Physicians, other health care professionals, and trainees in psychiatric units often confront the question of whether to seek criminal prosecution of patients with psychiatric disorders who assault staff members. Psychiatrists (
1,
2,
3,
4 ), psychiatrists in training (
5,
6 ), nurses (
3,
4,
7,
8 ), and patients (
3,
4,
9 ) are at risk of patient-initiated threats of violence or assaults. In particular, assaults or threats of violence by patients against psychiatrists in training are the most stressful adversity encountered during training (
10 ), are more commonly experienced by psychiatry trainees than by trainees in other specialties (
5 ), and can result in distressing long-term psychological consequences (
5 ). On inpatient units a relatively small number of patients is responsible for most of the violence, and some offend repeatedly (
3,
11 ). Nevertheless, prosecution of assaultive patients is uncommon; only about two dozen reports of such prosecutions have been published to date (
12,
13,
14,
15,
16 ).
We conducted a comprehensive literature search of PubMed, Cochrane databases, PsycINFO, and PsychLit—utilizing various combinations of the following search terms: "assaultive patients," "ethics," "psychiatric inpatients," and "law"—in order to identify relevant domains of ethical consideration. We found that a number of authors have attempted to identify diverse ethical considerations related to the question of whether to seek prosecution of psychiatric patients for violent behaviors on inpatient units (
12,
17,
18,
19 ). However, these ethical analyses are incomplete because either they have not explicitly identified or developed all of the relevant ethical considerations, in particular the role of the professional virtues, or they have not identified factors relevant to the strength of the arguments generated by these considerations (
12,
17,
18,
19 ).
To remedy these shortcomings, we developed a comprehensive ethical framework to assist psychiatric health care professionals in arriving at explicit, reasoned judgments about whether to seek prosecution of assaultive psychiatric patients. We accomplished this by identifying relevant ethical considerations, the arguments generated by those considerations, and how to assess the strength of such arguments. Using a case scenario, we illustrate how the arguments and their respective strengths should be used to reach a judgment about recourse to criminal prosecution. We focus on the inpatient setting because psychiatrists and nurses are most commonly assaulted in these settings and because they have more control over how to respond to such assaults given that the patient often is not able to leave the hospital.
A distinctive feature of our ethical analysis is the central importance of the professional virtues in making such judgments. The virtues are traits of character that should be cultivated so that physicians routinely discern and discharge moral obligations to patients (
