Stigmatization involves a separation of individuals labeled as different from "us" who are believed to possess negative traits, resulting in negative emotional reactions, discrimination, and status loss for the stigmatized persons (
1 ). Stigmatization of individuals diagnosed as having serious mental illnesses has been observed across the world, and the family members who help care for them report feeling stigmatized as a result of their association with the loved one with mental illness (
2,
3,
4,
5 ).
This study investigated the correlates of perceived stigma among the family caregivers of persons with diagnoses of bipolar disorder, a topic that has received little prior attention. We hypothesized that increased caregiver stigma is likely to be associated with patient characteristics that facilitate an "us-them" response by exposing the differences between persons with mental illness and those in the general population and with caregiver characteristics that increase the caregiver's vulnerability to negative emotional reactions.
Caregiver characteristics that have been found to be associated with caregivers' increased perceptions of mental illness stigma include higher education of the caregiver (
2,
3 ), younger or older age groups (
5,
6 ), race or ethnicity of the caregiver (
7 ), being a caregiver who is the spouse of the person with mental illness or who is female (
3 ), and mental health problems of the caregiver (
8 ). More educated caregivers may be more sensitive to rejection or status loss or may actually experience more rejection (
2,
9 ). Female caregivers may perceive greater stigma (
3 ), perhaps resulting from increased attunement to the nuances of interpersonal interactions, such as devaluation. Caregivers who are highly burdened, have limited support networks, or have depressive symptoms may also be more sensitive to, or may experience, greater stigmatization (
10 ). Caregivers who live with the patient may experience more direct discrimination compared with those who do not. Because individuals with mental illness from racial or ethnic minority groups live with their family more often than those who are white (
11,
12 ), their caregivers may experience more stigma.
Patient characteristics associated with caregivers' greater perceptions of mental illness stigma include younger age of illness onset, longer illness duration (
3,
5 ), and both male and female gender (
2,
3,
5 ). In the early phases of the illness, usually during late adolescence or early adulthood, caregivers' perceptions of stigma may be greater because the illness interferes with the affected individual's developmental tasks or meeting social role expectations. Certain illness characteristics or comorbid features of bipolar disorder may also increase the likelihood of being labeled as different from peers. Bipolar I disorder may result in greater perceptions of stigma than bipolar II disorder, because bipolar II disorder does not involve impairing behaviors or hospitalization, both of which may identify the patient as different. Possessing more than one stigmatizing attribute (
13 )—such as having bipolar disorder and being an "addict," having a history of arrests, or having prior psychiatric hospitalizations—may exacerbate caregivers' perceived or experienced stigma.
In contrast to the studies cited above, the study presented here examined a broad sample of individuals with bipolar disorder, some of whom had been stable over the previous year and some of whom had been ill throughout most of the prior year. Although labeling theory posits that mental illness stigma persists once labeling has occurred, irrespective of symptomatic improvement (
14,
15 ), empirical research has demonstrated that caregivers' perceptions of stigma may decrease as the patient recovers (
2 ), even when the patient has had a psychiatric hospitalization in the remote past (
3 ). Link and colleagues (
16 ) have also suggested that the strength of the association between stigma and a particular variable may decrease as the illness improves and active symptoms no longer identify the individual as different. Because hypothesized associations between patient and caregiver characteristics and stigma perceptions could be weakened by inclusion of stably asymptomatic individuals, we focused hypothesis testing on caregivers of patients in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) who were recently symptomatic (defined below).
We hypothesized that caregivers of female patients, who had earlier age of illness onset, a greater number of psychiatric hospitalizations, bipolar I disorder, substance use comorbidity, and a prior arrest history would report higher levels of stigma than caregivers of patients without these attributes. We predicted that female caregivers who were spouses, were more educated, were younger, lived with the patient, had fewer social supports, had greater burden, and had more depressive symptoms would report greater mental illness stigma. Ethnicity or race associations with stigma were examined on an exploratory basis. A group of caregivers of stable STEP-BD patients served as a comparison group.
Methods
Study design
This study employed baseline data from the Family Experience Study (FES) to test the above hypotheses. FES is a national, multisite study of 500 caregivers' experiences with individuals with bipolar disorder (
17 ). FES caregiver interview data were collected in conjunction with the STEP-BD, a longitudinal treatment effectiveness study for individuals with bipolar disorder that enrolled patients between November 1999 and January 2004. Details of the STEP-BD design are further detailed by Sachs and colleagues (
18 ).
