Between 1981 and 2005 more than 50,000 persons were living in nonmetropolitan statistical areas of the United States (that is, communities of 50,000 residents or fewer) when they were diagnosed as having AIDS, accounting for 6% of all AIDS cases (
1 ). Several studies portend that persons in rural areas living with HIV-AIDS experience increased levels of depressive symptoms, suicidal ideation, loneliness, and difficulty accessing health care and social services (
2,
3 ). Moreover, persons living with HIV-AIDS in rural areas have significantly shorter survival periods than their urban counterparts (
4 ). High rates of depression and loneliness among HIV-infected persons in rural areas are disconcerting because these factors are associated with more rapid disease progression and greater mortality (
5,
6 ).
Given the growing number of HIV-infected persons in rural areas, there is an urgent need to provide psychological services to this population. Unfortunately, geographic isolation, physical limitations, and confidentiality concerns preclude many from accessing these services (
7,
8 ). Telephone-based interventions can circumvent many of these barriers and reach individuals who have limited or no access to mental health services.
A meta-analysis by Mohr and colleagues (
9 ) found that telephone-delivered interventions are well-received and reduce depressive symptoms. They found significant symptom reductions across all assessment periods for patients enrolled in telephone-administered psychotherapy, compared with treatment as usual (d=.26); greater reductions were found when analyses were limited to changes from pre- to postintervention (d=.82). Moreover, the mean attrition rate in the 12 studies reviewed was 7.5%, markedly lower than attrition found in similar face-to-face interventions (range=14% to 65%).
One interpersonal psychotherapy intervention for persons living with HIV-AIDS has yielded hopeful results (
10 ). Interpersonal psychotherapy treats depressive symptoms by focusing on grief, interpersonal disputes, role transitions, and interpersonal sensitivity (
11 ). Given the nature of stressors that confront many HIV-infected persons in rural areas, such as multiple bereavements, partner-relational conflicts, and discrimination (
2,
12,
13 ), therapeutic interventions that focus on interpersonal relations may be highly appropriate for this group. However, the only known randomized clinical trial that tested interpersonal therapy with HIV-infected persons was conducted with an urban sample more than a decade ago and used a face-to-face format (
10 ). It is unclear whether telephone-delivered, interpersonal therapy can reduce psychiatric distress among HIV-infected persons in rural areas.
Because AIDS treatment providers are often in need of interventions that are brief and can be administered immediately (for example, to a client in acute crisis), the intervention presented here utilized a six-session format. Many investigations have found that psychotherapy provides beneficial results in as few as five to eight sessions (
14,
15 ). To shorten yet maintain the efficacy of this intervention, Myrna Weissman, an originator of interpersonal therapy, recommended following the original interpersonal manual but reducing the number of sessions from 12 to six (Weissman M, personal communication, 2005).
The hypothesis tested in this research was that participants who received brief, telephone-delivered, interpersonal therapy would evidence statistically significant and clinically meaningful reductions in depressive symptoms, psychiatric symptoms, and loneliness from pre- to postintervention, compared with persons in the control group, who received no active intervention. Participants in both conditions continued to access medical and mental health care services commonly available to persons living with HIV-AIDS—for example, individual therapy and support groups.
Methods
Participants and procedures
Seventy-nine participants were recruited through AIDS service organizations in ten states: Indiana (N=20), Arizona (N=16), Ohio (N=14), Kentucky (N=11), Pennsylvania (N=8), Minnesota (N=4), Michigan (N=3), California (N=1), Nebraska (N=1), and New York (N=1). Recruitment packets containing information about the study, eligibility criteria, and toll-free contact information were mailed to 21 AIDS service organizations; the agencies then forwarded packets to potential participants.
All eligible participants satisfied the following inclusion criteria: 18 years of age or older, self-reported diagnosis of HIV-AIDS, voluntary provision of informed consent, and residence in a community with 50,000 residents or fewer (that is, the criteria used by the Centers for Disease Control and Prevention to designate communities as nonmetropolitan [
1 ]). Furthermore, all participants met diagnostic criteria for a depression-spectrum disorder, as measured by a telephone-administered version of the Mood Module of the Primary Care Evaluation of Mental Disorders (PRIME-MD) (
16 ). Specifically, participants met criteria for a major depressive episode (current or partial remission) or dysthymic disorder. Of the 96 individuals who contacted the research office, 12 did not meet criteria for having a depressive disorder.
