Disengagement from mental health services continues to be a pressing problem for people with serious mental illnesses (
1,
2 ). Consumers who are homeless and have serious mental illnesses, and substance use disorders in particular, struggle to maintain stability in the community, leading to high rates of hospitalization, incarceration, and use of crisis services (
3 ). Assertive community treatment is an intensive intervention designed specifically to meet the needs of consumers whom the system has not successfully engaged. Consisting of a multidisciplinary team, which shares a small caseload of consumers, assertive community treatment provides crisis intervention, treatment, and rehabilitation services in the community (
4 ). More recently, assertive community treatment has been adopted as a service delivery mode for the Housing First model, which incorporates a right-to-housing philosophy and harm reduction approach. Consumers are offered immediate access to independent living that is not contingent on treatment adherence or maintaining sobriety. There has been research on the effectiveness of assertive community treatment and the Housing First model. However, the social interaction involved in engaging and maintaining consumers in services remains an understudied aspect that may have considerable impact on consumer outcomes for this highly vulnerable population (
4,
5,
6,
7,
8,
9 ).
Engaging consumers with assertive outreach has been described as "the velvet bulldozer" (
10 ), capturing the way case managers combine pressure and support in their service approach. When faced with a consumer who is reluctant to engage in services, case managers rarely have a set procedure to follow; instead, they rely on their skills, knowledge of the consumer, and the context in which they are making clinical decisions. Pressure, as opposed to support, takes the form of coercive strategies, beginning with persuasion, leverage, and inducements and escalating to threats and enforcement of formal mechanisms, such as involuntary commitment (
11,
12,
13 ). Neale and Rosenheck (
13 ) examined case managers' use of pressure and found that they tend to use less coercive measures, such as persuasion and leverage, rather than threats or formal mechanisms.
The perspective of consumers is key to understanding the impact of case manager pressure, because coercion is determined largely by how consumers interpret provider behavior (
14,
15,
16 ). Findings show that consumers vary in their subjective responses to coercive pressure within treatment settings (
9,
17,
18,
19 ). Differences in perceived coercion may be attributable to the existing relationship between provider and consumer. The degree to which the consumer feels an emotional bond with the case manager may influence the degree to which he or she feels coerced by the case manager (
20,
21 ). The concern is that high levels of perceived coercion will drive consumers, whose connection to the mental health system is tenuous at best, out of services and deter them from reengaging in services in the future (
22 ).
This exploratory study examined the extent to which social interaction between consumers and their case managers is related to the treatment experience from the perspective of consumers. The study addressed the following questions: What factors are associated with perceived coercion by the consumer? To what extent are perceived coercion, the consumer-provider relationship, and consumer and service contact characteristics associated with consumers' evaluation of a service contact? Understanding how perceived coercion and consumer-provider relationships shape consumers' responses to services is an important step toward improving service effectiveness, particularly with consumers whom the system has not successfully engaged.
Methods
The study setting was a program that provides services to people who have experienced long-term street homelessness and have serious mental illnesses and co-occurring substance abuse or dependence. The program combined the Housing First approach with assertive community treatment. The team consisted of a social worker as the team leader, a community psychiatrist, a psychiatric nurse, five case managers, and a peer support specialist. The caseload of 65 consumers was shared, and all team members had case management responsibilities. The team provided approximately 6,000 face-to-face service contacts with consumers each year. Approval for the study was obtained from city and university institutional review boards. The study was conducted between February 2006 and June 2006.
The unit of analysis for the study was an individual service contact. A service contact was operationally defined as a face-to-face encounter between the consumer and a case manager that lasted between 15 minutes and three hours. Consumers and case managers could be included in multiple service contacts provided that the service contact took place between a unique consumer-provider dyad.
Random days were selected each week for a researcher to attend the program for data collection. On those days a random case manager was accompanied in the field or in the office to sequentially sample service contacts. All service contacts for that provider on that day were eligible for inclusion in the study. At the conclusion of the service contact, the case manager briefly explained the research study, and if the consumer was willing to participate, the consent process and interview with the consumer were conducted by the researcher in a private space without the case manager present. A total of 80 persons were selected for the study from the service contacts. Of these, ten consumers declined to participate.
