The Epidemiologic Catchment Area study was the first large survey to demonstrate that addiction and mental disorders often co-occur in the general population and that only a minority of affected individuals seek professional help (
1 ). In addition, this study found that those with co-occurring mental and addictive disorders were more likely than those with either disorder alone to seek help (
2 ). Since that time these findings have been replicated by population surveys conducted across North America (
3,
4,
5,
6,
7,
8 ), Australia and New Zealand (
9,
10 ), and Europe (
11,
12 ).
The subgroup of individuals who meet the criteria for a disorder but have not sought professional help is of particular interest. With adjustment for illness severity, the proportion of those with a diagnosis who do not report that they have used services varies between 35% and 50% (
10,
13,
14,
15,
16 ). Aside from psychopathology, numerous attitudinal and sociodemographic factors are associated with perceived need for and use of mental health care (
17,
18,
19 ). It is not possible to equate unmet need with the proportion of those with a disorder who do not seek help (
20,
21 ). However, in health care systems that limit economic barriers to care, it is still of interest to examine why individuals who perceive a need for care do not seek help.
Population-based mental health survey research has adopted a diagnostic approach to the study of associations between mental health status and health outcomes or help seeking, although a role for dimensional measures of mental health status also has been recognized (
22 ). In contrast, population-based addiction research has tended to use dimensional measures of substance use and related problems, often to the exclusion of diagnostic information (
23,
24,
25,
26 ). Although there is little standardization across these studies in how measures are operationalized, substance use is consistently associated with the use of a variety of types of health services.
This study contributes to knowledge of the processes underlying help seeking by those with co-occurring mental and addiction disorders by examining relationships among need, service use, and satisfaction with mental health care in a population-based sample. This is the first study to examine these issues in a national Canadian setting. The research questions to be addressed include the following: Does the use of a comprehensive array of mental health services differ across past-year diagnoses of mental disorders and substance dependence? Do dimensional measures of substance use and mental health status contribute to the explanation of service use independent of diagnostic measures? Do the levels of satisfaction, perceived helpfulness, and unmet need differ across diagnoses?
Methods
Sample
Participants were respondents to the Canadian Community Health Survey (CCHS) Cycle 1.2 (N=36,984). The CCHS is a cross-sectional population health survey conducted biannually by Statistics Canada. Cycle 1.2, conducted in 2002, focused on mental health and well-being and was the first attempt to generate national estimates of the burden of mental illness in Canada. The target population included all noninstitutionalized adults 15 years of age and older living in the ten Canadian provinces, excluding those on Crown lands and military bases. Because this study was concerned with generalizing conclusions to the broad general population of Canada, the exclusion of these specialized populations was not expected to bias the results.
A multistage stratified cluster design was used to generate the sample. The response rate was 77%. The final sample was weighted to correspond to the general population of Canada (weighted N=approximately 24 million). A detailed description of the survey, including weight construction, is available elsewhere (
27 ).
Measures
The survey collected information on mental health and related problems, substance use and dependence and related problems, psychological well-being, and the use of mental health care and addiction-related care. The diagnostic content is based on the World Mental Health Composite International Diagnostic Interview (
28 ), which uses the diagnostic categories of the
DSM-IV (
29 ). Diagnostic algorithms were constructed for the past-year experience of five mood and anxiety disorders: major depression, manic episodes, panic disorder, social phobia, and agoraphobia. Past-year symptoms of substance dependence were assessed separately for illicit drugs and alcohol. Respondents were classified as positive for substance dependence if they reported three or more symptoms in the past year (
28 ). In our analysis, this information was combined to generate a four-level categorical variable describing diagnostic status: no disorder, 89.6% (approximately 22 million people); substance dependence alone, 2.1% (500,000 people); mental disorder alone, 7.4% (1.8 million people); and co-occurring disorders, .9% (200,000 people).
It should be noted that
DSM criteria for substance abuse, psychosis, and personality disorders were not included in the survey. Although this exclusion results in an underestimation of the burden of mental illness in Canada, the mental disorders covered in the survey are the most prevalent. The decision to exclude substance abuse from the survey was unfortunate; however, for the purposes of this study, it is likely that help seeking is more strongly related to the more severe dependence category (
6 ).