General methodology and intervention conditions
Before the initiation of the project, the study's methodology was approved by the university's institutional review board. During eligibility screening interviews, informed consent procedures and benefits and risks associated with the study were discussed with participants. Eligible participants were mailed informed consent forms and preintervention surveys to be completed and returned within ten days. Five individuals did not return surveys. Upon receipt of preintervention assessments, 79 participants were randomly assigned to usual care or to a telephone-delivered, interpersonal therapy intervention plus usual care (hereafter referred to as teletherapy).
Usual care condition. Participants assigned to the usual-care condition (N=38) received no active therapeutic intervention. However, all participants had access to services not provided by the research project that was available through their AIDS service organization (for example, support groups) and other providers in the community (for example, individual therapy). No limitations were imposed on participants' use of psychosocial services available to them outside of the study's protocol. Although participants in the usual care group were given the opportunity to contact the research office and request brief, time-limited individual telephone therapy if in acute distress, none requested this service.
Interpersonal therapy intervention plus usual care. Participants assigned to the teletherapy condition (N=41) received six 50-minute sessions of telephone-delivered therapy. Similar to participants in the usual care group, those in the teletherapy group had access to services provided by their AIDS service organization and other providers in the community. At the start of the intervention, all participants in the teletherapy group were encouraged to identify a private location for sessions, schedule sessions at a time when few interruptions were anticipated, and refrain from the use of call waiting, except in possible emergency circumstances.
The first teletherapy session explored participants' psychiatric symptoms, discussed the nature of depression, reviewed current interpersonal relationships, and identified a therapeutic focus for later sessions. On the basis of the interpersonal therapy protocol (
11 ), each participant's primary interpersonal concern was framed around one of four focal areas: interpersonal role disputes (for example, conflict with a partner); role transition (for example, loss of employment); grief (for example, death of a loved one); or interpersonal deficits, which was eventually relabeled "interpersonal sensitivity" (for example, chronic difficulty forming and maintaining close relationships) (
17 ). Sessions 2 through 6 addressed the interpersonal conflict identified in the first session via exploration of participants' perspectives, communication patterns, expectations, and adaptive coping strategies. Each participant had the same therapist for all six sessions.
Twelve therapists (11 master's-level clinical psychology trainees and one doctoral-level clinical psychologist), all of whom had three or more years of experience conducting psychotherapy, implemented the intervention. Therapists completed a one-day training session to maximize comprehension of the intervention, review interpersonal theory, and discuss biopsychosocial issues related to working with HIV-seropositive individuals. The training also reviewed protocols to be enacted in the event of an emergency (for example, a participant's expression of suicidal intent), including information detailing local mental health organizations in participants' home states and national AIDS crisis hotlines.
Training was followed with ongoing weekly supervision with a licensed clinical psychologist and as-needed individual consultations to ensure fidelity to the intervention protocol. A standardized adaptation of the original interpersonal manual, revised to reflect the shortened number of sessions of the intervention, was used by all therapists to guide intervention delivery.
Assessment instruments
All study data were collected between February 2006 and March 2007. Before and immediately after participating in the intervention, participants were mailed the study's 12-page questionnaire, along with self-addressed, stamped envelopes to return documents. The questionnaire took approximately 45 minutes to complete. Participants were compensated $20 for completing the preintervention survey and $20 for completing the follow-up survey. No financial compensation was provided to participants for time spent in therapy. Study measures are listed below, all of which used a retrospective recall period of the past week. All psychometric characteristics were based on data collected in this study.
Beck Depression Inventory. The 21-item Beck Depression Inventory (BDI-II) measured cognitive, affective, and somatic symptoms of clinical depression (
18 ). Each item uses a 4-point response scale, yielding a total possible score between 0 and 63, with higher scores indicating greater depressive symptomatology (
α =.89).
Outcomes Questionnaire. The 45-item Outcomes Questionnaire (OQ) measured psychiatric distress across three dimensions: subjective discomfort, interpersonal relations, and social role performance (
19 ). Each item uses a 5-point response scale, ranging from 0, never, to 4, almost always. The OQ total score was also computed, with possible scores ranging from 0 to 180; higher scores indicated poorer overall psychiatric functioning (
α =.95, total scale).
Provision of Social Relations Scale. The 15-item Provision of Social Relations Scale (PSRS) assessed perceived social support from family members and friends (
20 ). Each item used a 5-point response scale, ranging from 1, very much like me, to 5, not at all like me. Higher scores indicate more support (
α =.88).
