Although many if not most homeless individuals have had past involvement with the criminal justice system (
1,
2,
3,
4,
5,
6 ), little attention has been paid to determining the risk of homelessness among jail inmates, compared with the general population, or to determining how jail inmates who had been homeless differ from other inmates. Some researchers have reported that the criminal activities of homeless individuals are predominantly minor crimes that directly result from their efforts to survive on limited resources—for example, breaking into buildings or stealing (
6,
7,
8 ). Several studies, however, have also found substantial rates of criminal justice system involvement for major crimes among homeless populations (
2,
9,
10,
11,
12 ). Although such crimes may reflect survival strategies (
7,
13,
14,
15 ), it is also likely that people who have been incarcerated for crimes in the past are at greater risk of homelessness after they have completed their sentences (
1,
16 ).
Homeless individuals may also be more likely to have health conditions that may increase their risk of involvement in the criminal justice system. Substance abuse—highly prevalent in the homeless population and often associated with involvement in the criminal justice system (
1,
2,
3,
7,
8,
9 ) through arrests for drug possession or sales or for public intoxication (
1,
6,
7,
8,
10,
11 )—may also increase the risk of violent crime (
17 ).
Severe mental illness is also more prevalent among homeless people than in the general population (
5,
12,
18,
19,
20,
21 ) and has been associated with increased risk of involvement with the criminal justice system (
6,
12,
22,
23 ), particularly for violent crimes (
22,
23 ). People with severe mental illness may be less able to cope with the stresses of homelessness (
23,
24 ) or may perpetrate criminal acts that are manifestations of their illness (
17,
25 ).
The sociodemographic characteristics of homeless individuals—such as being male, single, young, poor, from a minority ethnic group, or poorly educated—may also be associated with both homelessness and the risk of involvement with the criminal justice system. Some previous research, however, has failed to find differences in these measures between homeless and domiciled individuals involved in the criminal justice system (
11,
15,
20,
22,
23,
26,
27,
28,
29 ).
Most prior research in this area has examined past criminal justice involvement of currently homeless people by using data collected from community homeless samples and provides little information beyond prevalence rates of past criminal justice system involvement.
The study presented here sought first, to investigate the relative risk of recent homelessness among current jail inmates, compared with the general population, standardized to the age, race and ethnicity, and gender distribution of the jail sample. In contrast to prisons, jails are penal institutions for the immediate, largely shorter-term confinement of people pending arraignment, trial, or sentencing or the confinement of individuals who are serving time for less serious crimes. Second, we sought to explore the relationship between homelessness and jail incarceration by examining factors that differentiate homeless and domiciled jail inmates.
We thus examined whether in comparison to domiciled jail inmates, inmates who have been homeless are currently incarcerated for offenses that can be characterized as resulting from efforts to survive with limited resources; are more likely to have clusters of symptoms indicating mental illness and substance abuse, a mental health diagnosis by a clinician, or greater mental health service use; have greater past criminal justice system involvement; or have distinctive sociodemographic disadvantages. The relatively few studies that have examined these issues through inmate surveys have been limited to nonrandom and small samples with narrow geographic coverage and have not focused on jail inmates; instead, they focused on prison inmates. This study is thus the first of which we are aware that used data from a national jail survey to investigate the prevalence and correlates of recent and past homelessness among jail inmates.
Methods
Data source
The data presented here are derived from the 2002 Survey of Inmates in Local Jails carried out by the Bureau of the Census for the Bureau of Justice Statistics of the U.S. Department of Justice (
30 ) to provide nationally representative data on jail inmates. Because these data are in a public access data set with all identifying information removed, it was not necessary to obtain informed consent or institutional review board approval. The interviews were conducted from January to April 2002 (
30 ).
The sample design for the survey was a stratified two-stage selection, with jails selected first and inmates then chosen from those in the selected jails. In the first stage of sample selection, jails were divided into six strata on the basis of the size of the male, female, and juvenile populations in each jail. All the jails from the largest two strata were selected: 38 jails containing more than 40 juvenile inmates with unspecified additional adults and 191 jails containing 40 or fewer juvenile inmates along with more than 1,500 adult male inmates or more than 75 adult female inmates. A total of 231 more jails were selected from 3,136 jails in the remaining four strata, making a total sample of 465 jails. Specifically, one of every three jails was selected from the third stratum (jails holding between 501 and 1,500 adult male inmates); one of every four jails was selected from the fourth stratum (jails holding between 201 and 500 adult male inmates); one of every 13 jails was selected from the fifth stratum (jails that held between 41 and 200 inmates); and one of every 74 jails was selected from the sixth and final stratum, the stratum of jails with the smallest population of inmates (less than 40 male inmates) but with the largest number of jails.
