Procedure
Participants were sampled from 11 residential drug abuse treatment programs that provided publicly funded treatment to adults within Los Angeles County from August 1999 to April 2002. Follow-up assessments were conducted through April 2003. Upon admission, individuals were screened by program staff for study inclusion by asking them whether they had a history of mental health or emotional problems or had ever received treatment or were currently seeking treatment for a mental health or emotional problem. Eligible patients were referred to research staff who then conducted study intake procedures, which included obtaining patients' informed consent for study participation.
Baseline assessments were conducted at least 48 hours after treatment admission to allow patients to stabilize. These interviews took approximately six hours to complete and usually were conducted in multiple sittings. Participants received payment of $40 for the interview in the form of noncash vouchers for local stores or restaurants. Face-to-face follow-up interviews (lasting an average of two to three hours) were scheduled with all participants at six months after admission for treatment; participants were paid $50 in noncash vouchers for completion of these interviews.
All study procedures were reviewed and approved by the University of California, Los Angeles (UCLA), Institutional Review Board. A federal Certificate of Confidentiality to protect subject confidentiality was obtained from the National Institute on Drug Abuse.
Participants
Participants were 400 adult men and women recruited from 11 residential drug treatment programs. The mean±SD age of participants was 36±8.4 years. There were 213 men (53 percent) and 187 women (47 percent). Of the total, 140 participants (35 percent) were African American, 176 (44 percent) were white, 52 (13 percent) were Hispanic, and 32 (8 percent) were of other ethnicities. Over half of the sample (211 patients, or 53 percent) had never been married, and one-third (133 patients, or 33 percent) had less than a high school education. Most of the sample (328 patients, or 82 percent) had been homeless, and most (236 patients, or 59 percent) had been under legal supervision in the past.
Participants were assessed on the Structured Clinical Interview for the DSM-IV Axis I Disorders-Patient Edition (SCID-I/P, version 2.0) (
47 ) for mood, psychotic, posttraumatic stress, and substance use disorders. Interviewers were trained to conduct the SCID by diagnosticians from the Diagnosis and Psychopathology Unit of the UCLA Center for Research on Treatment and Rehabilitation of Psychosis. Interviewers were required to achieve a minimum overall kappa of .75, a minimum sensitivity kappa of .75, and a specificity kappa of .75 on symptom agreement, and 90 percent accuracy of agreement on diagnosis (
48 ). Of the 400 participants, 255, or nearly two-thirds (64 percent) had a diagnosis of mood disorder (major depression, dysthymia, bipolar disorder, or mood disorder not otherwise specified [NOS]), and the remaining 143 (36 percent) were diagnosed as having a psychotic disorder (schizophrenia, schizoaffective disorder, or psychosis NOS). In addition, 208 (52 percent) were given a diagnosis of posttraumatic stress disorder.
Regarding lifetime substance use, 278 participants (70 percent) had a diagnosis of alcohol dependence; 260 (65 percent), cocaine dependence; 176 (44 percent), cannabis dependence; 168 (42 percent), amphetamine dependence; 115 (29 percent), opioid dependence; and 99 (25 percent), sedative dependence. Background characteristics of the study sample have been described in depth previously (
49 ).
Out of the total sample, 361 (90 percent) were located for follow-up; 351 (88 percent) completed the follow-up interview; five (2 percent) did not complete the follow-up because they refused, three were deceased, and two could not be scheduled; and the remainder (39 patients, or 10 percent) were not located for follow-up. Comparisons between those who did and did not complete the six-month follow-up interview revealed no significant differences in background characteristics or in follow-up rates by program where they were treated.