20 ). The motivation for our emphasis on the professional virtues is threefold. First, by serving as a constraint on self-interest, the virtues can help to focus the psychiatrist's concerns on the needs and interests of patients. Second, the virtues can protect against the possibility that strong feelings evoked by assaultive patients will undermine the standard of care. Third, by cultivating the professional virtues the psychiatrist functions as a role model for other professionals on the team (
20,
21,
22,
23,
24 ).
Relevant ethical considerations
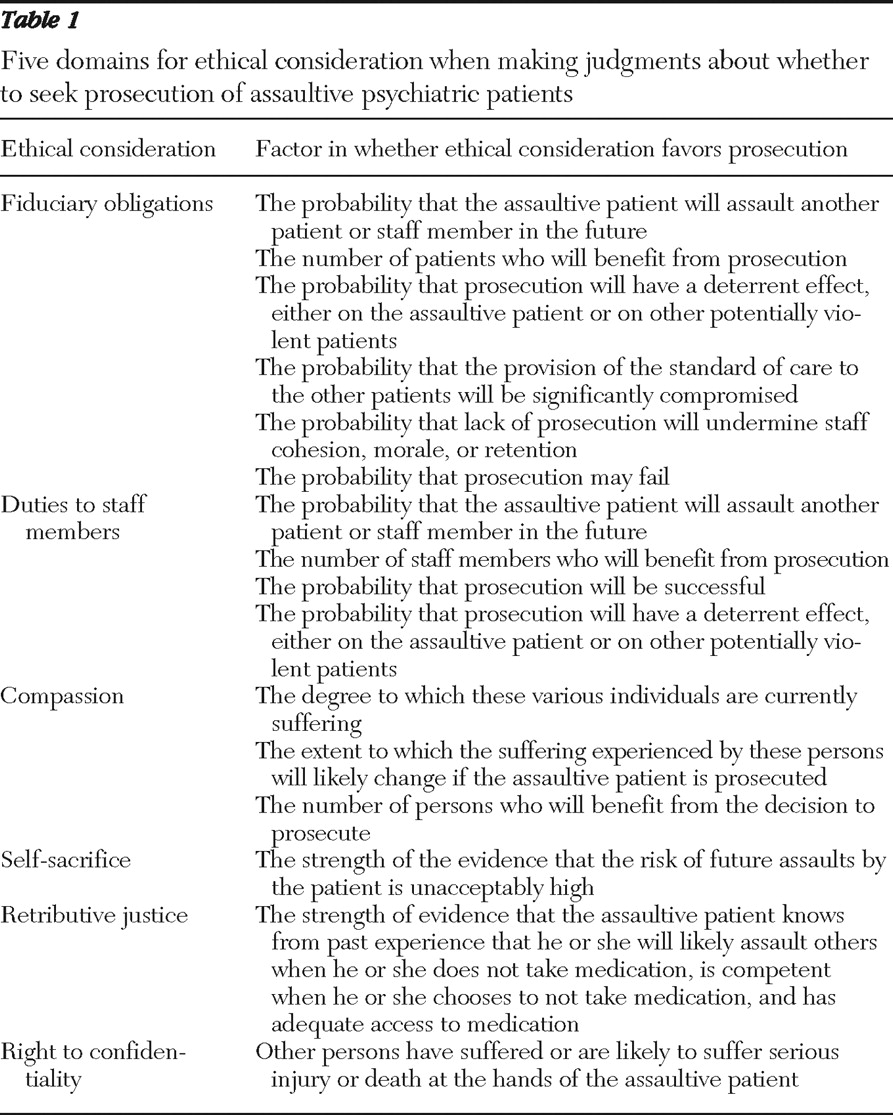
We identified five domains for ethical consideration in making judgments about whether to seek prosecution of assaultive psychiatric patients (
Table 1 ).
Fiduciary obligations
Psychiatrists and other mental health professionals have a fiduciary obligation to pursue courses of action that are reliably expected to advance the health-related and other interests of their patients (
20,
21,
22,
23 ). Fiduciary obligations exist independently of the decision-making capacity or autonomy of the patient. Prosecution may be in the assaultive patient's interest if it helps to restore autonomy or deter the assaultive patient from committing additional assaults (
17,
25,
26 ), foster relief from the experience of guilt over having harmed others, or educate the assaultive patient about appropriate behavior. However, even if this is not the case, the psychiatrist may still have a fiduciary obligation to pursue this course of action if he or she judges that prosecuting the assaultive patient will likely advance the best interests of other patients by protecting their safety or that it will serve as a deterrent to other potentially violent patients (
25 ). In these ways, the interests of other patients can sometimes reasonably be judged to outweigh the interests of the assaultive patient.
When deciding whether prosecution is in the interest of other patients, it is important to consider whether a failure to seek prosecution would likely compromise the provision of the standard of care to those patients and thus be inconsistent with fiduciary obligations to them. A particular concern is that the resources needed to adequately monitor an assaultive psychiatric patient could be used to meet the clinical needs of other patients in the unit or patients waiting in the emergency center for admission. Additionally, a failure to prosecute may in some cases have deleterious effects on staff cohesiveness or effectively create a "hostile" work environment, leading some staff members to consider resigning (
25 ). These effects could compromise the overall provision of the standard of care to all patients. The decision regarding whether or not to prosecute should thus take into account its likely effects on staff cohesion, morale, and retention.
The strength of an argument based on fiduciary obligations depends on the probability that the assaultive patient will act violently again in the future; the number of patients who will benefit from prosecution; the probability that prosecution will have a deterrent effect, either on the assaultive patient or on other patients; the probability that the provision of the standard of care to the other patients will be significantly compromised by not seeking prosecution; and the probability that a failure to prosecute will undermine staff cohesiveness, morale, or retention.