Measures
The researcher administered a 20-minute structured interview with the consumer to assess sociodemographic characteristics, consumer report of the consumer-provider relationship, consumer report of case manager utilization of coercive strategies, perceived coercion, and consumer evaluation of the service contact. Agency clinical records were reviewed for diagnostic and housing information. The primary clinical diagnosis was based on the most recent diagnosis in the record. Housing status was based on whether the consumer had housing (in an apartment) or not (in a shelter or on the street) at the time of the interview. Service contact location and time of service contact were recorded by the researcher.
Consumer characteristics and service contact characteristics were independent variables. They included gender, race, age, education, primary psychiatric diagnosis, representative payee status, and housing status. Service contact characteristics were location and length of time.
The consumer's assessment of the consumer-provider relationship and the case manager's use of coercive strategies were included as key independent variables in all analyses. The consumer-provider relationship was measured by the Working Alliance Inventory, Short Form (WAI-S) (
23 ). The 12-item measure referred to the consumer's bond with his or her case manager and the pair's collaboration on tasks and goals. Respondents rated the statements on a 4-point Likert scale (from strongly disagree to strongly agree; higher scores indicated a more positive relationship), and scores were summed. The measure has been found to have good reliability and to be highly correlated with the original 36-item Working Alliance Inventory (
24,
25 ). Coercive strategies were measured by four of the five subscales from the Therapeutic Limit Setting measure (TLS) (
13 ). The subscales made up a 16-item measure for reflecting a continuum of coercive strategies by case managers, including verbal guidance, contingent withholding, involuntary hospitalization, and invoking external authorities. Responses were no or yes, and positive responses were summed; higher scores indicated stronger use of coercion. The TLS subscales have been shown to be internally consistent and predictive of the treatment process and alliance (
13 ).
Perceived coercion and service contact evaluation were included in the analyses as dependent variables. Perceived coercion was measured by two subscales from the Modified Admission Experience Survey (
26 ), which measures the extent to which consumers feel they are in control during outpatient services. The items were adapted to reflect a service contact between the consumer and case manager. The two subscales made up a nine-item measure. Responses were yes or no, and positive responses were summed. Service contact evaluation was measured by the tasks subscale of the Session Impacts Scale (
26 ), which measures the extent to which consumers feel they are in control during outpatient services. The items were adapted to reflect a service contact between the consumer and case manager. The two subscales made up a nine-item measure. Responses were yes or no, and positive responses were summed. Service contact evaluation was measured by the tasks subscale of the Session Impacts Scale (SIS) combined with two statements about progress made toward consumer goals as a result of the service contact (
27 ). The tasks subscale addresses having insights about self and others and solving problems. Respondents rated five SIS statements on a 4-point Likert scale (from strongly disagree to strongly agree), and scores were summed. Good validity and reliability have been demonstrated for the tasks subscale (
27,
28 ). Consumers chose one of ten areas, including social support, housing situation, mental health symptoms, and drug or alcohol use, as the primary purpose of the service contact. Respondents rated on a 4-point scale ranging from strongly disagree to strongly agree whether their situation and their ability to handle it in the designated area improved as a result of the service contact. The scores were summed. The tasks subscale and the evaluation statements were significantly correlated with each other (.35), and the measure had an overall Cronbach's alpha of .80.
Analyses
Nonresponse weights were created to adjust for differences between the universe of service contacts during the data collection period and the study sample on key variables. During the five-month data collection period, the team conducted 2,386 face-to-face service contacts. Agency service utilization reports provided data on consumer race, consumer gender, service contact location, and service contact length. When the study sample was compared with the universe of service contacts, the only significant difference in variables was found with respect to race, with the study sample overrepresenting African-American clients (87% versus 79%). The nonresponse weights were calculated with propensity score algorithms (
29 ). Weights were included in all analyses.