Respondents' pattern of substance use was characterized with three variables: average daily alcohol consumption, based on the number of standard drinks consumed on each of the past seven days; the frequency of heavy drinking in the past year, defined as five or more standard drinks per occasion; and past-year illicit drug use, excluding one-time use of cannabis. Mental distress was assessed with a self-reported general rating, which ranged from poor, rated 0, to excellent, rated 4, and the K-10 measure of generalized psychological distress (range=0–40, with higher scores indicating greater distress) (
30 ).
We grouped the types of mental health and addiction services examined into formal and informal sources. Formal care included hospitalizations and visits to psychiatrists, general practitioners, other physicians, psychologists, nurses, social workers, counselors, and spiritual advisors. Informal care included Internet-based support groups and chat rooms, self-help groups, and telephone helplines. Service use in the year preceding the survey was considered in order to match the time frame used to assess diagnostic status.
For each type of formal care, respondents rated their satisfaction on a 5-point scale that ranged from very satisfied, 1 point, to very unsatisfied, 5 points, and the perceived helpfulness of the service on a 4-point scale that ranged from helped a lot, 1 point, to not at all, 4 points. These measures were not available for informal care. Additional items assessed perceived unmet need for services, defined as occasions when respondents felt they needed help for mental health reasons or substance-related concerns but did not receive it.
Analysis