Although the jails in each stratum differed in size, roughly equal numbers of inmates were in the jails selected from each strata. Interviews were conducted in only 417 of the jails, because 39 refused and nine were either closed or had no inmates to survey.
In the second stage of sample selection, 7,750 jail inmates were randomly selected from a list provided by each jail—one of every 92 males, one of every 27 females, and one of every 12.6 juveniles. A total of 6,982 interviews were completed because 263 inmates refused to participate, 407 were released after sampling, and 98 could not be interviewed because of medical, security, or other administrative reasons. Thus the inmate nonresponse rate was 9.9% among those approached for surveys. Each interview was an hour long and based on computer-assisted personal interviewing. Inmates were assured of confidentiality. Further study details can be found in the survey documentation (
30 ).
The survey was weighted to account for the sampling design and nonresponses, so the sum of all sample weights would equal 631,241—the total number of inmates estimated to be in local jails using the 2001 Annual Survey of Jails. We proportionally downweighted the sample so our statistical tests would not be overly sensitive to the large estimated population—for example, if the entire population, rather than the available sample of that population, were used, the statistical power of analyses would likely lead to all of the results being significant. A new weight measure was created by dividing the existing final weight by the average number of inmates represented by each case (that is, 631,241/6,982=90.41). Use of the new, smaller weights resulted in the number of cases being used for analyses differing little from the original sample size—that is, the number of cases was adjusted only for sampling design and nonresponses. We also restricted the sample to individuals aged 17 years and older. After removal of juveniles and downweighting, 6,953 cases were available. Data were missing for 491 cases, so 6,462 cases were used for the analyses.
Measures
Housing status. A categorical measure was constructed that had a value of 0 if the inmate was never homeless (that is, living on the street or in a homeless shelter) during the year before incarceration, a value of 1 if the inmate reported a period of homelessness in the year before incarceration but not at the time of incarceration, and a value of 2 if the inmate was homeless at the time of his or her incarceration. Two dichotomous indicators based on this measure represented whether each inmate had a period of homelessness in the year before incarceration or had been homeless immediately before his or her incarceration.
Crime. Five measures classified the current controlling offense (that is, the reason for the current incarceration): violent crime, property crime, drug use, public disorder, or other crime. The survey designates one offense for each inmate as the "controlling offense." If an inmate is incarcerated for multiple offenses, the controlling offense is the crime that resulted in the longest or most severe maximum sentence. Two dichotomous indicators were also constructed to represent whether the inmate had a criminal record for a violent or a nonviolent offense in the past—that is, whether for either type of offense he or she had been arrested, sentenced to probation, or served time.
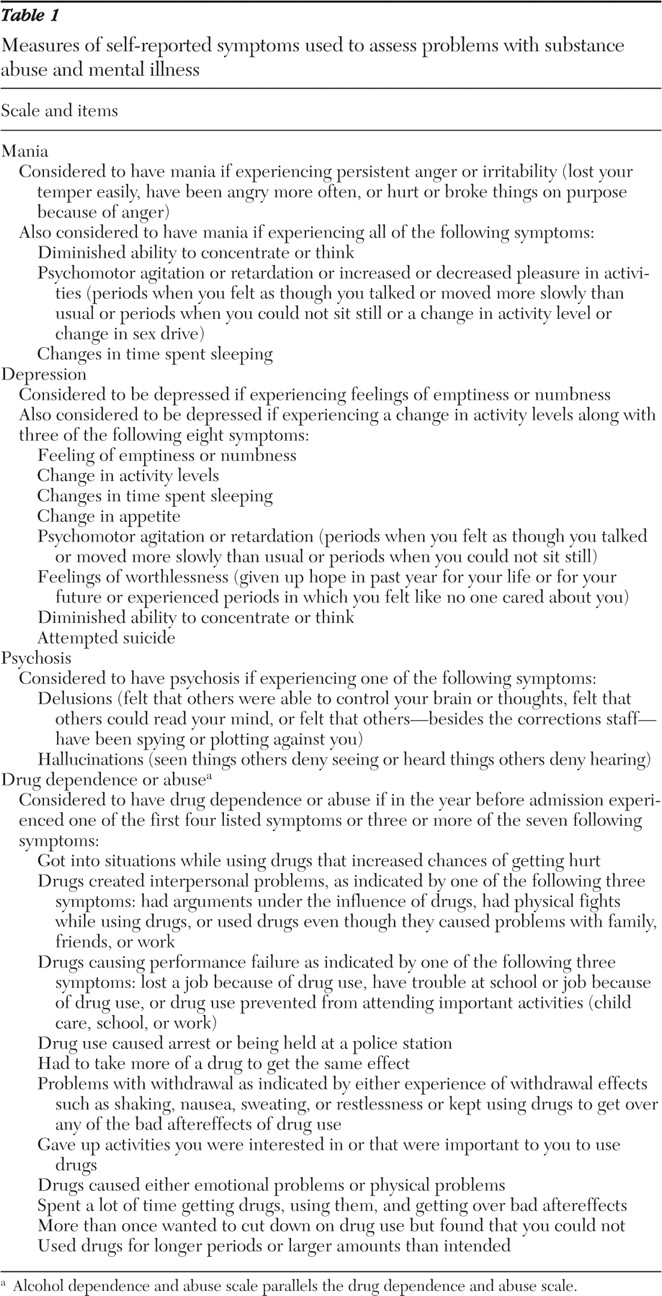