UCLA Loneliness Scale. A ten-item version of the UCLA Loneliness Scale assessed perceptions of loneliness (
21 ). Each item uses a 4-point response scale, ranging from 1, never, to 4, often. Higher scores indicate more loneliness (
α =.82).
Sociodemographic characteristics. Participants provided data on their gender, ethnicity, education, employment status, income, relationship status, duration of illness, health status, current living arrangements, mental health support services they were currently receiving (for example, individual therapy, AIDS-specific support groups, and 12-step programs), and pharmaceutical treatments they were receiving outside of the study's protocol (for example, antidepressant and anxiolytic medications).
Data analytic plan
Chi square tests of association and independent group t tests were first conducted to identify associations among demographic characteristics assessed at preintervention, intervention condition, and completion status (completed intervention or dropped out). The primary outcome analysis compared participants in the teletherapy group and those in the control group with repeated-measures analysis of variance (ANOVA) on scores from the BDI-II, the OQ, the PSRS, and the UCLA Loneliness Scale. Clinical significance was evaluated by using the Reliable Change Index (RCI) (
22 ), which was calculated as a difference in score (posttreatment score minus pretreatment score) divided by the standard error of measurement. Reliable change in scores greater than one standard deviation (1.96) suggested that a participant's pre- to postintervention change exceeded measurement error. Participants who showed reliable change and whose scores moved from a dysfunctional range to a more functional state were considered to have clinically meaningful change.
Results
Participant characteristics