Preliminary descriptive analyses examined selected sociodemographic characteristics, alcohol and illicit drug use, mental distress, and mental health and addiction service use across diagnostic status. Formal and informal service use was cross-tabulated to examine the combination of different sources of care.
Logistic regression was used to examine associations between diagnostic status and service use. Three models were run to examine the use of any services, formal services, and informal services. The independent variable of primary interest was diagnostic status (reference category: no disorder). Restricting the sample to respondents who used at least one service in the year before the survey, we used a multinomial logistic regression to examine the number of services used across diagnostic status (one, two, and three or more services). Multivariate models were run to calculate the adjusted odds of service use across diagnostic categories, with controls for gender, age, education, and the dimensional measures of substance use and mental health status.
Three final logistic regression models examined associations between diagnostic status and satisfaction with care, perceived helpfulness, and unmet need for care. Among those who had used formal services, mean ratings were calculated and dichotomized for satisfaction and perceived helpfulness across all used services. Dichotomization was used because the distribution of these summary variables was skewed toward greater satisfaction and helpfulness. The third logistic regression estimated the odds of unmet need in the full sample, regardless of service use.
The analyses were conducted in SPSS 12.0 (
31 ) and Wesvar 4.2 (
32 ). Population weights constructed by Statistics Canada were used to account for nonresponse and to align the final sample with the Canadian population. To account for the complex survey design and potential for attenuated standard errors, all parameter estimates were bootstrapped.
Results
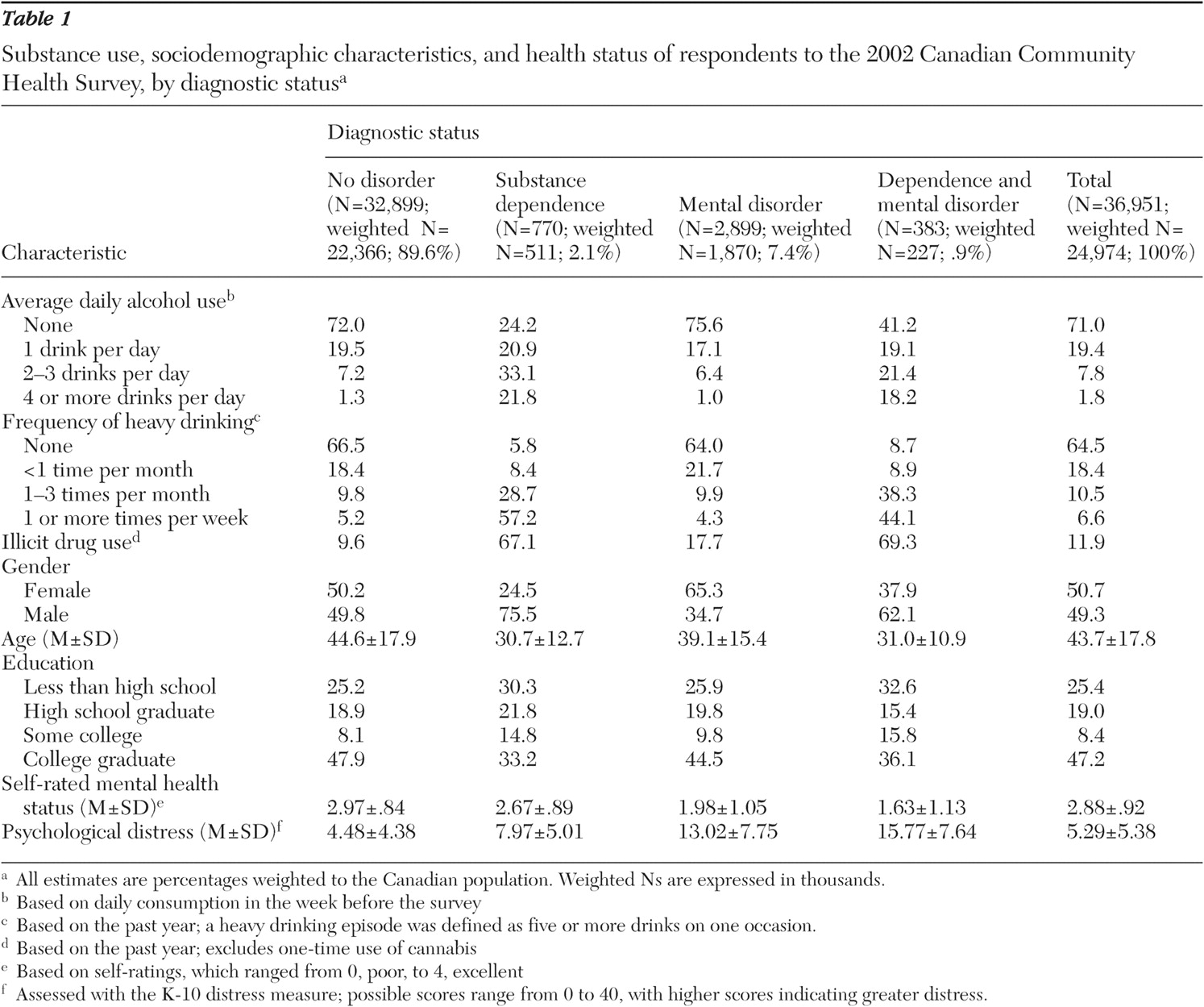
Table 1 describes alcohol and illicit drug use, sociodemographic characteristics, and mental distress across diagnostic status. As expected, those with substance dependence reported greater alcohol consumption and were more likely to report illicit drug use. Little difference was observed between those with substance dependence alone and those with co-occurring disorders. Men, younger individuals, and those with low levels of education were more likely to have substance dependence, both alone and co-occurring with a mental disorder, whereas women were more likely to meet the criteria for a mental disorder alone. Those with co-occurring disorders reported the poorest mental health status and highest psychological distress.
In total, 39% of those who met the criteria for a mental disorder or substance dependence had sought help.
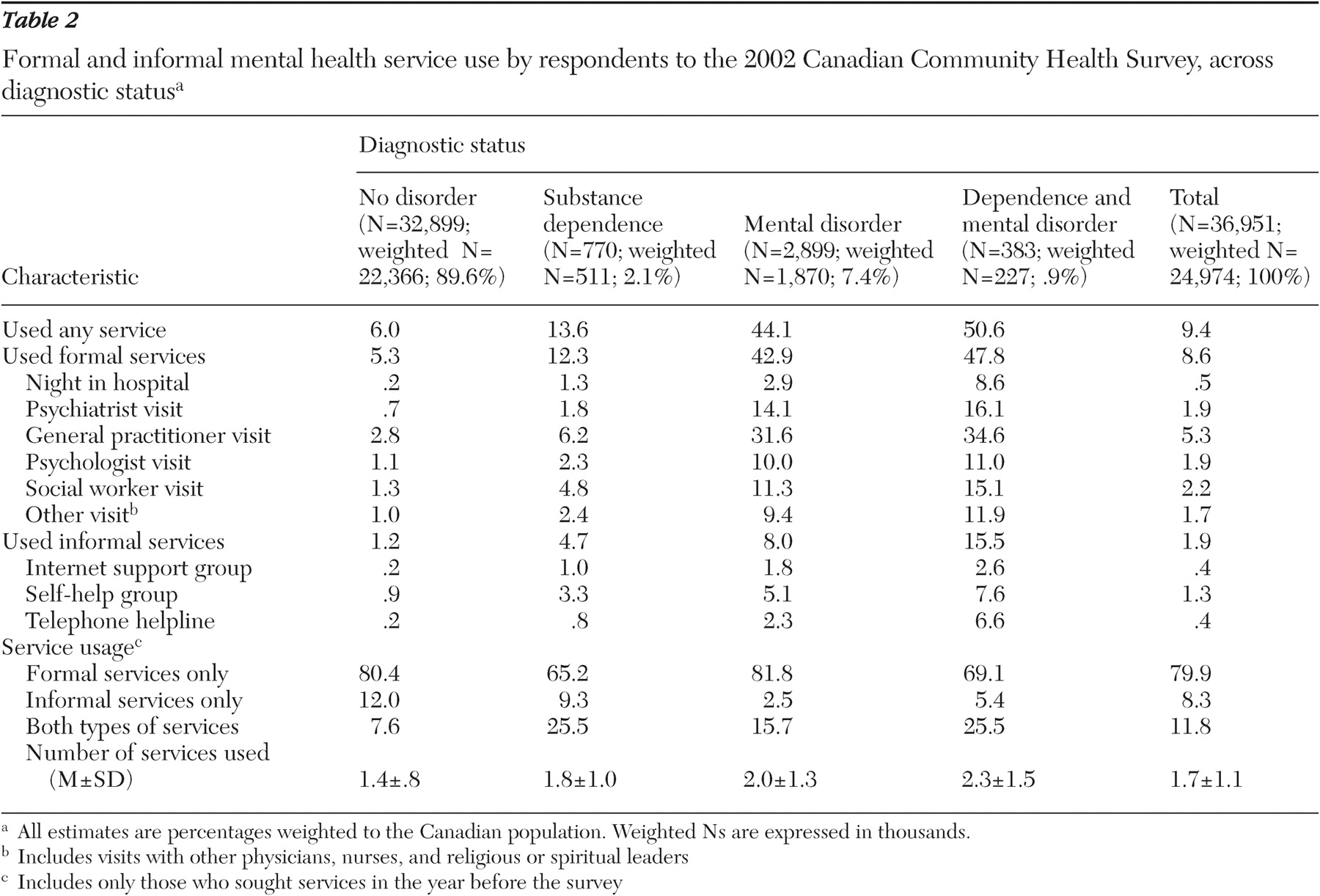
Table 2 describes service use in more detail. The likelihood of service use was clearly elevated among those with a mental disorder, with or without substance dependence. The most commonly used formal source of care was general practitioners. Of note, 27% of those who had used services in the prior year saw only a general practitioner. Among those who used at least one service in the year before the survey, a majority (80%) used only formal sources of care. Also, among service users, those with substance dependence and co-occurring disorders were more likely to report using informal services. There was not a great deal of variation across the groups in the mean number of services used, which varied from a low of 1.4 among those with no disorder, to a high of 2.3 among those with co-occurring disorders.