Mental health and substance abuse. Five measures used self-reported symptoms to assess problems with substance abuse and mental illness. One measure was based on whether each inmate currently had a cluster of symptoms that indicated difficulty with drug abuse or dependence and another if he or she had a cluster of symptoms that suggested problems with alcohol abuse or dependence. Three additional measures were created that indicated whether inmates had clusters of symptoms associated with each of three specific mental illnesses: depression, mania, or psychosis. These five measures do not represent clinical or research diagnoses, because the Department of Justice 2002 Survey of Jail Inmates did not assess the severity or duration of the symptoms or the distress caused by the illness and because no exclusions were made for symptoms resulting from medical illness, bereavement, or substance abuse.
Table 1 provides details of the algorithms used to construct these measures. Scales used in the table are based on a Bureau of Justice Statistics special report that used the 2002 Survey of Inmates in Local Jails (
30 ) and on personal communications with the authors of the report (James DJ, Glaze L, personal communications, Jan 2007–Feb 2007).
Three additional measures reflected mental health service use in the year before arrest and since incarceration: treatment in a mental hospital or other treatment program, receipt of psychotropic medications, and receipt of professional counseling. A measure was also created to indicate whether the inmate had been told that he or she had a mental health diagnosis within the past year.
Demographic characteristics. A series of measures was created to represent gender, marital status, current employment, veteran status, education (at least a high school degree or GED), and earnings of greater than $1,000 per month before incarceration. An additional measure represented tenure in jail of less than one month. Additional dichotomous indicators were used to represent age in four categories along with race and ethnicity (black, white, other, or Hispanic). Individuals could be coded as belonging to one or more racial or ethnic groups.
Trauma. Several measures were also created to indicate whether the inmate had ever experienced trauma, including being shot at (excluding military combat), attacked with a knife or other sharp object, sexually abused, or physically abused. Two additional variables addressed whether the inmate had been physically or sexually abused as a minor.
Analyses
Analysis proceeded in three steps. First, we computed the risk ratio for homelessness in the previous year among jail inmates, compared with the general population.
Next, we performed a series of bivariate chi square tests to examine whether significant relationships existed between homeless status and current and past criminal justice experience; homeless status and the presence of symptom clusters associated with mania, depression, psychosis, depression, and substance abuse; and homeless status and other indicators of mental illness, sociodemographic characteristics, or traumatic experiences.
Finally, two multivariate logistic regression comparisons were undertaken. In the first we compared inmates who had been homeless at all in the year before incarceration with those who were not homeless. In the other comparison we examined the differences between prisoners who experienced an episode of homelessness in the year before incarceration and prisoners who had been homeless at the time they were incarcerated. Both models included measures of criminal justice system involvement; the presence of symptom clusters associated with mania, depression, psychosis, and substance abuse; whether a clinician gave a mental health diagnosis in the past year; and mental health service use, sociodemographic characteristics, and trauma history. Forward stepwise selection of variables was used. The criterion for entry into the model was p≤.05, and for removal it was p<.05. All statistical modeling was done with the procedure PROC LOGISTIC of the SAS software system, version 8.0.