Patients and caregivers for the study presented here were recruited in outpatient clinics from eight STEP-BD sites participating in FES. Enrollment for FES began in July of 2002, and follow-up caregiver interviews were conducted at six and 12 months after a baseline interview. Consenting patients identified the friend or family member most involved in their care—that is, the person who responds in an emergency, attends appointments, provides financial assistance, or interacts on a daily basis. All patients provided informed written consent, and the study was reviewed and approved by their respective university human research committees. Caregivers were then invited to participate during patient visits or by phone. Those providing written informed consent were assessed on baseline measures of stress, coping, health, and service use by phone or in person for about 90 minutes. Caregiver interviews were coordinated with the patient visit schedule so as to be administered within 30 days of the psychiatric clinical or data collection visit. The study presented here reports cross-sectional data from the caregiver baseline assessments only, collected from July 2002 to January 2004. Additional details of the study are available in a report by Perlick and colleagues (
17 ).
Patient assessments
Diagnoses. The bipolar disorder diagnosis (I, II, and not otherwise specified and schizoaffective, bipolar type) was made through a standardized affective disorder evaluation (ADE) (
19 ). The ADE includes a modified version of the mood and psychosis modules from the Structured Clinical Interview for DSM-IV (
20 ). The ADE assesses for prior arrests (coded as yes or no). Alcohol and substance use disorders were determined by using the Mini-International Neuropsychiatric Interview Plus, version 5.0 (MINI), a semistructured interview designed to identify current major axis I disorders (within the past 12 months) (
21 ). Alcohol use comorbidity included abuse or dependence or both, and substance use comorbidity included abuse or dependence or both of any nonalcohol substance. The ADE and MINI were completed at STEP-BD entry by STEP-BD trained clinicians.
Days well. Patient clinical status was assessed by calculating the number of days in which the patient was "well" (that is, nonepisodic) in the first year of his or her participation in STEP-BD. This measure, calculated by the STEP-BD data center, was based primarily on
DSM-IV criteria for mood episodes assessed at each psychiatric visit by using the clinical monitoring form (
18 ). The mean number of psychiatric visits during this first year was 9.34±7.31. Research assessments with the Montgomery Asberg Depression Rating Scale (
22 ) and the Young Mania Rating Scale (
23 ) as well as recent psychiatric hospitalizations were also considered in the determination of days well. The number of days between clinical visits was used in estimating the number of days that the patient was considered to be well or unwell. For example, when the patient was nonepisodic at two consecutive visits, he or she was considered well during that interval. If the patient was episodic at both clinical visits, he or she was considered unwell for the days during that interval. If the patient was nonepisodic one visit and episodic the next, he or she was considered well half of the days during that interval.
A majority of caregivers (275 of 500 caregivers, or 55%) completed the baseline interview during the patient's first year in STEP-BD, when days-well data were being collected. This was true for patients enrolled in STEP-BD during or after July 2002 when the FES began. For the remaining 45% of caregivers whose patient-relative entered STEP-BD before July 2002, days-well ratings were retrospective.
We hypothesized that associations between patient and caregiver characteristics and caregiver stigma perceptions would be evident only for patients who were currently or had recently been symptomatic. Naturalistic studies of bipolar disorder report that a majority of patients remain symptomatic after an acute episode and are not able to maintain role performance for at least half of the following year (
24,
25 ). On the basis of these findings, patients who were nonepisodic for more than three-fourths of the year were defined as being in the "well group." The remainder were classified as being in the "unwell group."
Caregiver assessments
CES-D. The Center for Epidemiologic Studies Depression Scale (CES-D) (
26 ) was used to assess depressive symptomatology. The CES-D is a 20-item scale with construct validity (Pearson's r=.7-.8) and cross-cultural validity (
27,
28 ).
Caregiver burden. The Social Behavior Assessment Schedule (
29 ) assesses patient problematic behavior and social role performance (defined as objective burden) and adverse effects on others (impact of patient's illness on the caregiver's work, social life, and emotional and physical well-being; defined as subjective burden). Interrater reliability has been reported for subjective burden subscales: .88 for problem behavior, .76 for role dysfunction, and .81 for adverse effects (
30 ); four items were added to typify manic-phase behaviors and symptoms, for a total of 39 items. Each item has an objective and subjective rating, both scored on a 3-point ranked scale. For example, the caregiver is asked to what degree the patient was withdrawn in the past six months (objective burden) and then to what degree the caregiver was distressed by the withdrawal (subjective burden). Scales were summed for a total scale score.
Social interactions. Social interactions were assessed with an 11-item brief form (
31 ) of the Duke Social Support Index (DSSI) (
32 ). The DSSI asks about frequency of social interactions in the previous week and then subjective experience of social support, ranked on a 3-point scale ranging from 1, hardly ever feeling supported, to 3, feeling supported most of the time.