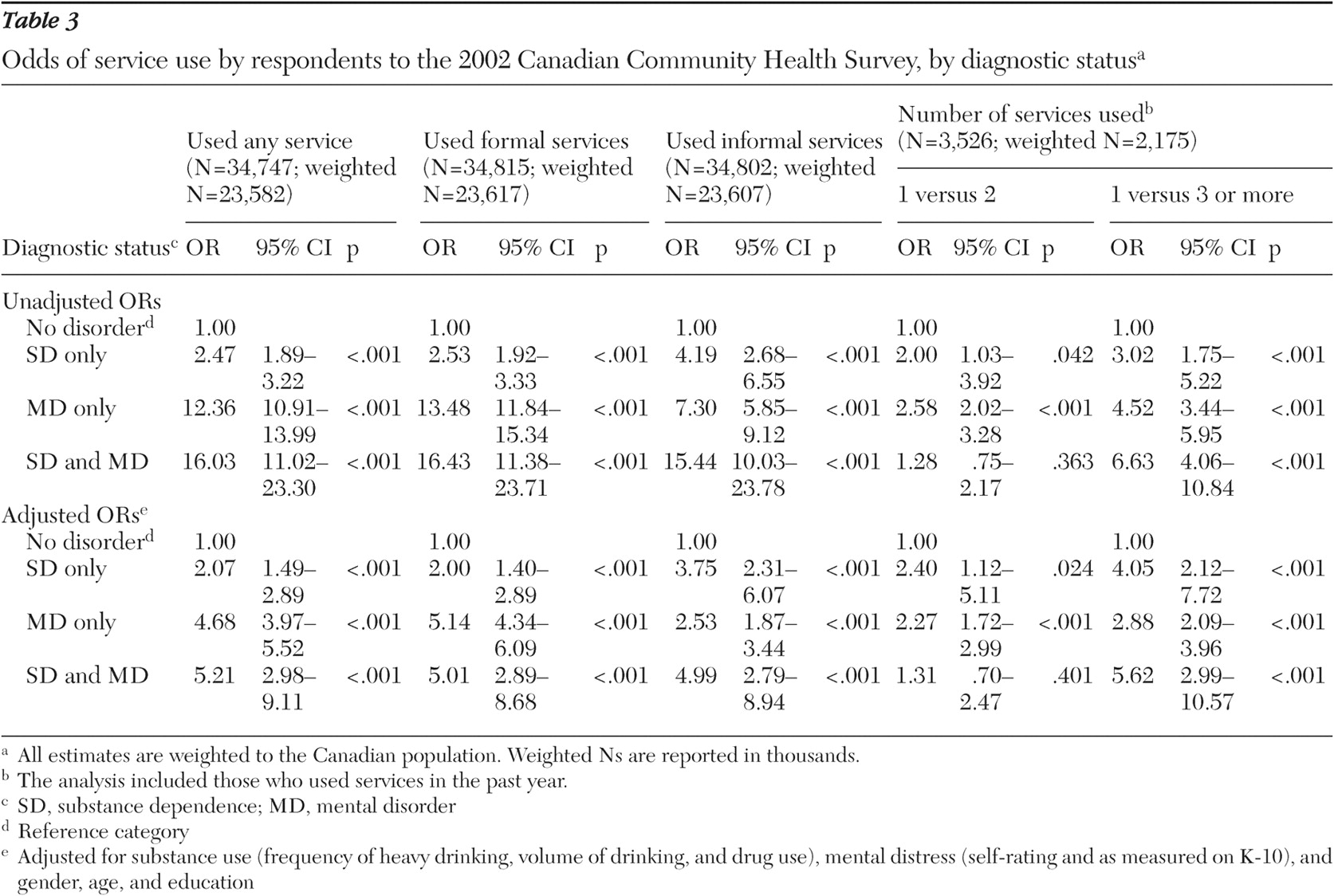
Table 3 summarizes the logistic regressions examining service use. The upper half of the table shows the unadjusted odds ratios for service use across diagnostic status. Regardless of the type of service, the odds of service use were significantly elevated for those with any diagnosis and were highest among those with co-occurring disorders. The odds of using any service or formal services showed an especially steep increase for those with a mental disorder, with or without substance dependence. Respondents with co-occurring disorders who used services had more than six times the odds of using three or more services relative to those with no disorder.
The adjusted odds of service use across diagnostic categories, with the analysis controlling for sociodemographic characteristics and dimensional measures of substance use and mental distress, are presented in the lower half of
Table 3 . The odds ratios were attenuated but remained statistically significant. Among the covariates (data not shown), illicit drug use, greater psychological distress, poorer mental health status, female gender, younger age, and higher education were significantly associated with the use of any service or formal services. Similarly, illicit drug use, greater psychological distress, poorer mental health status, and higher education increased the odds of informal service use, whereas consuming one drink per day on average reduced the odds of informal service use. Better self-rated mental health and lower education reduced the odds of using multiple services.