Participants' mean±SD age was 44.4±8.6 years (minimum age of 25 years, and maximum age of 65 years). Sixty-six participants (84%) were male. Sixty-one were white (77%), eight were African American (non-Hispanic) (10%), seven were Latino (9%), two were African American (Hispanic) (3%), and one was Native American (1%). The average participant had completed 12.2±1.9 years of formal education. Social Security Disability Insurance was the primary income of 48 participants (61%), and 53 (67%) reported an annual income below $10,000. Fifty-two participants (66%) had been prescribed highly active antiretroviral therapy (HAART). The average participant had been living with an HIV infection for 11.0±5.6 years and lived an average of 91.3±31.3 miles from a city of 100,000 or more residents.
At preintervention, participants' mean BDI-II score was 27.4±11.0, with 68 (86%) reporting BDI-II scores higher than 13, the cutoff value recommended for identification of at least mild depression (
18 ). Sixty-four participants (81%) exceeded the OQ clinical cutoff (that is, OQ ≥63) (
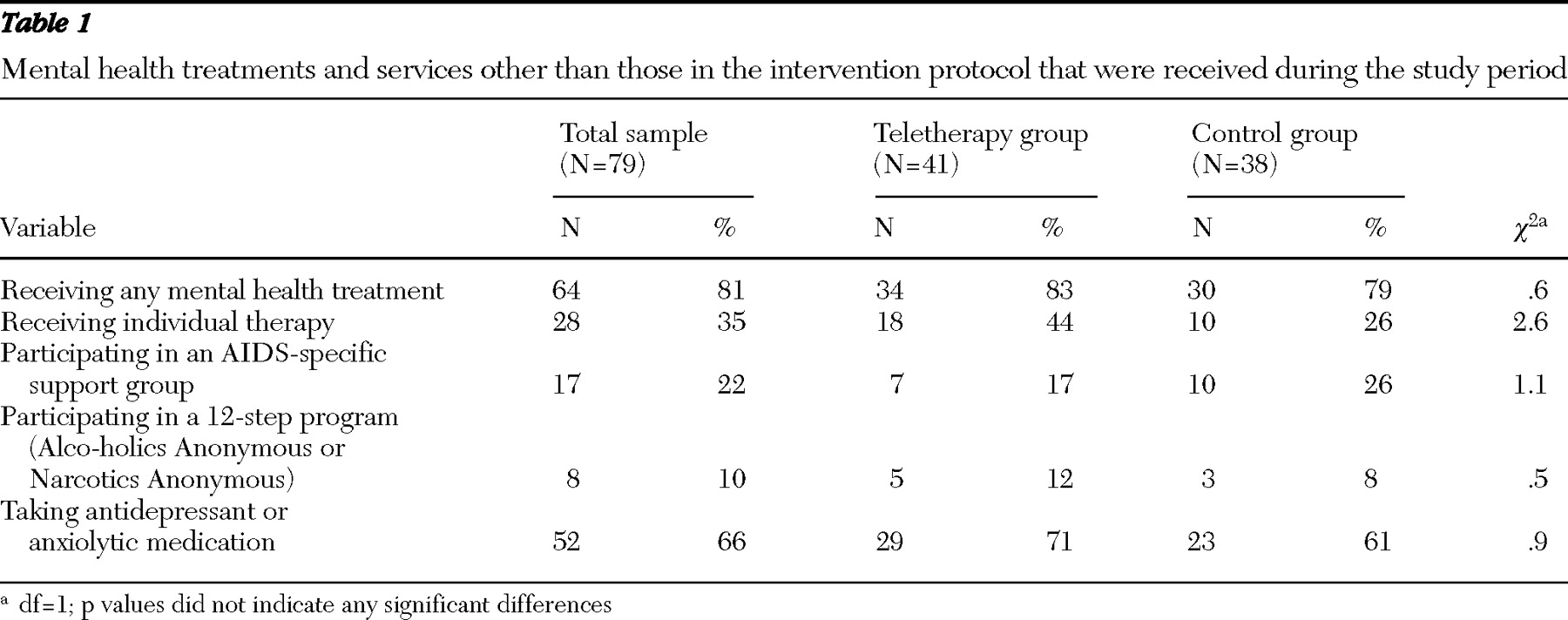
19 ). Most participants (N=64, or 81%) were receiving some form of mental health treatment during the study period outside of the study's protocol (
Table 1 ). Involvement in mental health treatment outside of the study's protocol (for example, attending support groups) was unrelated to study condition. Accordingly, utilization of outside services was comparable across condition at preintervention and not treated as a covariate in outcome analyses.
Chi square analyses found no relationships between intervention condition and gender, ethnicity, employment status, relationship status, or current involvement in mental health care services. A series of independent group t tests found no significant differences between intervention condition and age, education, number of years living with HIV, depressive symptoms, loneliness, or perceived social support at preintervention. However, participants in the teletherapy group had marginally higher OQ scores at preintervention (87.0±24.0) than those in the control group (78.2±22.0) (p=.09).
Attrition rates and completer versus noncompleter analyses