Results
Rates of homelessness
Altogether, 84.7% of our downweighted sample of U.S. jail inmates (N=6,462) were domiciled (that is, were not homeless) throughout the year before incarceration; 12.4% had been homeless in the previous year, although not at the time of incarceration; and 2.9% were homeless at the time of incarceration. The proportion of all individuals in jail who had been homeless was 15.3%. We estimated the annual rate of homelessness to be 1.36% to 2.03% in 1996, after standardization of the general population sample to the age, gender, and race or ethnicity distribution of the jail sample (
32,
33,
34,
35 ). Thus the rate of homelessness among jail inmates was approximately 7.5 to 11.3 times the annual rate of homelessness in the general population.
Sample characteristics
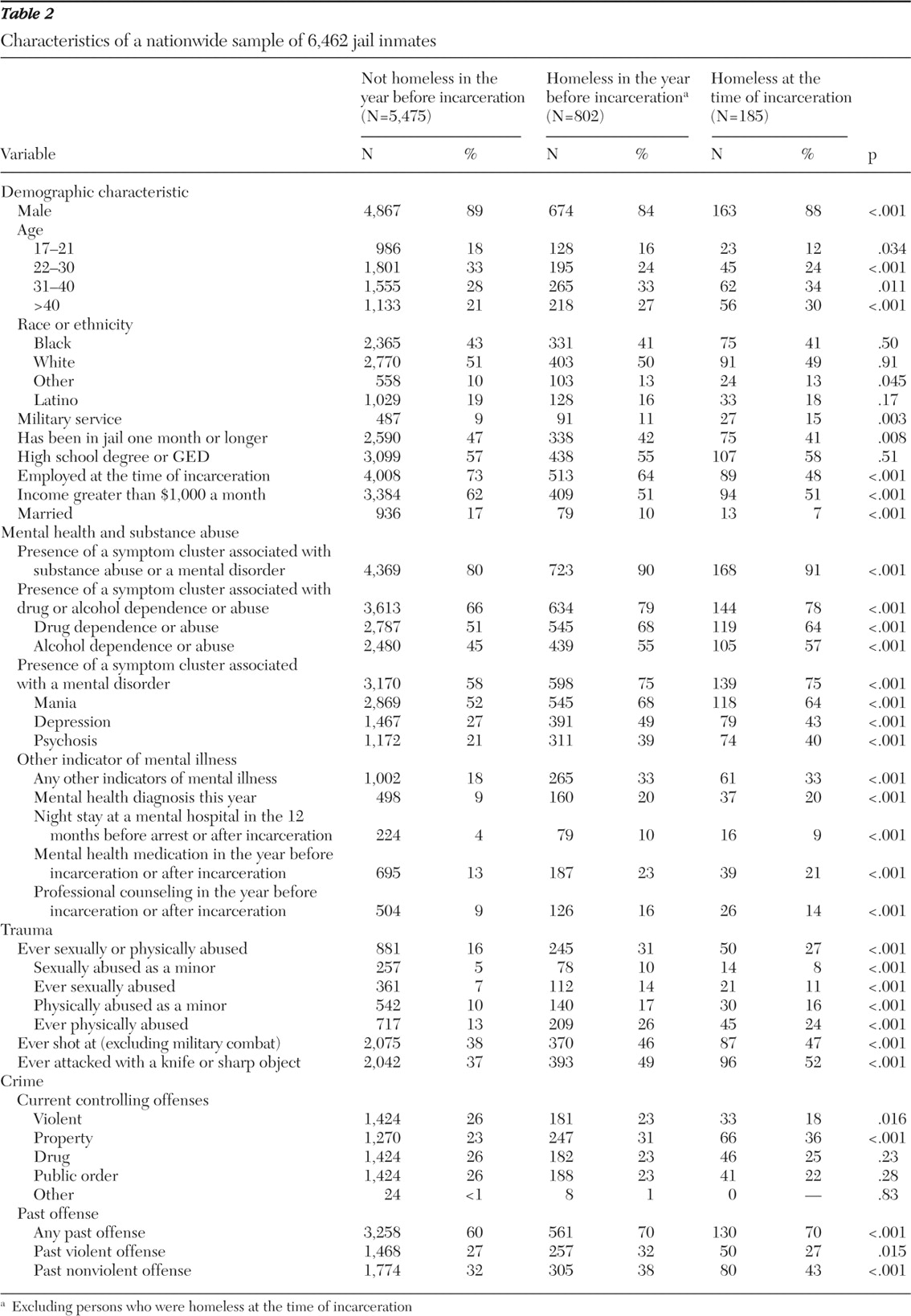
Chi square tests indicated that on most measures there were significant differences between inmates who were domiciled the year before incarceration, inmates who had an episode of homelessness, and those who were homeless immediately before incarceration (
Table 2 ). In comparison with domiciled inmates, inmates in the two homeless groups were significantly more likely to be currently incarcerated for a property crime and less likely to be currently incarcerated for a violent crime. However, homeless inmates were more likely to have a criminal history of both violent and nonviolent offenses.