Mental illness stigma. Mental illness stigma was measured by the Discrimination-Devaluation Scale (DDS), a combination of the Patient Devaluation and Stigma Scale (
15 ) and the Family Devaluation and Stigma Scale (
33 ). The DDS is a 15-item measure rating caregivers' views about most people's acceptance of mental illness. Scores are ranked on a 4-point scale ranging from 1, strongly agree, to 4, strongly disagree. Eight questions assess patient-focused stigma, such as "Most people look down on someone who once was a patient in a mental hospital." Seven questions assess caregiver-focused stigma, such as "Most people do not blame parents for the mental illness of their children." Items were summed for an overall stigma score, with higher scores indicating greater perceptions of mental illness stigma. A prior study reported moderately high correlations of these combined scales with two caregiver samples (.58 and .62) (
4 ).
Statistical analysis
Means and standard deviations were calculated for continuous variables, and proportions were calculated for categorical variables. We stratified patients by clinical status, using the days-well variable, and tested hypotheses separately for the resulting well and unwell groups. We first examined whether stigma scores (subscales and then overall score) were higher for the unwell group. Bivariate analyses were conducted to examine associations with perceived stigma. Pearson product-moment correlations were used for continuous variables, and analysis of variance was used for categorical variables, with Bonferroni corrections to adjust for the number of post hoc comparisons. The overall stigma score was used to represent perceived stigma in these analyses, because the overall scale had the highest internal consistency reliability (.86 versus .75 for the patient scale and .80 for the caregiver scale).