Perceived coercion and service contact evaluation were examined via bivariate analyses to determine whether means differed statistically, by t tests, between levels of categorical independent variables or whether the correlations were statistically different from zero for continuous independent variables. Multivariate analyses examined predictors of the service contact evaluation, including the two key independent variables and those that were statistically significant in the bivariate analyses. Univariate, bivariate, and multivariate regression analyses (standardized and unstandardized) were conducted with the SAS Surveyfreq, Surveymeans, and Surveyreg processes (
30 ). Generalized estimating equations were used to adjust the standard errors of our estimates in order to accommodate the clustering of service contacts nested within the data about the nine case managers (
31 ). Cohen's f
2 was calculated to assess the magnitude of study effects (
32 ). Specifically, f
2 is a ratio of the explained variance of a variable of interest as obtained from the regression output to the error variance in the multivariate model, with small, medium, and large effects corresponding to an f
2 of .02, .15, and .35, respectively (
32 ).
Results
Sample characteristics
The sample comprised 70 service contacts between unique case manager and consumer dyads. The dyads included nine case managers and 42 consumers. Each case manager participated in an average of 10.9±5.1 service contacts, and each consumer participated in an average of 2.14±1.1 service contacts.
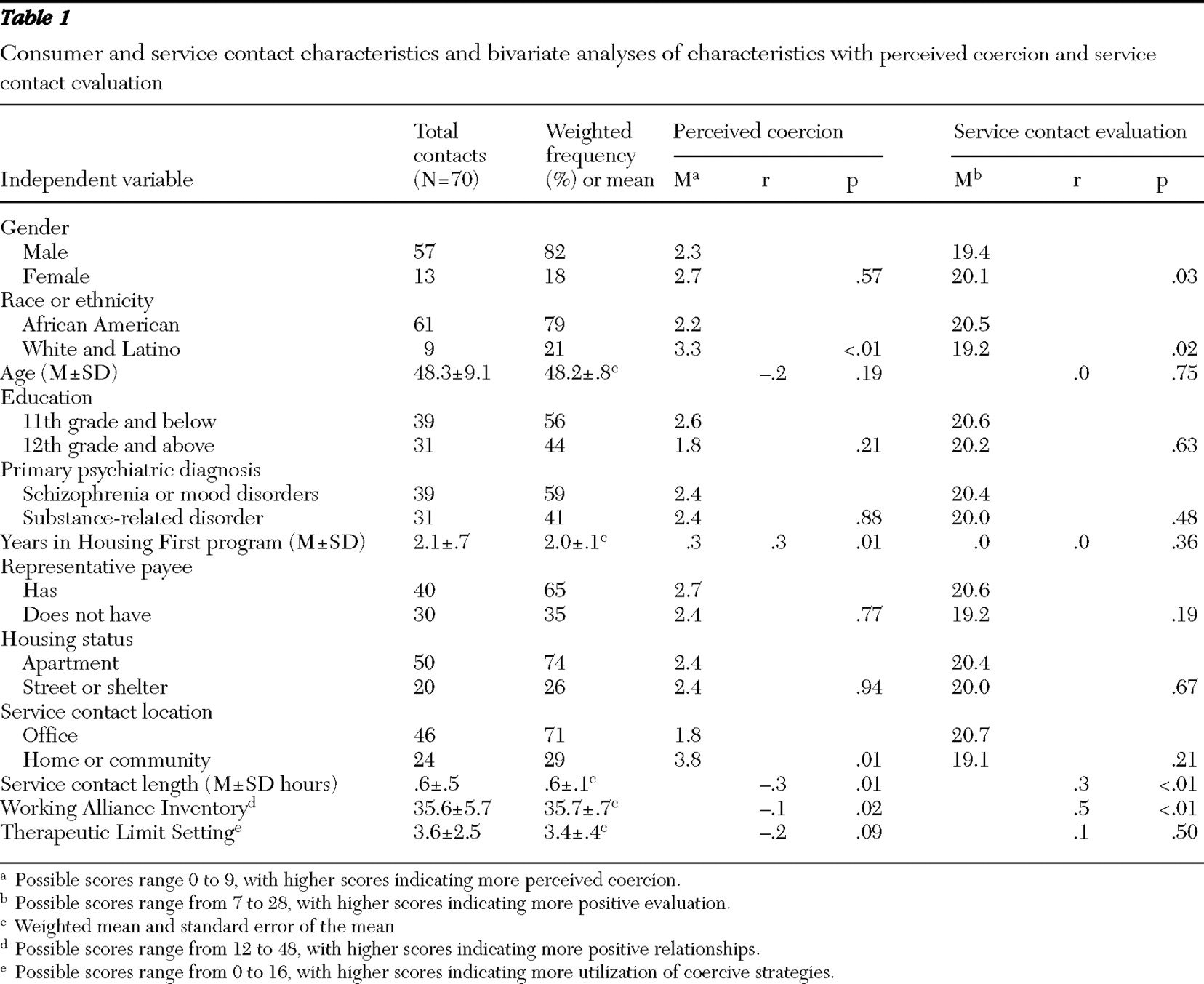
Table 1 presents consumer and service contact characteristics. Overall the sample did not differ greatly from the universe of service contacts, which reflects the demographic characteristics of people experiencing long-term homelessness in Philadelphia, with most being African American and male.
The sample mean score for the TLS was 3.6±2.5 out of a possible 16 points, demonstrating that, from the perspective of consumers, case managers mainly used verbal limit-setting strategies and almost never used high-end coercive strategies. The sample mean score for WAI-S was 35.6±5.7 out of 48 possible points, indicating that a majority of consumers reported positive relationships with case managers.
According to the bivariate analysis (
