One of the challenges facing psychiatric health care systems is the inevitable variations in decision making that become evident when clinicians' performance is systematically measured. With each passing year, new studies emerge supporting empirically validated treatment interventions and, in some cases, delineating algorithms or protocols designed to guide treatment decision making in a stepwise fashion. Although each year new studies validate such interventions, their findings have not ended controversy in many areas of psychiatric intervention and best practice. Many of these disagreements have yet to be directly addressed by empirical research.
The mental health field continues to develop such interventions and protocols, and it is important to identify areas in which unhelpful variations in care can be remediated. In this column we describe a project undertaken at Western Psychiatric Institute and Clinic that focused on use of low-dose antipsychotics to address patient agitation and sleep difficulties. The literature does not support this practice. Moreover, the practice has led to substantial increases in treatment costs and the potential for increased medication-related side effects. Our goal was to increase awareness of these practices, develop a measurement system to support discussion about alternatives, and ultimately, to change prescribing practices. In this project we focused specifically on quetiapine, given observations at our institution that it was frequently prescribed at low doses for sleep and agitation, despite a lack of evidence for such use, the potential for significant adverse sequelae, and considerable cost.
This project was undertaken with the belief that changes in prescribing practices are best implemented through a combination of education about best practices and empirically validated methods, timely feedback about individual prescribing practices, and respectful peer discussion about prescribing decisions and superior alternatives. Our intent was to combine all three intervention methods and track prescribing practices at a large academic inpatient psychiatric facility.
The medical literature supports the use of continuing education for practitioners via in-person lectures, case conferences, and even the use of videos or simulations to bring clinicians' practices more in line with current guidelines (
1,
2,
3 ). Although such education results in some practice changes that are retained more than a year later, the gains are nevertheless modest (
4 ). In a study of 94 practicing physicians, less than one-third changed their practices in accordance with recommendations, even when they received individualized feedback from a committee of pharmacologists (
5 ).
Successful strategies for changing physicians' prescribing practices typically involve a variety of techniques (
6 ). Active participation in the learning process and definition of specific problems to be addressed are vitally important. Reinforcement of concepts, along with frequent individual feedback to physicians about their behavior, also facilitates change (
7 ).
The literature provides little information about attempts to change prescribing practices in mental health settings. A study of more than 40 Veterans Affairs hospitals assessed the role of various forms of education in modifying prescription of antipsychotics and anti-Parkinsonian medications in conformity with then-current prescribing recommendations (
8 ). Although the interventions appeared to result in a clinically meaningful alteration in prescribing practice, none of the results were statistically significant.
Another intervention to change prescribing practices involved identification of "questionable practice" prescription patterns, such as the prescription of three or more antipsychotics, and subsequent mailings and other initiatives to educate prescribers (
9 ). Our intervention was similar in that it used an initial educational process and subsequent peer discussions in groups of prescribers to address prescribing practices. Thus the educational process involved significant peer interaction and active discussion of appropriate practices.
Physician-designed intervention
Western Psychiatric Institute and Clinic is a large inpatient psychiatric hospital in Pittsburgh with 286 beds and approximately 40 inpatient psychiatrists. To assess physicians' adherence to evidence-based treatment guidelines and our ability to change prescribing practices, we monitored the prescription of quetiapine by inpatient psychiatrists for 18 months.
Before monitoring began, discussion groups with physician peer groups were held within service lines. The main objective of this physician-designed intervention was to stimulate discussion in order to improve practitioners' knowledge and the quality of care. The first part of the intervention was an introductory discussion of the project for groups of two to four physicians, which was led by the medical director of the physicians' service line. The second part involved electronic dissemination to physicians of several journal articles on the use of quetiapine (available from the authors on request). In the third part of the intervention, the medical director of the service line contacted the prescriber of each new prescription that met criteria for low-dose prescription of quetiapine. No manipulation of treatment was involved; that is, no mandatory replacements were ordered. Instead, a discussion about the rationale for the prescription occurred.
The therapeutic dosage of quetiapine for the treatment of psychotic and bipolar disorders typically ranges from 400 to 800 mg per day. Approved indications support dosages of 200 mg or less only during initial titration or for elderly patients. Therefore, new inpatient prescriptions of quetiapine for 200 mg or less per day were flagged by the monitoring system. After the prescriptions were flagged, relevant information, including dosage, patient demographic characteristics, and the name of the prescribing physician, was obtained by the hospital pharmacy on a daily basis. The information was entered into the study database, and electronic summary reports that contained information on the dosage and the name of the prescribing physician were e-mailed to both the medical director and chief of service for each of the hospital's six service lines as well as to the prescribing physician. The medical director was subsequently responsible for contacting the prescribing physician to determine the indication for the new prescription. The indication and justification for the low dose were identified by the prescribing physician, and this information was entered in the database.
