The September 11, 2001, terrorist attacks on the World Trade Center resulted in widespread traumatic stress and psychiatric symptoms (
1 ). In response to these attacks, the New York State Office of Mental Health rapidly created a large-scale public health intervention, Project Liberty, that offered short-term crisis counseling, psychoeducational interventions, and triage referral to residents of the greater New York City metropolitan area (
2 ). Free, anonymous brief counseling was available for more than two years after the attacks. The project provided face-to-face disaster-related services through outreach in community settings, such as homes, businesses, and schools. Providers were required to complete logs of service encounters indicating demographic information about recipients, date and location of service, and up to 16 risk categories that identified certain groups (for example, family of missing or deceased, persons who had been physically injured, and uniformed and rescue personnel) who were likely to be at especially high risk of experiencing impairment, most notably posttraumatic stress disorder (PTSD) (
3,
4 ) and depression (
5 ).
Little is known about the timing of entry into counseling by members of such high-risk groups (
6 ). This study examined the timing of entry into service for different risk groups by determining the dates on which individuals in various risk groups first accessed Project Liberty's individual counseling services for 27 months after the attacks.
Methods
Logs of service encounters from the 177 community-based Project Liberty programs that operated through December 31, 2003, recorded a total of 753,015 service encounters (687,848 individual, 37,232 group, and 27,935 public education) that were processed as a data extract dated May 7, 2004. During these visits, counselors coded service recipients into one or more of 16 risk categories, combined into eight clusters: family of missing or deceased; persons directly affected (that is, injured in the attacks, had a home with major damage, evacuated the World Trade Center, evacuated school, or worked at the World Trade Center but was absent on September 11, 2001); uniformed personnel (that is, firefighters, police, and Port Authority police); other rescue or recovery workers; schoolchildren; displaced employed and unemployed workers; persons with disabilities (that is, past or pre-existing trauma, psychological or substance abuse problems, or physical disability that limits mobility); and the general population.
To avoid having individual entries duplicated, categories were arranged hierarchically, as described above. Each service recipient was categorized as belonging to the first applicable category—for example, if an individual had both lost a friend or family member and was a rescue worker, he or she would be placed in the "family of missing or deceased" category and not the "other rescue or recovery workers" category. The Mount Sinai School of Medicine Institutional Review Board found this secondary analysis of anonymous data to be exempt.
Results
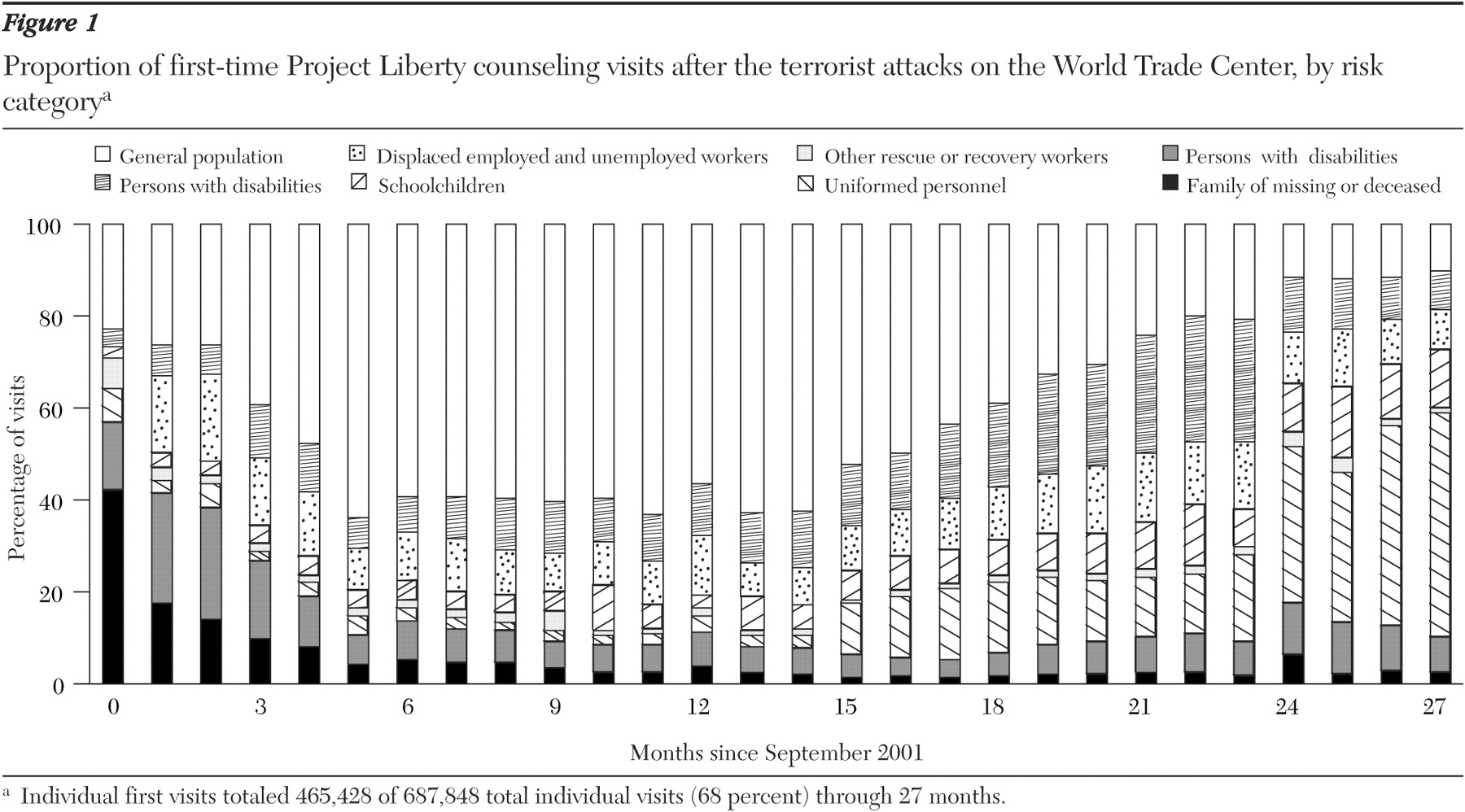
Figure 1 shows data from all 465,428 service logs for individual counseling coded as first visits and plots the proportional use of first-time Project Liberty counseling visits by members of each risk category relative to other categories for 27 months after the World Trade Center attacks. Overlap between uniformed personnel and other rescue or recovery workers was also examined.