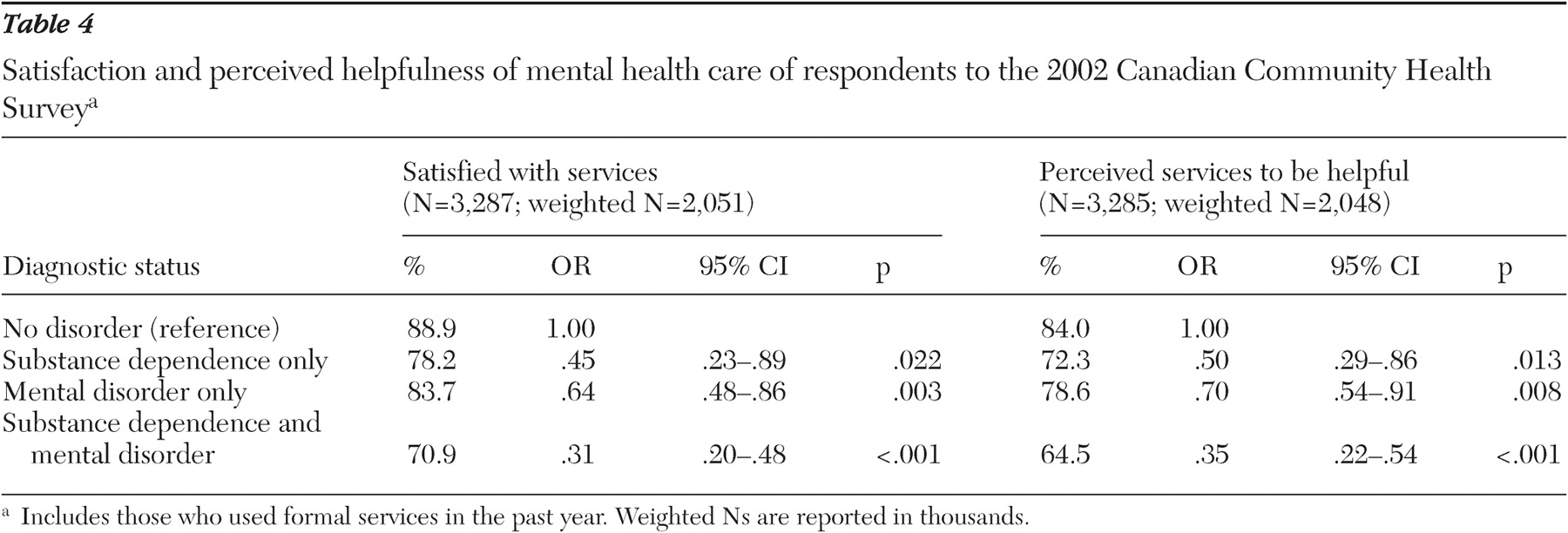
Table 4 presents the results on satisfaction and perceived helpfulness of services for the subsample who received formal care in the year preceding the survey. Most service users reported being satisfied with their care, although the prevalence varied across diagnostic groups, from a high of 89% among those with no disorder to a low of 71% among those with co-occurring disorders. A similar association was found for the prevalence of perceived helpfulness. These findings were supported by logistic regression, in which the odds of being satisfied or judging care to be helpful were significantly lower among those with any diagnosis, with the lowest odds observed among those with co-occurring disorders.
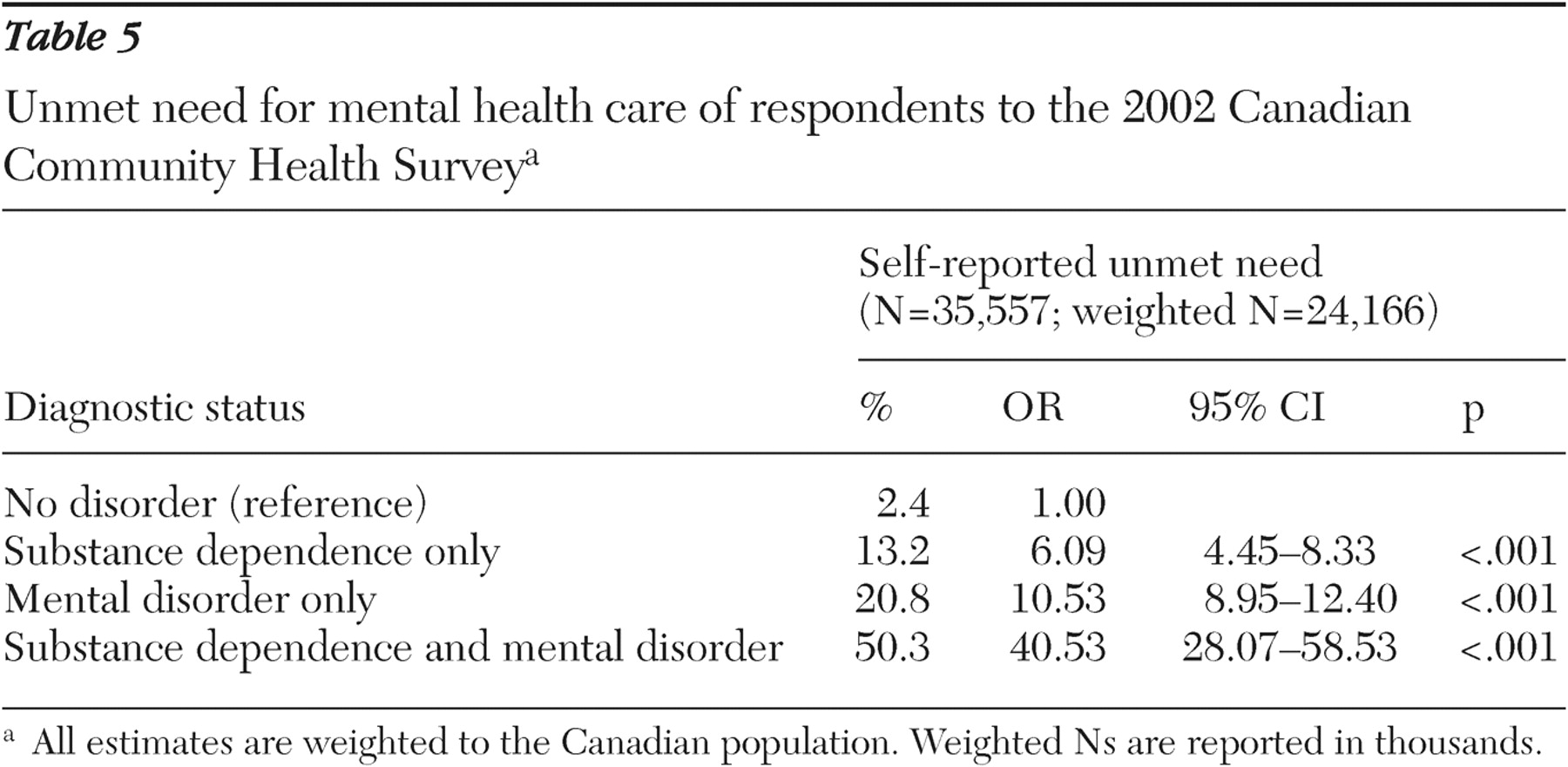
Table 5 illustrates the prevalence and odds of unmet need for mental health care across diagnostic status. The prevalence of unmet need was elevated among all diagnostic categories; however, it was especially high among those with co-occurring disorders. The odds of reporting unmet need among those with co-occurring disorders were four to seven times greater than among those with either disorder alone. Further analyses highlighted that the most common reasons for unmet need included preferring to self-manage symptoms (reported by 35% of respondents with unmet need), not getting around to seeking care (19%), not knowing how to get help (16%), and being afraid to ask for help (15%).
Discussion
Approximately 10% of all Canadians, and 40% of those with diagnosable disorders, sought help for mental health- or addiction-related concerns in 2001. This finding is comparable with estimates reported in population surveys conducted elsewhere (
6,
10,
11,
12,
14 ).
The most common source of help was general practitioners. This finding is also similar to those of previous studies (
6,
10,
11,
14,
33 ). It may be expected given the focus of such surveys on mood and anxiety disorders, excluding those such as psychosis, which are more commonly treated by specialists, as well as the exclusion of individuals in institutions. In this study, general practitioners were the sole care provider for approximately one-quarter of those with a mental or an addictive disorder who sought services in the year before the survey. Because this survey did not consider the adequacy of care, it is not possible to speculate on whether this finding speaks to the effectiveness of care provided by general practitioners or of barriers to accessing specialized care. Other studies have noted that mental health care received in primary care settings is less likely to be concordant with therapeutic guidelines than care received in specialist mental health settings (