To better assess long-term impact on behavior, we decided to discontinue peer discussions and data feedback to physicians from the system and from the medical director approximately four months after the project began, but we continued to monitor prescription and use of low-dose quetiapine for 18 months after the intervention was implemented.
Evaluation of the intervention
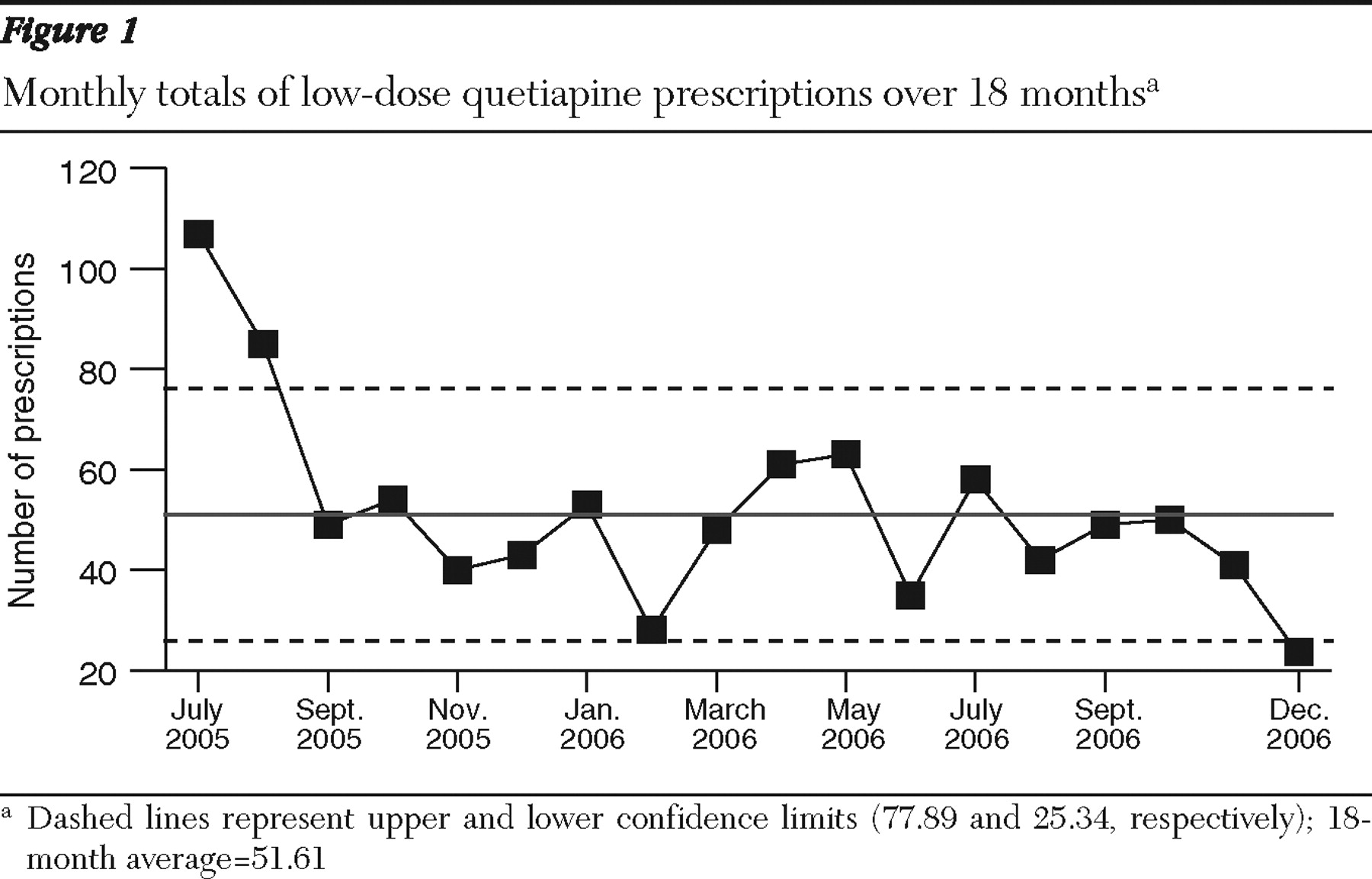
To determine the effectiveness of the intervention, each month for 18 months we compared the frequency of flagged prescriptions for low-dose quetiapine to the frequency at baseline—that is, in July 2005 before the intervention began. Low-dose quetiapine prescriptions for elderly patients (where a lower dose was indicated) or for those in the midst of an upward titration were not included in the monthly totals. In July 2005 approximately 50 attending physicians at the hospital wrote 107 new prescriptions of 200 mg or less of quetiapine. In December 2006 the same number of attending physicians wrote 23 such prescriptions (
Figure 1 ). Before the intervention, the cost for all inpatient quetiapine prescriptions was $15,170 per month. A gradual decline was observed over the course of the intervention. In December 2006 the cost was $7,028 per month.