Exploratory multivariate linear regression with a backward stepwise procedure was employed to evaluate the associations between stigma and variables that had shown significant relationships (p<.05) with stigma in the bivariate analyses. Analyses were run separately for the well and unwell groups.
In view of variations in the timing of the caregiver baseline interview in relation to the period during which days-well data were collected, the above bivariate analyses were repeated as a reliability check. We used the cross-sections clinical status rating linked to the caregiver interview (that is, within 30 days), which also characterized the patient as unwell (that is, met criteria for a subsyndromal or major mood episode) or well (that is, recovered).
Results
Degree of stigma and correlates
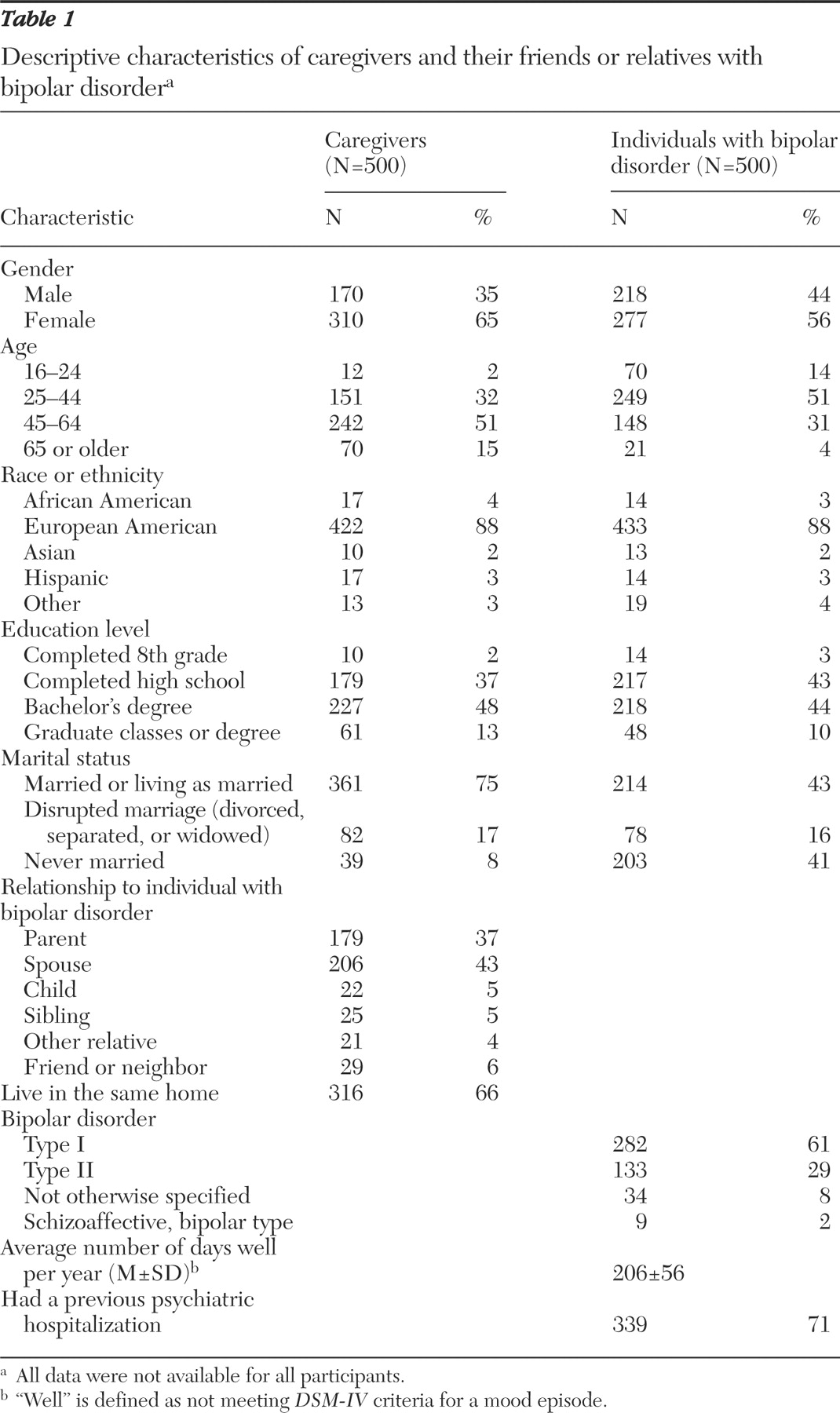
Table 1 provides descriptive statistics for caregivers and patients. For the patient-focused subscale of mental illness stigma, averaged across items, a majority of caregivers agreed or strongly agreed with 66% of stigma endorsing statements (data not shown). For the caregiver-focused subscale of mental illness stigma, a majority of caregivers agreed or strongly agreed with 38% of stigma-endorsing statements. There were no significant differences between well and unwell groups on scores of patient stigma, caregiver stigma, or overall stigma.
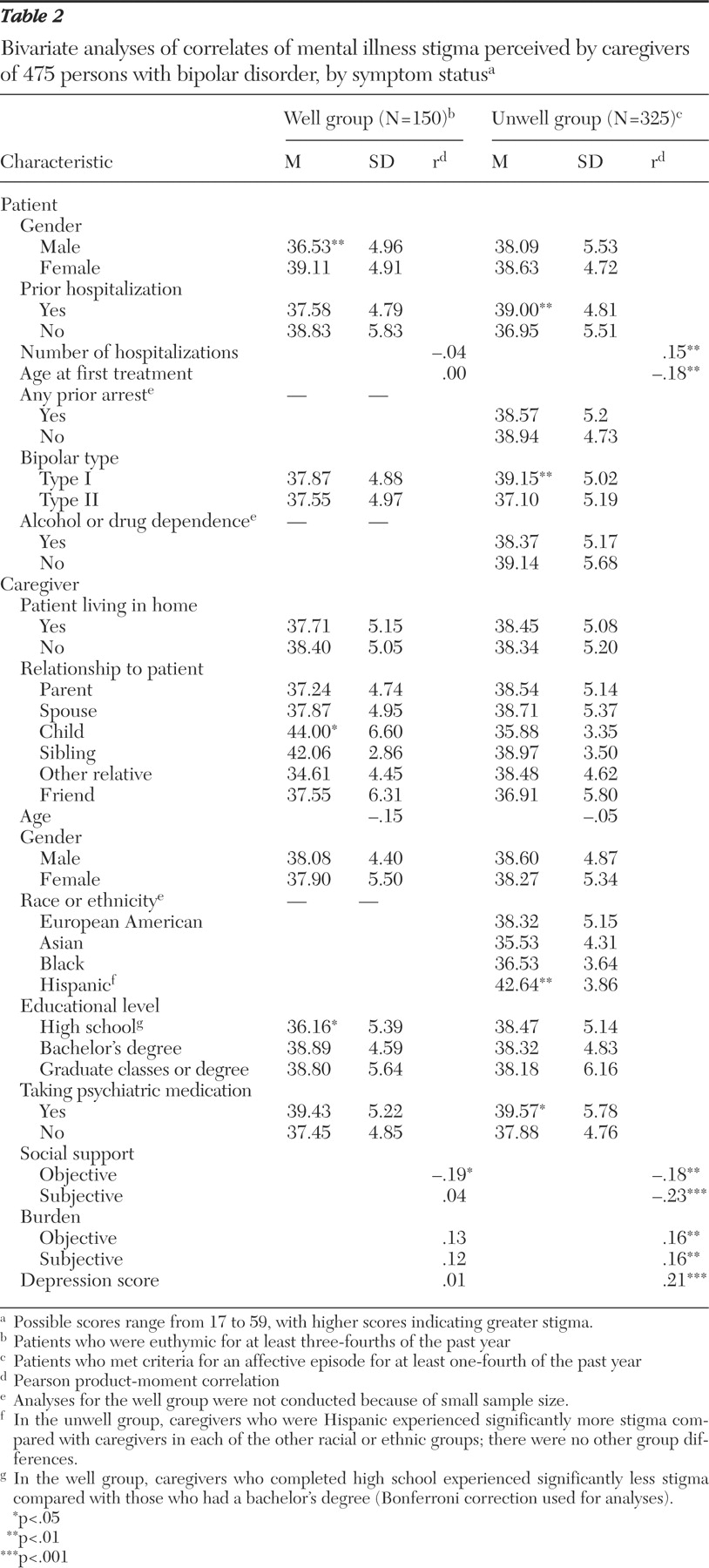
Correlates of stigma over a year for well and unwell groups in bivariate analyses are reported in
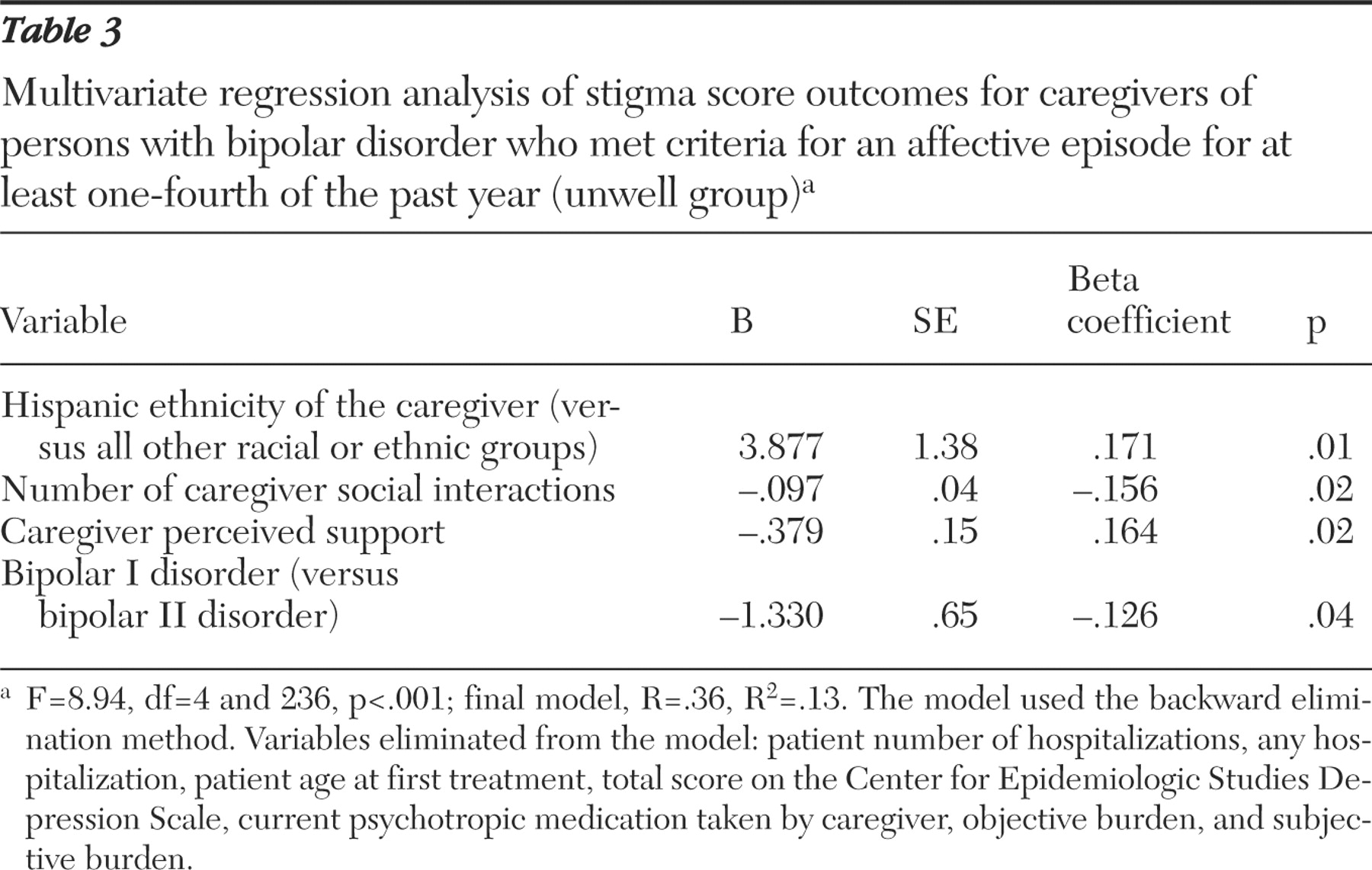
Table 2 . For the unwell group, significant correlates of stigma were entered into a regression equation as independent variables: patient age at first treatment, patient hospitalizations (yes or no), number of patient hospitalizations, bipolar I disorder versus bipolar II disorder, objective and subjective caregiver burden, caregiver ethnicity (Hispanic versus all others), caregiver CES-D score, current psychotropic medication taken by caregiver (yes or no), number of caregiver weekly social interactions, and perceived caregiver social support. As shown in