6,
34,
35 ).
General practitioners have themselves reported concerns over limited training in assessment, treatment, and referral for mental and addiction disorders, as well as insufficient integration with specialized care providers (
36,
37,
38,
39 ). Considering their central role in providing services to this population, further research is needed to examine the adequacy and effectiveness of primary care for addiction and mental disorders. Notably, a recent study from the United States reported on the increasing frequency of use of mental health care services from the general medical sector alone (
40 ).
Informal services, such as self-help groups, were used less frequently than formal sources of care, and only a minority reported using only informal care. A similar minority reported using both informal and formal sources of care. The relatively higher use of informal care among those with substance dependence who used services is likely related to the popularity of self-help groups such as Alcoholics Anonymous.
Consistent with previous studies, respondents with co-occurring disorders had greater odds of using services than those with either disorder alone (
2,
3,
7,
8,
12 ). Notably, the association between substance dependence and help seeking, although significant, was small relative to that for mental disorders and help seeking. Those with substance dependence also rated their mental distress as higher than that of those with no disorder but lower than those with mental disorders. Previous studies have noted a lower impact of addiction disorders on disability (
7,
18,
41,
42,
43 ), perceived need for care (
18,
19 ), and help seeking (
13,
14 ) relative to mood and anxiety disorders. The experience of substance problems in the general population may therefore play a relatively minor role in bringing people into care. Alternatively, it is possible that personal factors, such as lower motivation, and societal factors, such as greater stigma and negative attitudes, are barriers to seeking and receiving care for substance-related concerns (
44,
45 ).