In assessing the strength of this argument, one must also consider the possibility that an attempted prosecution may be unsuccessful. Here it is important to underscore that our argument is framed in terms of probability: if prosecution will have a deterrent effect, then the argument weighs in favor of prosecution; if prosecution is likely to fail, then it obviously will not have a deterrent effect, in which case the argument will weigh against prosecution. The determination of the probability of successful prosecution will, presumably, vary from case to case.
Duties to staff members
In addition to fiduciary obligations to their patients, health care professionals also have a duty to protect the well-being of their colleagues by preventing them from being seriously harmed (
18 ). Therefore, when considering whether to seek prosecution, the interests of staff members should be taken into account.
If the patient is likely to assault staff members in the future despite their best preventive and treatment efforts, then it is reasonable to assume that it is in the interests of the staff that the assaultive patient be prosecuted and thereby transferred from the ward. The number of staff members who might benefit from prosecution remains a salient consideration; if many more persons will benefit significantly, then an argument can be made in favor of prosecution, even if the assaultive patient does not benefit. Health care professionals also need to consider the probability that the patient will be successfully prosecuted. Finally, consideration should be given to the probability that prosecution will have a deterrent effect in the future, either on the assaultive patient himself or on the other patients. This should include the possibility that prosecution may fail.
In sum, whenever it is probable that an assaultive patient will continue to be violent in the future, many staff members likely will benefit significantly, the patient will be successfully prosecuted, and prosecution is likely to have a deterrent effect, then this argument will generally favor prosecution (
17 ).
The strength of this argument depends on the number of staff members whose interests will be affected and the significance that we should attach to those interests. In particular, the health-related interests of staff members should not be sacrificed when they are at risk of serious, far-reaching, and irreversible harm from an assaultive patient. We acknowledge that risk is difficult to assess and predict, but we note that our proposed framework does not require certainty, only a high probability of risk.
Professional virtues
Throughout much of the history of modern medical ethics, it has been widely held that as fiduciaries, medical professionals should conduct themselves according to a virtue-based ethic (
21,
22,
23 ). Some contemporary virtue ethicists hold that a virtue-based ethic can guide actions (
27,
28 ). The well-recognized professional virtues of compassion, self-sacrifice, and self-effacement are particularly relevant in the case of prosecuting assaultive patients (
20,
21,
22,
23,
24 ).
The virtue of compassion requires that psychiatric health care professionals pursue the course of action that best alleviates the suffering of all those directly affected by the assaultive patient's aggressive behavior. In most cases, health care professionals need to consider the suffering experienced by the assaultive patient's victims, other staff members, patients who have not yet been assaulted but may feel threatened or intimidated, and the assaultive patient. In general, this argument will favor prosecuting the assaultive patient if it can be judged that the suffering experienced by the assaultive patient is less significant than that experienced by the other individuals.
The strength of an argument based on the virtue of compassion will depend on the degree to which these various individuals are currently suffering, the extent to which the suffering experienced by these persons will change if the assaultive patient is prosecuted, and the number of persons who will benefit in terms of relief from suffering from the decision to prosecute. Suffering includes both physical and emotional injury, so assessment of suffering should take account of both.
The virtue of self-sacrifice is the disposition to accept some risks to one's own safety, within reasonable limits, in order to fulfill fiduciary obligations of treatment. For example, this virtue may require that psychiatric health care professionals accept some risk to their own safety if doing so is necessary to ensure appropriate treatment of a patient. However, enduring violent assaults is not intrinsic to the treatment of psychiatric patients. Therefore, when psychiatric health care professionals judge that the risk of further violence from an assaultive patient is a strong possibility, they should conclude that the limits of self-sacrifice have been reached. The strength of an argument based on the virtue of self-sacrifice will turn on the strength of the evidence that the risk of future assaults by the patient is genuine.
The virtue of self-effacement works in conjunction with the virtue of self-sacrifice to focus the psychiatrist's concern on the patient. Self-effacement obligates the psychiatrist to put aside factors that should not count as relevant to the provision of treatment. Feelings such as anger, fear, and foreboding for the safety of oneself and others can cloud judgment and unhinge the fiduciary relationship (
24 ). Psychiatric health care professionals who discipline themselves on the basis of self-effacement are more likely to act on the basis of reasoned arguments than strong feelings. Such reasoned arguments are ideally supported by mentorship and collaborative input from the other members of the treatment team.
