52, df=2, 110, p<.001). Homelessness (and continued drug use) complicated patients' ability to find employment and stable housing.
Data from the Time Line Follow Back assessment indicated that patients in the left-care group attended fewer individual drug abuse counseling sessions than those in the other two groups. Patients in the left-care group attended individual substance abuse counseling on an average of 4.05±3.82 months over the year, whereas those in the self-pay group attended sessions for a mean of 7.39±5.03 months and those in the Plus group attended sessions for a mean of 8.86±4.59 months (F=7.15, df=2, 110, p=.001). The same results were found for group therapy (F=7.75, df=2, 110, p=.001); patients in the left-care group attended therapy for a mean of 4.00±3.85 months out of the year, whereas those in the self-pay and Plus groups attended sessions for 8.57±4.59 and 8.81±5.05 months out of the year, respectively.