We also sought to determine whether prescription of several medications increased as a result of the decline in quetiapine use, including chlorpromazine, clonazepam, diphenhydramine, haloperidol, hydroxyzine, lorazepam, temazepam, trazodone, and zaleplon. Although use of these medications was not examined in the same systematic manner as quetiapine, a brief analysis of the cost of the possible substitute medications over the 18-month period did not show any increase.
Lessons learned
We learned several lessons from the quetiapine project. First, perceived problems with prescribing practices must be validated empirically. A look at the prescribing practices for quetiapine at our institution suggested a broader utilization pattern than is supported by literature on the use of second-generation antipsychotics. Thus the need for an intervention was evident. Second, establishing a daily, real-time feedback loop in regard to prescribing practices that used a mix of electronic and handwritten data collection systems was quite complex, which highlights the importance of fully integrated electronic medical records systems. It was necessary to piece together a hand-based flagging system and a workflow between pharmacy staff and data collection staff and then convert this information to an electronic format for easy reading and dissemination to attending physicians, medical directors, and service chiefs.
Before implementing data tracking and feedback, we distributed journal articles on the use of quetiapine and held service-line discussions with medical leadership and attending physicians. These discussions promoted collegial interaction and learning. Physicians were able to hear about and actively discuss the prescribing practices of their colleagues. The discussions served as a prelude to the intervention and helped many physicians assess and modify their own prescribing practices. Thus we avoided presenting the intervention as a top-down or heavy-handed approach to altering practice patterns.
Physicians' responses to the intervention were generally positive. We sought feedback from prescribers on the process and found that many were appreciative of the opportunity to see how their peers practice medicine and to have discussions in a nonjudgmental, peer-protected environment. Further, several took this opportunity to modify their practices. One physician noted that he realized the need to be more transparent in his documentation when he modified patients' therapy. We estimate that 5%–10% of the prescribers who participated viewed the process negatively. These physicians usually cited reasons related to having their practices seemingly questioned.
Changes in prescriptions were not mandated, and low-dose quetiapine could be continued by the prescriber even after a discussion with the medical director. Therefore, we did not collect data on the specific cases in which the medication was continued at a low dose or the indications for continuation. As noted above, low-dose quetiapine prescriptions for elderly patients or for those in the midst of an upward titration were not counted. However, because prescribers could continue the medication at a low dose, no specific "allowable" categories of low-dose quetiapine were defined. In addition, we did not collect data on whether the intervention resulted in a change in patients' clinical status or increased costs in other areas, such as increased utilization of other services or increased hospital days after the prescription change occurred.
A number of individuals were concerned that we would see a rebound effect once active feedback to physicians ceased at around four months and that the practice would slowly increase. As noted, we continued to monitor prescribing practices and use of quetiapine for 18 months after the active phase of the intervention. Thus, for a year after peer discussions and data feedback ended, use of low-dose quetiapine remained at low levels, and there did not appear to be any rebound effect or resumption of the targeted practice.
Conclusions
The intervention process demonstrated that it is possible to affect the prescribing behavior of a substantial number of practitioners in an inpatient setting at a large academic teaching hospital through a process of education, feedback, and peer discussion. The decrease in new starts of low-dose quetiapine resulted in a reduction in the exposure of patients to medications with potentially serious side effects and decreased the likelihood of drug interactions among patients taking other antipsychotics. In addition, the reduction in use resulted in significant cost savings.
This project provided insight into both the processes and the information system features that are necessary to provide a real-time intervention. We believe that the lessons learned will be transferable to other projects that target prescribing practices at our institution and to similar projects at other institutions.
Acknowledgments and disclosures
The authors thank Charles F. Reynolds III, M.D., for his thoughtful review of the manuscript; Karen L. Fielding, Pharm.D., and Kristen L. Sakely, R.Ph., for assistance with data collection; and Kalyani Gopalan, M.S., M.H.A., and David White, M.H.A., for assistance with data analysis and presentation.
Dr. Fabian has received a speaker's honorarium from Bristol-Myers Squibb and investigator-initiative grant funding from GlaxoSmithKline. Dr. Nash is on the speakers bureaus of Eli Lilly and Company and Novartis. Dr. Haskett is on the speakers bureaus of Eli Lilly and Wyeth. The other authors report no competing interests.