Thirteen participants (16%) were lost to attrition. Participants in the teletherapy group were marginally more likely to discontinue study involvement (N=10) than those in the control group (N=3), although this association was not significant. Some of those who discontinued study involvement could not be contacted as a result of relocation without a forwarding address (N=5) or loss of telephone service (N=3). Others discontinued participation as a result of lack of time (N=1), family conflicts (N=1), mortality (N=1), or repeated inability to commit to intervention participation (N=2). Independent-group t tests and chi square analyses found no significant associations between whether participants completed the study or dropped out and any demographic or psychosocial variables assessed at the preintervention. Participants with missing postintervention data (N=13) were retained for final outcome analyses by using a last-observation-carried-forward approach, a method commonly used in clinical trials to provide a conservative estimate of outcomes had participants remained in treatment but evidenced no change (
23 ).
Treatment outcomes
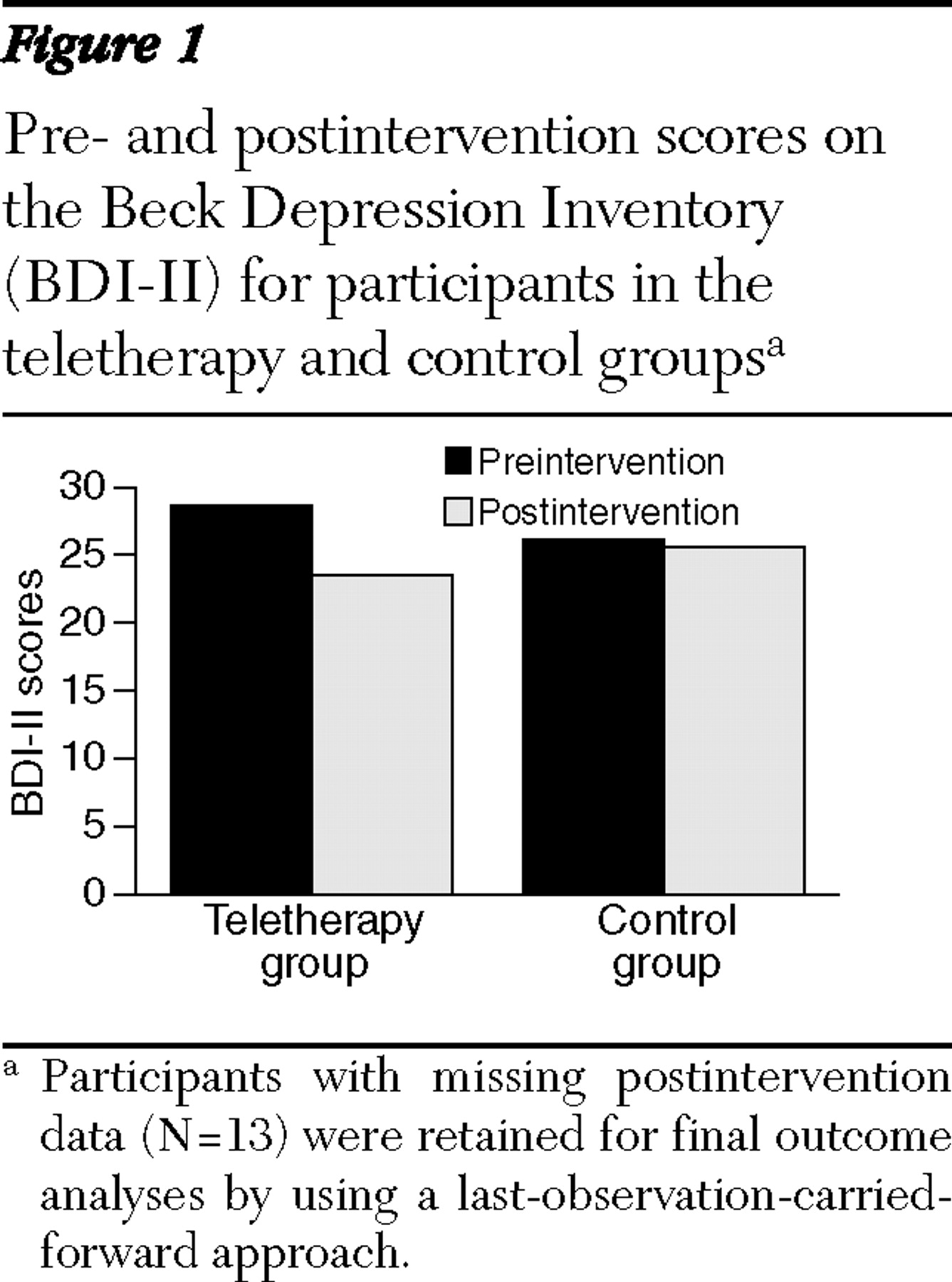
A series of 2 (teletherapy and control) × 2 (preintervention and postintervention) repeated-measures ANOVAs was conducted that used the study's four outcome measures. The ANOVA that used BDI-II scores found no main effect for condition, a significant main effect for time (F=8.9, df=1 and 77, p<.01), and a significant time × condition interaction (F=6.1, df=1 and 77, p<.05). The interaction, shown in
Figure 1, showed that participants in the teletherapy group reported significant reductions on the BDI-II scores from preintervention (28.7±11.2) to postintervention (23.5±12.5) (mean change score=5.2), compared with those in the control group (preintervention score=26.1±10.8 and postintervention score= 25.6±13.5, with a mean change score=.5) (partial eta-squared for interaction=.07). One-way ANOVA post hoc comparisons found that the two conditions did not differ significantly on BDI-II scores at pre- or postintervention.