Across 27 months, just a little over half (244,515 of 465,428 persons, or 53 percent) of service logs for first visits were for individuals in one of the first seven risk groups. The proportion of individuals in one of the first seven risk groups as compared to the general population was curvilinear, such that members of one of the first seven risk groups accounted for between 60 and 76 percent of all first visits during the first four months, then dropped to about 40 percent until 15 months, when the proportion climbed to nearly 90 percent in the 24th to 27th month.
Within this overall pattern, three outcomes are noteworthy. First, brief counseling for persons who lost family members or friends was proportionally large initially, accounting for more than 40 percent of the first visits in the month immediately after the World Trade Center attacks, but the rate declined dramatically after that point (5 percent or less after month 5). Second, a major proportional increase in counseling occurred for uniformed personnel, from about 3 percent of first visits in the first 12-month period to about 14 percent in the second 12-month period, with an even more dramatic increase to about 42 percent occurring during months 25 to 27. Only a small percentage of uniformed personnel were also coded as "other rescue or recovery workers": 4 percent (346 of 8,979 persons) of fire personnel, 2 percent (721 of 32,209 persons) of police officers, and 12 percent (87 of 702 persons) of Port Authority police. Third, the proportion of displaced employed and unemployed workers with first visits was both substantial (about 11 percent across 27 months) and quite consistent (ranging from 8 to 19 percent) throughout the 27-month period.
Discussion
The anonymity of respondents made it impossible to link first and subsequent counseling visits, which represents a limitation of this investigation. Analysis of first-time counseling is nonetheless instructive in that it was used proportionally more by high-risk individuals than the general population, both immediately after and during the second year after the World Trade Center attacks. The large proportion of fire and police personnel who sought counseling, especially after the first anniversary of the World Trade Center attacks, was especially noteworthy. In the context of disaster work (
6,
7 ), such individuals are at increased risk of developing PTSD and depression months and even years after major disasters. Increased use of counseling by uniformed personnel may also have been in response to specialized advertising campaigns in partnership with professional baseball teams that targeted male rescue workers and uniformed personnel. In the fall of 2002 the Police Organization Providing Peer Assistance was added to the list of Project Liberty providers to conduct outreach and provide service to police. It is clear that individuals in need of treatment accessed these services more than two years after the event, underscoring the need for promoting their continued availability for several years after a disaster.
In addition, these data show how specific treatment emphases could be shifted usefully to target needs of individuals at higher risk who emerge at different times after disasters. For example, grief work (
8 ) could be initiated immediately after disasters. The healing power of mourning rituals (for example, funerals) may well augment the effectiveness of such grief interventions to expedite more rapid return to normal functioning (
9 ). Subsequent cognitive-behavioral interventions could be targeted to help rescue workers and uniformed personnel improve their networks of social and occupational support (
10 ). As unemployment and occupational dislocation are constant financial stressors that are associated with psychiatric impairment, counseling also could profitably be combined with provision of meaningful work experiences for unemployed and displaced workers.
Conclusions
After the first anniversary of the World Trade Center attacks, individuals at higher risk than the general population used proportionally more first-time counseling services. Family members who had lost loved ones accounted for the largest percentage of visits in the first month, whereas uniformed personnel used disproportionately larger percentages of services near the end of the second year. Occupationally displaced and unemployed workers sought counseling at a relatively steady rate. These patterns suggest that large-scale counseling services be made available initially, with more attenuated services available for extended time periods after disasters and amplification of services around event anniversaries. The focus of counseling might be shifted to meet emerging needs of different high-risk groups.
Acknowledgments
This evaluation was funded by grant FEMA-1391-DR-NY (titled "Project Liberty: Crisis Counseling Assistance and Training Program") to New York State from the Federal Emergency Management Agency. The Center for Mental Health Services of the Substance Abuse and Mental Health Services Administration administered the grant.