Table 3, bipolar I disorder, as opposed to bipolar II disorder, remained associated with greater stigma (t=-1.33, df=5,251, p=.04). Hispanic ethnicity (t=2.81, df=5,251, p=.005), fewer weekly social interactions (t=-2.401, df =5,251, p=.02), and less perceived social support (t=-2.53, df=5,251, p=.02) also remained associated with greater stigma. Given the smaller number of Hispanic caregivers, outlier diagnostics were used to evaluate the presence of stigma scores beyond two standard deviations from the mean that might have influenced the findings; no outlier scores were found for this group.
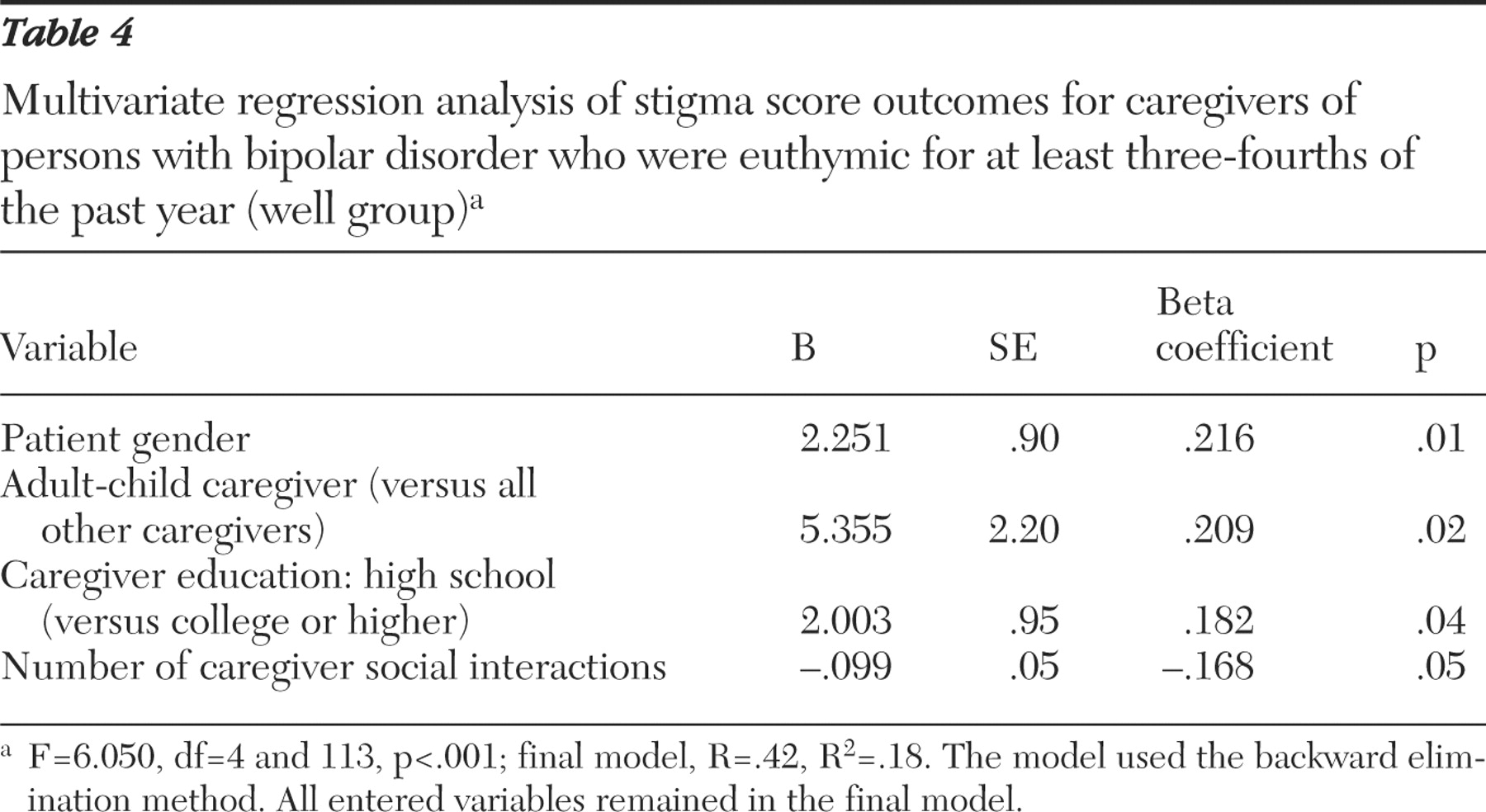
For the well group, predictor variables were entered in the multivariate regression: patient gender, caregiver education level, relationship of caregiver to patient (adult child versus all others), and number of weekly caregiver social interactions. As shown in
Table 4, variables that remained associated with greater stigma perceptions were female gender of the patient (t=2.50, df=4,113, p=.01), caregivers who were children of the individual with bipolar disorder (t=2.43, df=4,113, p=.02), caregivers with at least a college education (t=2.12, df=4,113, p=.04), and caregivers with fewer weekly social interactions (t=-1.96, df=4,113, p=.05).
The bivariate analyses that substituted clinical status from within 30 days of the more recent clinical status linked to the caregiver baseline interview demonstrated an almost identical pattern of results from days well in a year, with the Pearson r and F values highly similar. When using the cross-sectional clinical status measure, some significant associations were reduced to trends, compared with the measure of days well over a year, a more reliable measure of what relatives face day to day.