Different traditions have emerged in population-based research on mental and addiction disorders with respect to the use of diagnostic versus dimensional measures of problems. Although diagnostic information is characterized by greater standardization, thus facilitating cross-study comparisons, studies using dimensional measures are able to examine the impacts and outcomes of risky drinking and drug use behaviors among those who do not necessarily meet dependence criteria. Elsewhere, elevated alcohol consumption and episodic heavy drinking were associated with the experience of substance problems (
46 ) and the use of health services (
23,
24,
26 ). In this study, these measures did not contribute to the rate of help seeking when symptoms of dependence were controlled. Past-year illicit drug use was associated with greater odds of help seeking, indicating that drug use may specifically affect perceived or real need for care over the experience of dependence symptoms. It is possible that legal, other institutional, and informal pressures to enter treatment may be stronger for users of illicit drugs than for users of alcohol, a less stigmatized psychoactive substance. These pressures may also be more urgent for illicit drug users than for drinkers (that is, given ultimatums between treatment and jail).
Among those who used mental health care services in the year preceding the survey, a majority (65%–89%) of individuals were satisfied with the care they received (71%–89%) and perceived it to be helpful (65%–84%). Although this remained true across diagnostic categories, the prevalence of satisfaction and perceived helpfulness was lowest among those with co-occurring disorders. Satisfaction with care can affect compliance, treatment outcomes, and future patterns of help seeking (
47,
48 ). Further research is needed to examine sources of dissatisfaction among those with co-occurring disorders, including specific types of care and providers. Of note, this finding may speak to system-level inadequacies in the management of co-occurring disorders (
44,
45,
49 ). It is again possible to speculate on the role of personal factors, such as poor motivation or care preferences (for instance, dissatisfaction with a care plan that involves medications negatively viewed as substitutes for substances of abuse), as well as stigma and the attitudes of professionals on consumer satisfaction with the process of care (
44 ).
The proportion of those reporting unmet need for care was also highest among those with co-occurring disorders. The magnitude of the difference in unmet need between those with mental and co-occurring disorders relative to the difference in help-seeking rates makes it unlikely that this finding resulted from greater help seeking and, therefore, greater overall exposure to the health care system. The most commonly reported barriers were related to the acceptability of care, including a preference for self-managing symptoms. This finding is similar to previous reports (
50 ) and is consistent with studies documenting the discord between perceived need for care and impairment (
17,
18,
19 ).
As the data are cross-sectional, it is not possible to determine causal relationships between the experience of disorders and use of services and the potential impact on prognosis. It also was not possible either to identify the disorder that initiated help seeking or to empirically examine the role of provider factors on the help-seeking process. Diagnosis and caregiver biases, which may depend on factors such as education and previous clinical experience, are likely to have implications for service use, satisfaction, and unmet needs. Finally, the 12-month recall period for service use is not considered to be optimal from the perspective of reporting accuracy (
51 ); however, this is the time frame most commonly used in similar surveys and, importantly, corresponds to the diagnostic information. In general, studies of the accuracy of self-reported service use data have found that stigmatized care, including mental health visits, are underreported (
51 ).
Conclusions
As expected from previous community and treatment studies, individuals with co-occurring disorders accounted for a significant proportion of those seeking care for mental health and addiction issues. However, in Canada, as elsewhere, there is currently a low level of coordination between these two sectors of care (
52 ). The potential for specialized care for co-occurring disorders in terms of acceptability to consumers and impact on outcomes is promising (
53,
54,
55 ) and should be further explored. The differential use of services, satisfaction with services, and unmet need across diagnostic status allow for speculation on differing levels of disability and stigma in the help-seeking process for different types of disorders.
The association between comorbidity and unmet need is particularly troubling, and an additional study investigating this association in more detail is under way. Future research should address why services are considered to be unsuitable or unnecessary to some Canadians, examining the roles played by care preferences, illness severity, stigma, and service arrangements. Research is also required to specifically address the nature of the disorders that bring people into the system and any differential barriers to care, so as to increase our understanding of the association between need and demand for mental health care.