Measures
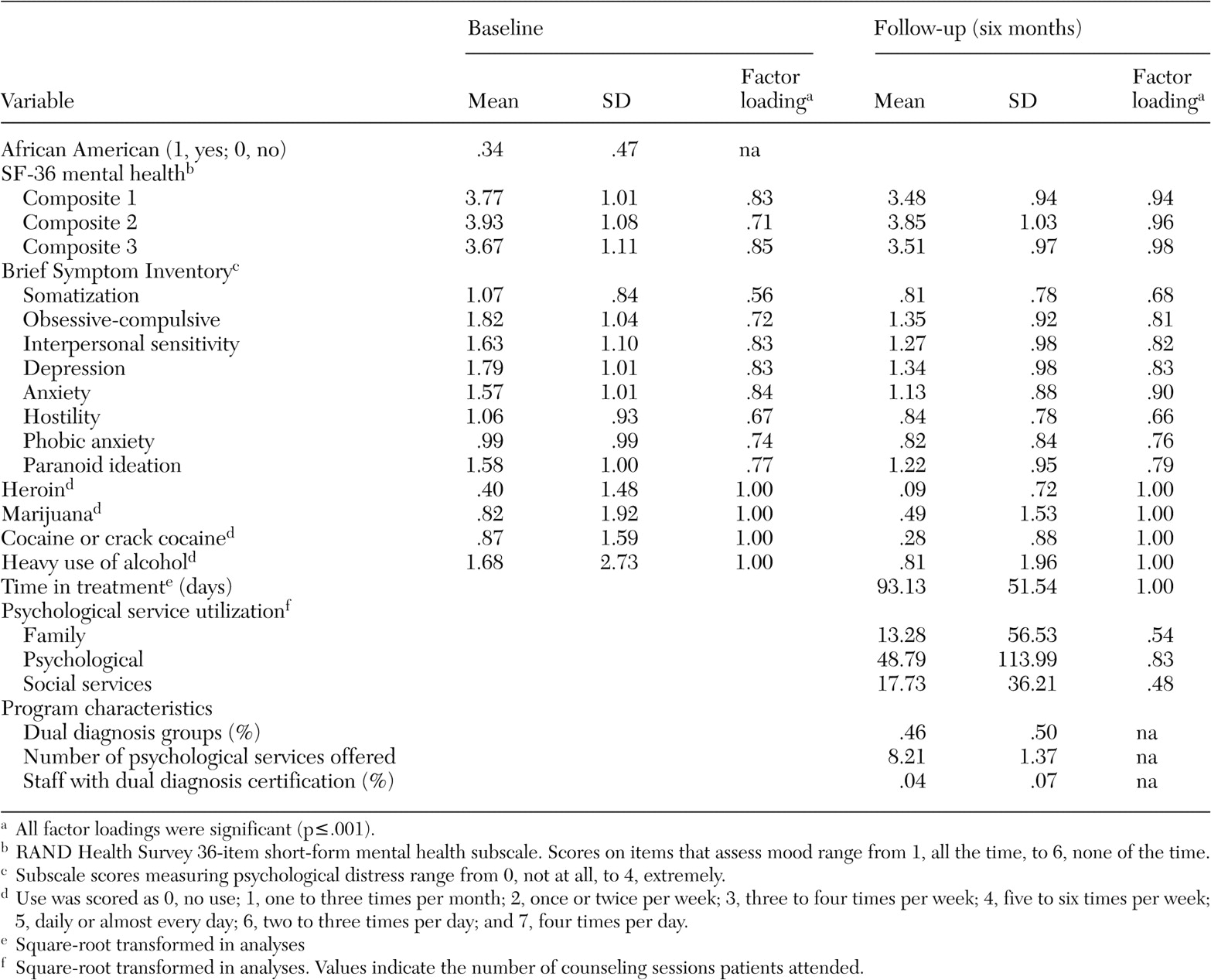
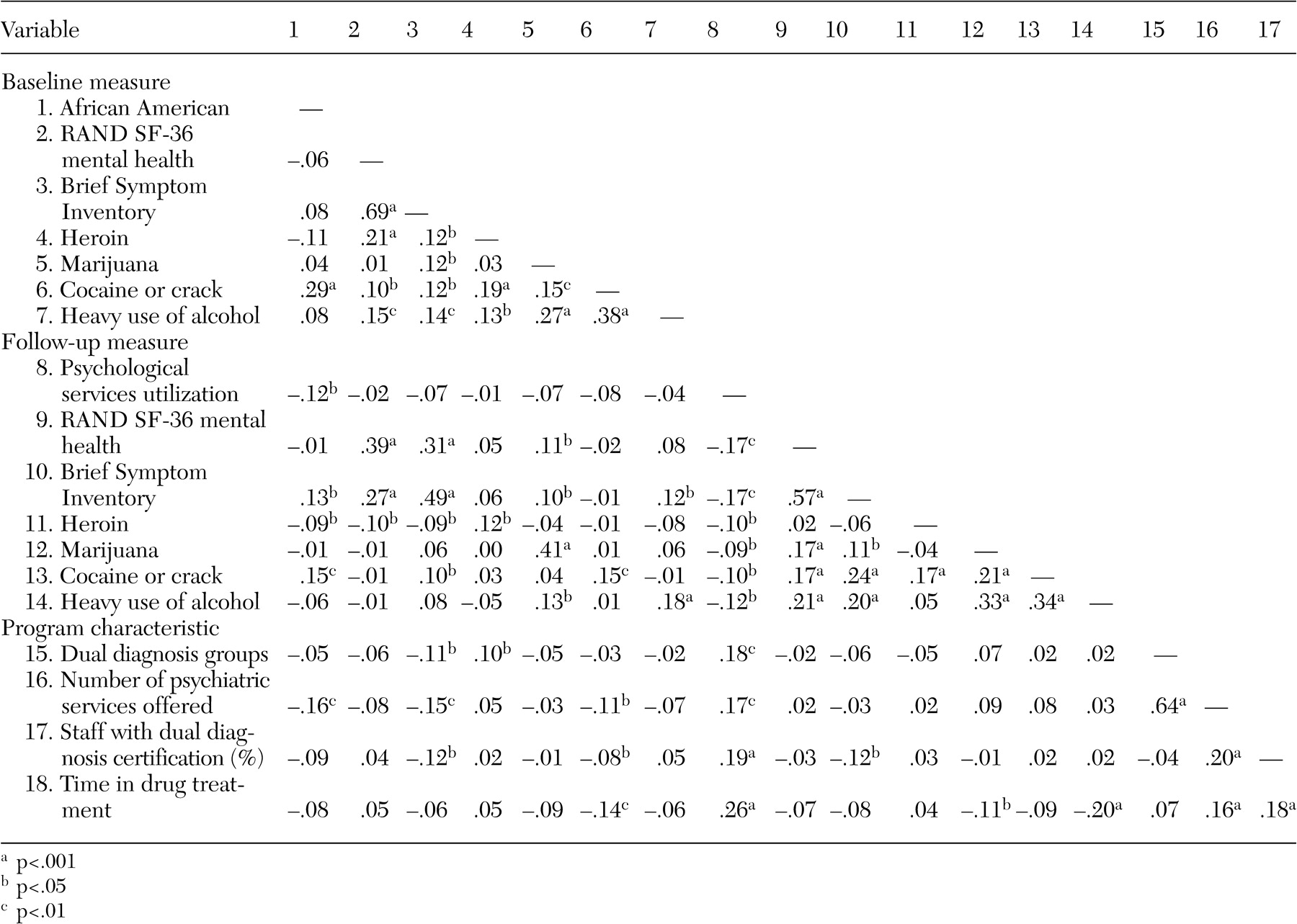
Baseline patient-level measures. Background patient characteristics included in the analyses consisted of ethnicity (African American: 1, yes, 0, no), two measures of psychological functioning, and substance use frequency. Other demographic characteristics, including Hispanic or white ethnicity, gender, age, marital status, and education, were examined as possible predictors but were not significantly associated with the outcome measures and thus were dropped from the analyses.
The Brief Symptom Inventory (BSI) (
50 ) was used to assess psychological distress at the time of treatment admission. The BSI is a 53-item questionnaire derived from the Symptom Checklist-90; respondents rate on a 5-point scale how much a symptom distressed them during the previous week (0, not at all; 4, extremely). Eight subscales from the BSI were used as indicators of an overarching latent variable representing psychological distress. The subscales included somatization, obsessive-compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, and paranoid ideation.