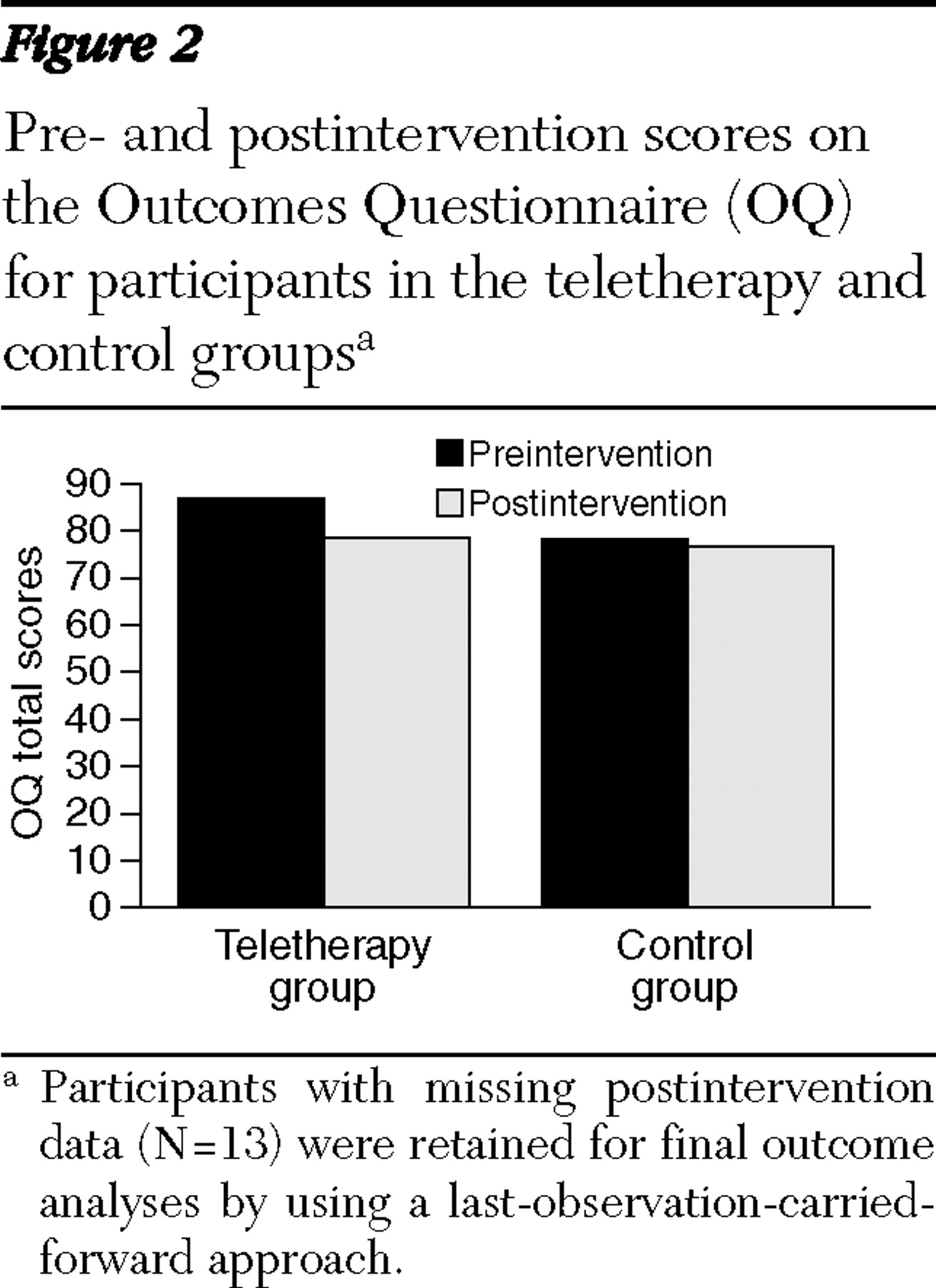
ANOVA conducted using total scores on the OQ found no main effect for condition, a significant main effect for time (F=9.5, df=1 and 77, p<.01), and a significant time × condition interaction (F=4.5, df=1 and 77, p<.05). The interaction, shown in
Figure 2, found that participants in the teletherapy group reported greater decreases in OQ scores from preintervention to postintervention (preintervention=87.0±24.0 and postintervention=78.5±31.3; mean change score=8.5) than did those in the control group (preintervention=78.2±22.0 and postintervention=76.7±26.6, with a mean change score=1.5) (partial eta-squared for interaction=.06). One-way ANOVA post hoc comparisons found that participants in the teletherapy group reported marginally higher OQ total scores at preintervention than did those in the control group (p=.09); the two groups did not differ significantly at postintervention. No hypothesized condition × time interactions were found for the UCLA Loneliness Scale or the PSRS.