Symptom clusters associated with mania, depression, psychosis, and substance abuse were common among all inmates but were significantly more prevalent among homeless inmates, with rates 10% to 22% higher among homeless inmates. The rate at which homeless inmates reported other indicators of mental illness was also 15% higher than that among domiciled inmates (33% versus 18%). Consistent with these results, homeless inmates were significantly more likely to report use of mental health services or of medications for a mental illness.
The three groups of inmates were not significantly different in education or on indicators of race and ethnicity, with the exception of significant but slight differences with respect to the other racial category, and although the inmate groups significantly differed with regard to gender and past military service, these differences were very small.
For several other sociodemographic characteristics, there were substantial and significant differences among the three groups of inmates. Employment among inmates who had been homeless in the previous year was 9% lower than that among inmates in the domiciled group, whereas employment among those who were homeless at the time of incarceration was 25% lower than that among inmates in the domiciled group. The proportion of the homeless inmates who had an income of greater than $1,000 a month was approximately 10% lower than among inmates in the domiciled group. Homeless inmates were also significantly older but less likely to be married.
Furthermore, homeless inmates were significantly more likely than domiciled inmates to have been exposed to all categories of trauma, specifically to have been sexually or physically abused.
Multivariate logistic regression
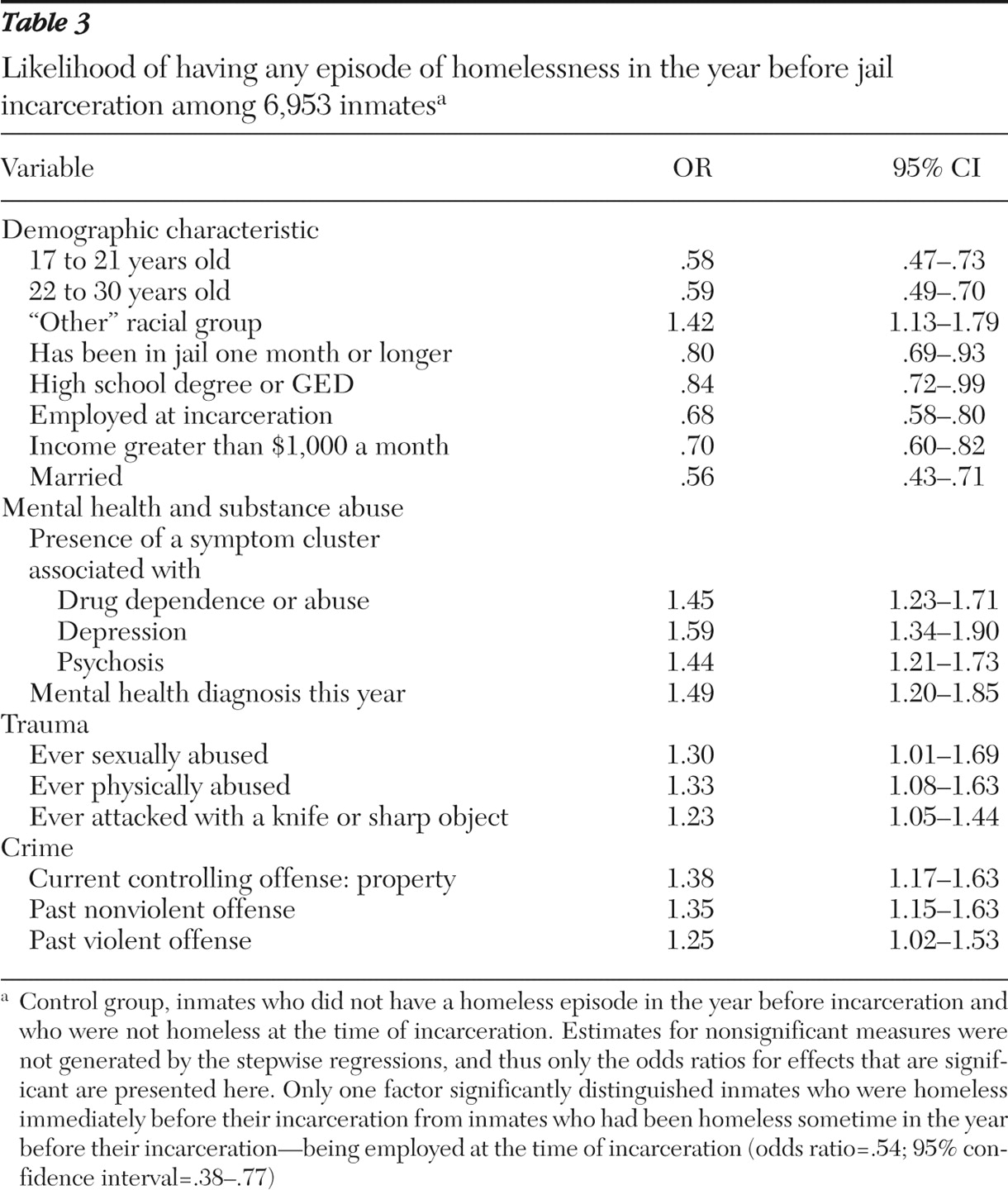
The results of multivariate analyses of whether the inmate had experienced any episode of homelessness before incarceration were similar to the results of the bivariate analyses (
Table 3 ). Indicators of mental health problems and substance abuse problems were the strongest predictors of homelessness. Respondents who reported clusters of symptoms associated with drug dependence or abuse, depression, or psychosis or those who had received a mental health diagnosis in the past year were approximately one-and-a-half times more likely to have been homeless. After the analyses adjusted for other factors, service use and taking medications were not independently associated with homelessness.
Having committed a property crime at the time of incarceration increased the odds that an inmate had been homeless (odds ratio [OR]=1.38), as did having a previous record of having committed either a nonviolent offense (OR=1.35) or a violent offense (OR=1.25).