Discussion
This study examined associations of patient, illness, and caregiver characteristics with caregivers' perceived stigma in bipolar disorder. We hypothesized that for caregivers of patients who had recently exhibited active symptoms, the caregiver, patient, and illness attributes that clearly identified the patient as different from others or that increased caregiver susceptibility to social rejection would be associated with higher levels of perceived stigma. Our hypotheses were borne out in part. Among the patient characteristics, early age of onset, a greater number of hospitalizations, and being diagnosed as having a more severe type of illness were associated with higher levels of caregivers' perceived stigma at the bivariate level. However, only illness type remained significant at the multivariate level, perhaps because of shared variance between these measures. Among the caregiver characteristics, higher levels of burden, depressed mood, and lower levels of social support were associated with higher levels of perceived stigma, although only social support remained significant at the multivariate level.
Caregivers whose relatives display a more severe type of bipolar disorder perceive higher levels of stigma; however, stigma experiences are less distressing for caregivers who are surrounded by supportive persons who are less likely to stigmatize. Or, caregivers who perceive less stigma may be more likely to seek social support. The finding that Hispanic caregivers had higher levels of perceived stigma than other caregivers should be regarded as preliminary and interpreted with caution given the small sample. Although more of the patients who had Hispanic caregivers resided with them (82% of patients