Clinically meaningful change among study completers
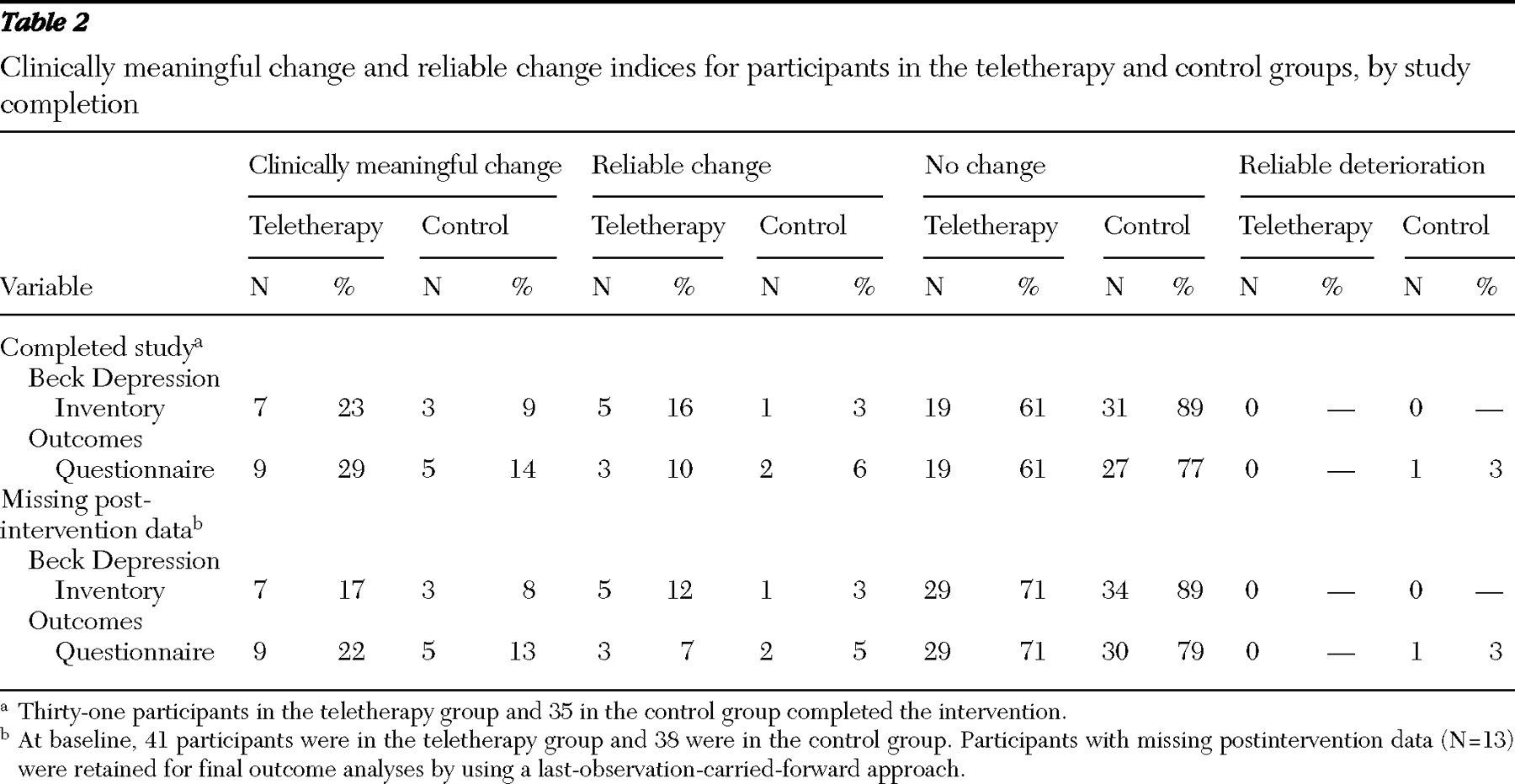
Clinically meaningful and reliable change on the BDI-II. Of the 31 participants who completed the interpersonal therapy intervention, seven (23%) showed a clinically meaningful change on the BDI-II. Specifically, these participants evidenced a reduction of ≥9 points on the BDI-II and had postintervention BDI-II scores of 13 or less (calculated from community samples by using the RCI [RCI =(X
post -X
pre )/S
diff ]) (
24 ). An additional five participants (16%) in the teletherapy group evidenced reliable change (that is, change of BDI-II score ≥9 points and a postintervention BDI-II score higher than 13). The remaining participants in the teletherapy group (N=19, or 61%) evidenced no reliable change. No participants in the teletherapy group evidenced an RCI value indicating reliable deterioration (that is, RCI<–1.96 in this sample). Among participants in the control group, only three (9%) evidenced clinically meaningful change on the BDI-II over the six-week study period, and only one showed reliable change.
Clinically meaningful and reliable change on the OQ. Among those who completed the teletherapy sessions, nine (29%) evidenced a reduction on the OQ of ≥14 points and had final OQ scores of ≤63 (defined as standards for determining clinically meaningful change in outpatient and community clinics) (
25 ). Another three participants (10%) in the teletherapy group evidenced reliable change (that is, a decrease of ≥9 points in OQ scores over the study period and postintervention scores ≥63). The remaining 19 participants (61%) in the teletherapy group evidenced no reliable change. In the control group, only five participants (14%) showed clinically meaningful change on the OQ; two participants (6%) evidenced reliable change. One participant in the control group had an RCI value indicating reliable deterioration (
Table 2 ).