Having been in jail longer than one month (OR=.80) and several sociodemographic assets were negatively associated with having been homeless, specifically having finished high school or having a GED (OR=.84), being employed (OR=.68), having a monthly income of greater than $1,000 a month (OR=.70), and being married (OR=.56). Additionally, inmates in both the 17- to 21-year-old age group (OR=.58) and the 22- to 30-year-old age group (OR=.59) were less likely than inmates older than 30 years to have been homeless.
Past episodes of either sexual abuse (OR=1.30) or physical abuse (OR=1.33) were also associated with an increased likelihood of homelessness, as was a past episode of having been attacked with a knife or another sharp object (OR=1.23).
Homelessness at incarceration
Only one factor significantly distinguished inmates who were homeless immediately before their incarceration from those who had been homeless sometime in the year before their incarceration. Being employed at the time of incarceration reduced the odds by about half of being homeless immediately before incarceration.
Discussion
In this study, data from a large national survey were used to examine the rates and correlates of homelessness among adult jail inmates. The rate of recent homelessness among U.S. jail inmates was found to be very high (15.3%), approximately 7.5 to 11.3 times higher than that found in the general population, after standardization to the age, race or ethnicity, and gender distribution of the sample. In comparison with other inmates, homeless inmates were not only more likely to be currently incarcerated for a property crime but also more likely to have past criminal justice system involvement for both nonviolent and violent offenses and to have mental health and substance abuse problems and a lack of personal assets.
Past studies of individual jails and city jail systems have found higher rates of homelessness than we did, ranging from 7.8% to 20% of persons who were homeless at the time of incarceration (
20,
21,
36 ) and 25% to 33% of persons who had an episode of homelessness in the two months before incarceration (
20 ). The lower rate we observed in the national sample used in this study probably reflects the representation of rural areas (in addition to urban areas) in this sample. Rural areas have lower rates of homelessness than urban areas. However, there is agreement between this study and earlier research that regardless of where they are incarcerated, jail inmates have much higher homeless rates than the general population.