with Hispanic caregivers compared with 59 % to 65% of patients with caregivers from other racial or ethnic groups), co-residence was not a significant correlate of stigma, and thus more direct exposure of these caregivers to mental illness discrimination did not appear to explain this finding.
Correlates of stigma within the well group
Because patients in the well group had not been identified as different by their illness symptoms for the greater part of one year or longer, we did not hypothesize that there would be associations between patient illness features, caregiver stress, or other measures to perceived stigma. Contrary to expectations, we found that both patient and caregiver attributes (female gender of the patient, more caregiver education, fewer social interactions, and being an adult child of the patient) were significantly associated with perceived stigma at the multivariate level. Interestingly, however, the variables associated with stigma in the well group differed from those associated with stigma in the unwell group.
Our results suggest that stigma does not simply subside when symptoms remit but rather is related to different factors. The finding that caregivers in the well group perceive as much stigma overall as caregivers in the unwell group further supports this view. One potential explanation for this pattern of findings is that social role expectations and system interactions differ based on the "wellness" of a person. For example, college-educated caregivers may have higher aspirations for their relative with bipolar disorder, which are only operational when the relative is well and able to return to work or school. Engaging in more demanding social role activities might also expose deficiencies or residual symptoms leading to devaluation or rejection, or it might create stress, which exacerbates stigmatizing illness symptoms.