Table 1 ), perceived coercion was associated with race, years in the program, service contact location, service contact length, and WAI-S score. Service contact evaluation was associated with gender, race, service contact length, and WAI-S score. TLS score was not associated with either of the dependent variables.
Perceived coercion
The regression analysis (
Table 2 ) with perceived coercion as the dependent variable indicated a negative relationship between consumer-provider relationship and perceived coercion (b=-.10, p<.05). However, the use of coercive strategies by case managers, as reported by the consumer, was not associated with perceived coercion. The negative association between consumer-provider relationships and perceived coercion was small (f
2 =.08). Race was associated with perceived coercion, with white or Latino consumers (b=1.20, p<.05) experiencing higher levels of perceived coercion than African-American consumers; the effect size was small (f
2 =.1). There was a strong positive relationship between the time consumers were in the program and the extent to which they felt coerced (b=1.18, p<.005). In terms of service contact characteristics, there was a negative relationship between perceived coercion and service contact length (b=-1.77, p<.05). The effect of perceived coercion on amount of time in the program was medium (f
2 =.17) and on length of service contact was small (f
2 =.14). A comparison of the standardized coefficients showed that years in the program and length of service contacts were associated with greater change in perceived coercion than race or consumer-provider relationships.
In the regression analysis with service contact evaluation as the dependent variable, perceived coercion was the only significant variable. Coercion perceived by the consumer was negatively associated with service contact evaluation (b=-.69, p<.05), representing a medium-to-large effect size (f 2 =.34). Relationships between the other variables and service contact evaluation, including consumer-provider relationship, which had been significant in the bivariate analyses, proved not to be explanatory in the multivariate models.
Discussion
Overall the study indicated that consumers perceived some coercion in encounters with case managers. When coercion was perceived, it had a significant association with how consumers evaluated services. In terms of consumer perception of case manager behavior, case managers in the study used almost exclusively low-end coercive strategies, and no relationship was found between their use of these strategies and perceived coercion.