In addition to estimating the relative risk of homelessness, we explored several factors associated with homelessness among jail inmates, including crimes related to efforts to survive with limited resources, health conditions, and demographic characteristics. The controlling offense of homeless individuals was more likely to be a property crime, suggesting that their most recent incarceration may have resulted from "survival behavior." But homeless inmates were also significantly more likely to have committed violent and nonviolent crimes in the past and had many other problems, suggesting that coping with the material stresses of homelessness is not the only factor putting them at risk of incarceration. This finding is consistent with some previous studies that have reported more frequent histories of adolescent antisocial behavior among homeless people (
2 ).
There were also clear indications that both mental illness and substance abuse indicators were associated with greater risk of homelessness among jail inmates and that substance abuse appears to be the stronger risk factor for incarceration among both homeless and nonhomeless inmates. Among jail inmates the rates of substance abuse were 2.4 to 3.7 times higher than rates of mental illness. In contrast, results of the National Comorbidity Study (
37 ), a national epidemiological study of noninstitutionalized Americans, found that the rate of mental illness was approximately eight times the rate of substance abuse. Although the measures used in our survey and the National Comorbidity Study are not strictly comparable, there seems to be a dramatic preponderance of addictive diseases in the jail population in contrast with the nonincarcerated adult population.
The association of mental illness with homelessness among jail inmates may reflect limited access to mental health services, particularly inpatient services. Over the past 50 years, psychiatric hospitalization has become far less available because of reductions in bed availability (
17,
36 ) as well as high legal standards for involuntary mental hospitalization (
8,
17,
25,
38,
39,
40 ). Additionally, when homeless individuals with a serious mental illness commit a crime, the police may not readily identify their illness as a precipitating risk factor (
17,
38,
40,
41 ).
As expected, homeless inmates were also more likely to be unemployed and unmarried and to have lower incomes and less education. Unexpectedly they were older, and race and ethnicity did not differentiate homeless and domiciled inmates, suggesting that among jail inmates, blacks and Hispanics are at similarly high risk as non-Hispanic whites for homelessness, at least at the national level.
Our results thus provide evidence that all three factors—past criminal justice system involvement, mental illness and substance abuse, and lack of sociodemographic assets—are major contributors to the high rate of homelessness among jail inmates, which implies that the effort to survive with limited resources through criminal acts is not the predominant factor contributing to the incarceration of homeless individuals. In fact, the greater age of homeless inmates and their more extensive criminal histories suggest that past incarceration, even before they became homeless, may have been a major risk of subsequent homelessness. Incarceration has been noted to increase the risk of homelessness by weakening community and family ties, as well as by severely limiting opportunities for employment and access to public housing (
1,
42 ). It is thus possible that, as others have suggested, a sizable proportion of homeless jail inmates became homeless in part as a result of prior incarceration (
4,
43 ). This bidirectional association between homelessness and incarceration may result in a certain amount of cycling between public psychiatric hospitals, jails and prisons, and homeless shelters or the street (
4,
43 ).
Three potential limitations to our conclusions deserve comment. First, our sample did not include individuals who had committed more serious crimes, because the 2002 Survey of Inmates in Local Jails did not include individuals who were incarcerated in state or federal prisons. However, it is useful to analyze data on jail inmates separately from data on prison inmates, because jail inmates are "closer" to the community from which they originally came as a result of having shorter sentences. A second limitation of our study is that it relies entirely on self-report data that may not be precise or well validated, especially as concerns mental illness and substance abuse diagnoses. Lastly, the five measures of mental health and substance conditions were based on clusters of symptoms and were not diagnostic measures because, as stated above, the Department of Justice did not assess the severity or duration of the symptoms or the distress or dysfunction caused by the illness and because no exclusions were made for symptoms resulting from medical illness, bereavement, or substance abuse. However, clusters of DSM-IV mental health and substance abuse symptoms do provide informative indications of mental health and substance abuse status.
Conclusions
Regardless of the above limitations, this study adds to our understanding of incarceration among homeless jail inmates. This study documented the much higher rates of homelessness among jail inmates, compared with the general population. Additionally, evidence was provided for the role of prior criminal justice system involvement, poor health status, and the lack of sociodemographic assets in increasing the rates of homelessness among jail inmates.
Acknowledgments and disclosures
The authors report no competing interests.