Increased social role expectations may also explain the association between female gender of the patient and stigma in the well group. Females are more often expected to socialize with others outside the family, and family members may feel more stigmatized if their female spouse or child with bipolar disorder does not live up to this social role expectation. Alternatively, female patients who assume or resume their social and occupational activities may be more discriminated against than their male counterparts for manic or hypomanic behaviors, such as interpersonal aggression, hypersexuality, and risk taking, because these traits are more socially acceptable in males. The role of caregiver for adult children may be especially stigmatizing, because caring for a parent early in life is atypical; such perceptions of stigma may be heightened during periods of symptom remission when the parent resumes going to work or social functions and is thus more likely to expose his or her child to experiences or reports of rejection. In contrast to the above findings limited to the well group, the finding that increased stigma was associated with decreased social interactions was significant for both groups, suggesting that social support is an important correlate of stigma for caregivers during all phases of the relative's illness.
Comparison with other studies and limitations
Our findings differed from those of other studies that found that caregiver gender and age were associated with perceived stigma. Patient gender, caregiver education level, and caregiver relationship to the patient were related to stigma, but only in the well group, and it was adult children in this group who reported the most stigma, rather than spouses as in prior studies. Differences between our findings and prior studies may be attributed to differences in caregiver samples, patient samples, or measures of stigma. For example, education level was relatively high in this group of patients and caregivers, and a skewed distribution or restricted range might lead to negative findings in the unwell group. Our sample was also larger and more heterogeneous than those employed in other studies, potentially obscuring relationships observable in a sample with fewer extraneous sources of variance. Most studies have not evaluated the strength of associations with stigma in relation to patient clinical status, and our findings suggest that results may differ depending on patient symptom level. Finally, the measure of stigma we employed assesses the stigmatizing beliefs attributed to "most people," whereas measures from prior studies have inquired about the caregiver's direct experience of discrimination and might have yielded more positive findings.
This study has several limitations. Because caregivers declining participation or whose family members were not in active treatment were not investigated, we may have excluded the most stigmatized caregivers. This was a cross-sectional study that precludes drawing causal inferences. Use of qualitative methods might have enhanced interpretation of findings. Replication of our findings regarding race or ethnicity and stigma in larger samples is needed. In addition, further investigation of particular stigma experiences is needed to examine the relationship between social role expectations and caregiver stigma for patients whose symptoms have stabilized.
Conclusions
At the community level, interventions that decrease mental illness stigma might increase the likelihood that when needed, family members will seek social support, which is evidently quite important for caregivers. At the individual level, a significant number of caregivers were receiving medication for emotional problems. Level of functioning, sociocultural context, and particular factors viewed as stigmatizing (for example, labeling and symptoms) should be considered when determining the social and developmental issues of greatest concern to the family. In treatment for caregivers, improving the quality and quantity of social support should be a primary recommendation (for example, the Depression and Bipolar Support Alliance). When caregivers have no psychiatric diagnosis, family therapy without the patient present is available; however, the lack of medical insurance coverage of this treatment remains a problem.
Acknowledgments and disclosures
This study was conducted with the support of grants N01-MH-80001 and R01-MH-65015 from the National Institute of Mental Health. The authors thank Gary S. Sachs, M.D., and Michael E. Thase, M.D., principal investigators for the STEP-BD. The STEP-BD Family Experience Collaborative Study Group consisted of Joseph R. Calabrese, M.D., Terence A. Ketter, M.D., Mark Fossey, M.D., Lauren B. Marangell, M.D., Andrew A. Nierenberg, M.D., and Jayendra Patel, M.D.
Dr. Bowden reports receiving research grants from Abbott Laboratories, Bristol-Myers Squibb, Elan Pharmaceuticals, GlaxoSmith-Kline, Janssen, Lilly Research, the National Institute of Mental Health, Parke Davis, Smith Kline Beecham, and Stanley Medical Research Foundation; being a consultant for Abbott Laboratories, GlaxoSmithKline, Janssen, Lilly Research, Sanofi-Synthelabo, and UCB Pharma; and being part of a speaker's bureau for Abbott Laboratories, GlaxoSmithKline, Janssen, Lilly Research, and Pfizer. Dr. Culver reports receiving funding from Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, Eisai, Eli Lilly, GlaxoSmithKline, Pfizer, RepliGen, and Wyeth Pharmaceuticals. Dr. Ostacher reports receiving honoraria from AstraZeneca, Bristol-Myers Squibb, GlaxoSmithKline, Pfizer, Janssen, and Concordant Rater Systems and receiving research funding from Pfizer. The other authors report no competing interests.