Discussion
Results from this pilot trial suggest that brief telephone-delivered, interpersonal therapy constitutes a potentially effective approach to reducing psychiatric distress among HIV-infected persons in rural areas. Participants in the teletherapy group evidenced significant reductions in depressive and psychiatric symptoms (unlike those in a time-matched control group). Moreover, nearly 30% of participants in the teletherapy group who completed the intervention reported clinically meaningful reductions in OQ total scores. This rate is comparable to, albeit somewhat lower than, rates of clinically meaningful change reported in the psychotherapy outcome literature. Between 40% and 60% of participants in clinical efficacy trials evidence clinically meaningful improvements after 12 to 14 sessions, 10% show clinical deterioration, and the remainder show minimal or no change (
26 ). Note that these estimates of clinically meaningful change are based on treatments of 12 or more sessions (the number typically administered in efficacy trials) and not the three to five sessions administered in routine practice; effectiveness rates in the latter setting are typically 10% (
27 ).
As such, rates of clinically meaningful change observed in this study were less than those found in randomized controlled clinical trials but greater than those seen in routine practice settings. Although it is important to note that approximately 23% of participants in the teletherapy group showed a clinically meaningful change on the BDI-II (compared with only 8% of those in the control group), the teletherapy group's mean BDI-II score at postintervention remained in the "moderate" level of depressive symptomatology, and participants in the teletherapy and control groups did not differ significantly at postintervention on BDI-II scores. Although the teletherapy intervention may promote clinically meaningful change among some participants, the lack of even greater reductions in BDI-II scores in this study calls into question the utility of this briefer version of the original interpersonal therapy intervention. Perhaps increasing the number of intervention sessions would augment the intervention's efficacy.
Several study limitations should be noted, including the relatively small sample (N=79) and the self-selected nature of the sample that provided power sufficient only to detect large effect sizes (
28 ). All data were self-report in nature and susceptible to social desirability, demand characteristics, and recall bias. No physiologic or chart-review data were collected, and no formal documentation of participants' HIV-seropositive status was obtained. An additional limitation is the study's eligibility screening protocol and assessment of participants' depressive symptoms at preintervention. Specifically, 14% of participants diagnosed as having a depressive disorder during eligibility screenings reported preintervention BDI values of 13 or less. This disparity could be the result of the different assessment methodologies inherent to the two procedures (for example, a telephone-based interview used to make a diagnosis versus a self-report measure of depressive symptoms). Conversely, this disparity could be related to participants' experiencing reductions in depressive symptoms after learning that they had enrolled into an intervention study that might connect them with mental health support services at no cost (
29 ).
The study assessed only short-term effects associated with the intervention; no long-term follow-up determined whether the intervention gains reported by participants in the teletherapy group were maintained over time. An additional limitation is that most participants (81%) were receiving concurrent mental health treatment outside of the intervention, including psychotropic medications, individual therapy, and support groups. Although no significant group differences in the use of alternate mental health treatments were found at preintervention, slightly greater proportions of participants in the teletherapy group appeared to be accessing mental health services outside of the study, compared with those in the control group. Some gains reported by participants in the teletherapy group may have been the result of these outside services and not the intervention. All intervention therapists were trained and supervised according to the original interpersonal therapy protocol (
11 ); however, none was formally certified in interpersonal therapy; the use of nonexpert therapists may have had an impact on study findings. Lastly, on the basis of national AIDS surveillance data, this study undersampled rural African Americans, persons infected through intravenous drug use, and persons from southern states (
30,
31 ).
Conclusions
This investigation found that brief telephone-delivered, interpersonal therapy showed potential to reduce psychiatric distress among HIV-infected persons in rural areas. These findings are consistent with research showing that telephone-delivered, interpersonal counseling—a shortened variant of interpersonal therapy developed for psychologically distressed but not clinically depressed persons—reduced depressive symptoms among women following miscarriage (
32 ). However, the preliminary nature of this pilot study and the relatively small effect sizes associated with the intervention suggest that additional examination of this intervention is needed before it can be disseminated widely to persons in rural areas living with HIV-AIDS.
Acknowledgments and disclosures
This study was funded by the Ohio University Health Psychology Group.
The authors report no competing interests.