The study findings concur with those of Monahan and colleagues (
14 ), who found that low-end coercive strategies, such as persuasion, were not related to feelings of coercion by the consumer. The lack of relationship between utilization of strategies and perceived coercion may also indicate that provider behavior is being interpreted differently, depending on the existing relationship between the case manager and consumer. As a result, the bond between consumer and case manager is related to the consumer's perception of coercion, whatever the case manager's behavior. Moreover, the study found a modest negative relationship between consumer-provider relationship and perceived coercion.
The study demonstrated that consumers experience feelings of coercion during their social interactions with case managers. However, sources of coercion appeared to be more diffuse than case manager behavior, in that consumers' perception of coercion did not correspond to their report of use of coercive strategies by case managers. This finding suggests that case managers must not only monitor their own actions but also be aware of the consumer's subjective understanding of the service contact. Consumers are often mindful of past experiences with other providers in their present clinical relationships, which can be a source of perceived coercion (
33 ). Previous disempowering experiences may contribute to their current feelings of coercion and learned helplessness.
Perceived coercion had a negative relationship with the evaluation of the service contact by the consumer. The question arises whether short-term negative effects from one social interaction could translate into longer-term negative outcomes. For a population with a high level of distrust for and precarious engagement with mental health services, there seems a greater likelihood of driving individuals out of services if they feel coerced. Also, negative social exchanges have been found to be more predictive of consumer outcomes than positive social exchanges (
34 ). The study provides empirical support for one of the central tenets of the recovery movement—that there is no role for coercion in mental health services, either short or long term (
35 ).
Cultural factors played a role in the consumer response to services, with African-American consumers experiencing lower levels of perceived coercion than whites and Latinos. White and Latino consumers constituted a minority in the program and may have felt they were treated differently from others. More positive alliances have been found among case managers and African-American consumers than white consumers, suggesting that persons in racial-ethnic minority groups may respond more favorably to assertive outreach activities as opposed to more traditional services (
36 ).
The service-related factors associated with perceived coercion were the length of service contact and the time the consumer had been in the program. Consumers experienced higher levels of coercion during shorter service contacts. Many of the service contacts conducted in the study were only 15 minutes long (32% of contacts), which is the minimum time allowed for Medicaid billing purposes. These contacts may have felt more "business like" for the consumer, because there was little time for social niceties, and they may have felt more cajoled by the program requirements. It is noteworthy that consumers who had been in the program for a longer period also experienced higher levels of coercion. This finding may reflect the initial engagement phases of offering consumers apartments with few strings attached—a key component of the Housing First model—and the later service phases that focus more on mental health treatment and reduction of substance use. But, again, this may have been more a perception by consumers, rather than their case managers' behavior or the program approach, which stresses consumer choice.
There are several notable limitations to the study. The study design had to accommodate the logistical and feasibility demands of case managers. This meant they functioned as gatekeepers for study participants, which introduces the possibility that case managers selected service contacts on the basis of social desirability. However, few differences between the study sample and the universe of service contacts with respect to consumer and service contact characteristics were found. The sample was relatively small because of resource constraints. However, even with a small sample the study detected medium effects. The study design was cross-sectional, and key measures were drawn only from consumer self-report in a single interview. Therefore, measures may be subject to reporting bias, and no inferences can be made about causality. Future research could address these limitations by conducting a longitudinal study to examine whether baseline measures of perceived coercion relate to follow-up ratings of alliance by consumers and providers and long-term clinical outcomes such as retention in services.
Conclusions
The study clearly indicated that process factors play an important role in how consumers respond to services. Further research is needed to identify mechanisms of support that provide case managers with alternatives to use of pressure. Genuine collaboration fostered by shared decision making and structuring consumer-provider communication are examples of strategies that empower consumers and improve satisfaction with services (
37,
38,
39 ). The study also showed that case manager decisions about the length of time they meet with consumers is related to the quality of service. Therefore, providing case managers with the clinical skills and the time to build trusting relationships is vital to promoting engagement and recovery-oriented services.
Acknowledgments and disclosures
This research was supported by grant F31-MH072558 from the National Institute of Mental Health.
The authors report no competing interests.