The second measure of psychological distress was a latent variable indicated by three composite parcels formed from the means of nine items from the RAND Health Survey 36-item short form (SF-36) (
51 ) that constitute the mental health subscale of energy and emotions. Items were combined randomly to form three separate indicators because of the high coefficient alphas among the items at baseline (.83) and follow-up (.94) (
52 ). The items assess depressed mood in the previous four weeks. Scores range from 1, all of the time, to 6, none of the time, and were reverse-scored where appropriate so that higher scores indicated more distress.
Four items assessed frequency of use of specific substances in the 30 days before treatment admission. Heroin, marijuana, cocaine or crack, and heavy use of alcohol (alcohol use to intoxication) were included. Each variable was assessed on an 8-point scale: 0, no use; 1, one to three times per month; 2, once or twice per week; 3, three to four times per week; 4, five to six times per week; 5, daily or almost every day; 6, two to three times per day; and 7, four times per day.
Baseline program-level measures. Three program-related variables from the administrator survey were included in the current analysis: first, whether the programs provided "dual diagnosis groups" (meaning self-help or group counseling specifically for this population); second, the total number of psychological services provided on site, summed from a list of 15 specific services; and third, the percentage of counselors and case managers who had obtained certificates or specialized training in dual diagnosis treatment.
Follow-up measures. Psychological service use consisted of the number of family, psychological, and social service counseling sessions the patient attended during the six-month follow-up period and was assessed with the Treatment Services Review (
53 ). Services included those received in the initial drug treatment episode as well as services received in aftercare or other treatment settings. Each sum was a separate indicator of a latent variable representing service use. This variable was positioned as a mediator of the outcomes. Time in drug treatment (measured in days) was included as a control variable predicting service use and the outcomes, because time in treatment alone could have affected the observed outcomes rather than use of specific services.
Psychological distress and substance use were assessed in exactly the same fashion at the six-month follow-up as they had been at baseline (BSI, RAND SF-36 Mental Health subscale, and frequencies of substance use).
Analytic method
The EQS structural equations program was used to perform the latent variable analyses (
54 ). Goodness of fit of the models was assessed with the maximum likelihood chi square statistic, the comparative fit index (CFI), the Satorra-Bentler chi square test (S-B chi square test), the robust comparative fit index (RCFI), and the root-mean-squared error of approximation (RMSEA) (
54,
55 ). The robust S-B chi square test was used in addition to the maximum likelihood chi square test because it is more appropriate when the data depart from multivariate normality. The CFI and RCFI range from 0 to 1 and reflect the improvement in fit of a hypothesized model over a model of complete independence among the measured variables. The RCFI adjusts for sample size; values at .95 or greater are desirable, indicating that the hypothesized model reproduces 95 percent or more of the covariation in the data (
55 ). The RMSEA is a measure of fit per degrees of freedom, controlling for sample size, and values less than .06 indicate a relatively good fit between the hypothesized model and the observed data (
55 ). The 90 percent confidence intervals (CIs) are also provided for the RMSEA.
An initial confirmatory factor analysis assessed the adequacy of the measurement model and the associations among the latent variables. Correlated error residuals were allowed between the same measured variables at baseline and at six months. Suggestions from the Lagrange Multiplier Test, which reports modifications to the original model that will improve the fit, were evaluated (
56 ). Modifications were allowed only if they made sense theoretically and logically.
We also assessed intraclass correlation coefficients (ICCs) among the patient characteristics and outcome variables in the model to ascertain whether a multilevel model would be appropriate given that the patients were nested within different programs. When ICCs for a dependent variable are negligible across organizational units and cluster size is small, multilevel models are not appropriate or necessary (
57,
58 ). The ICCs were small for all dependent variables, with a mean of .03. The only large ICC was .19 for African Americans, indicating that individuals of similar ethnicity tended to cluster within programs.
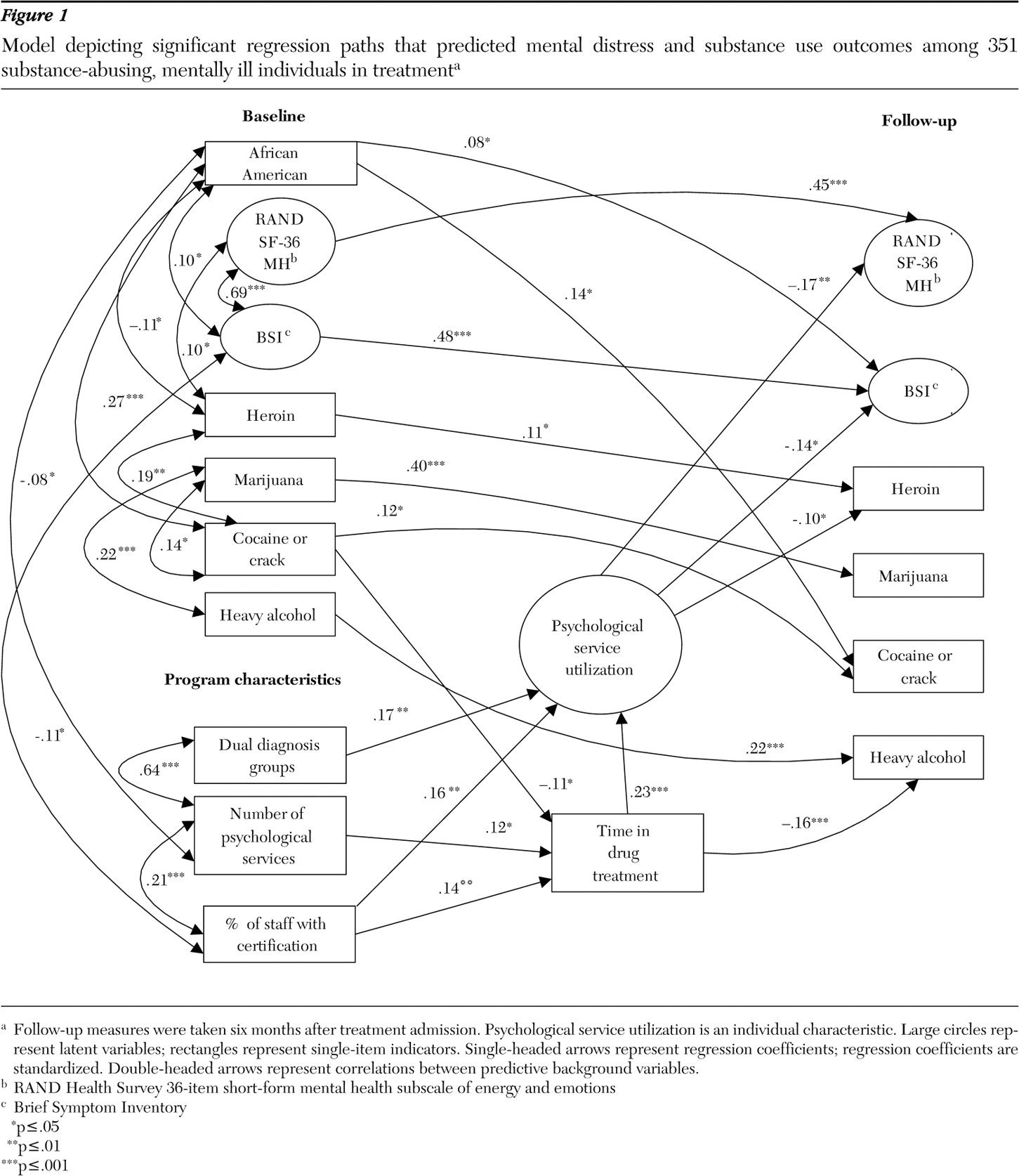
We then tested a predictive path model that positioned baseline patient and program characteristics as predictors of psychological service use as well as the outcome variables reflecting psychological distress and substance use. Program characteristics also predicted time in drug treatment, which was used as a further predictor of psychological service use. Time in drug treatment was also tested as a direct predictor of the outcomes to avoid a possibly spurious relationship between psychological service use and improvement in the outcome variables as a result of a longer drug treatment episode. Relationships that were significant among the predictive background variables were also included in this model as covariates. Nonsignificant paths and correlations in this model were trimmed gradually by following the recommended model-evaluation procedure of MacCallum (
59 ).