Retributive justice
The ethical concept of retributive justice is relevant when considering whether to prosecute assaultive patients. In ethics (as well as in law) retributive justice requires that we appropriately punish individuals who deserve to be punished (
29,
30 ), for example, those who have committed violent criminal acts.
An argument based on the concept of retributive justice will favor prosecuting psychiatric patients who are reliably judged by psychiatrists to meet thresholds of capacity related to their understanding of and responsibility for their actions and consequences when they attack patients and staff members. Formal determinations of capacity and of exculpatory lack of capacity are decided by courts on the basis of expert psychiatric testimony. Thresholds of capacity to stand trial are best determined by balancing decision-making capacity with the seriousness of the charge (
31 ). An interesting aspect of the argument from retributive justice is that it may also favor prosecuting assaultive patients who lack capacity at the time they attack patients or staff, provided all of the following conditions are met: patients knew from past experience that they will likely assault others when they do not take their medication, they were competent when they chose not to take their medication, and they had adequate access to their medication and psychiatric follow-up. That is to say, contrary to some accounts (
26 ), there can be cases in which prosecution is permissible even when a correlation between violent behavior and an underlying state of mental illness can be shown. The strength of an argument to this conclusion will turn on the weight of the evidence demonstrating that the three conditions listed above have been met.
Right to confidentiality
Patients enjoy a right to confidentiality—that is, the right to keep information that one discloses in confidence private. The key element in the right to confidentiality is that the information was disclosed in confidence (
20 ). The patient has a right to confidentiality; this right is a claim against the health care provider, who bears an obligation to fulfill or protect that right unless overriding considerations exist.
The right to confidentiality is often invoked in arguments that it is inappropriate to seek prosecution of assaultive patients (
17,
18,
25,
26,
32 ). The claim is that psychiatric patients have a right to control access to health-related information about themselves and that seeking prosecution of such patients violates this right. In ethical theory, however, it is commonly acknowledged that individual rights, including the right to confidentiality, carry little significance or are even waived or nonexistent when an aggressor causes other persons to suffer or puts them at risk of suffering, serious injury, or death at the hands of an aggressor (
17,
18,
33,
34,
35 ). Conversely, the right to privacy will carry greater weight to the extent that these outcomes are less likely to occur.
Applying the framework
Consider the case of Mr. B shown in the box on this page. In light of the fact that Mr. B has assaulted staff multiple times during this hospitalization, both the argument from fiduciary obligations and the argument from duties to staff members support the conclusion that it is in the interests of the other patients and staff that Mr. B be prosecuted, because he poses a real and substantial threat to their well-being. It is also in the interest of the other patients to prosecute Mr. B because the resources that are being used to monitor and house him could be better used to treat several other nonviolent patients. On the basis of the criteria set out above, one should conclude that these arguments carry great weight in this case.
An argument based on compassion goes in both directions—both for and against seeking prosecution. The suffering experienced by the patient's most recent assault victim, the other patients on the psychiatric unit, and the unit staff might be reduced considerably if Mr. B is prosecuted successfully. Should he remain on the psychiatric ward, he will likely suffer from isolation from the rest of the patient population. On the other hand, sending him to a forensic unit and seeking criminal prosecution could risk increased suffering on his part.
The virtues of self-effacement and self-sacrifice would normally count against prosecution. However, given the real risk of future violence on Mr. B's part, it follows from the above framework that the limits of self-effacement and self-sacrifice have been exceeded in this case.
The argument based on retributive justice strongly favors seeking prosecution. Before this latest series of assaults, Mr. B had been living in a halfway house where he had access to his medications. He also was informed about and therefore aware of the probable consequences of not taking his medication. On several occasions, failing to take his medications had led to his acting violently and being subsequently arrested. Moreover, it was noted that on previous discharges he had achieved a fairly high level of independent functioning, thus constituting prima facie evidence of competence (despite the difficulty of retrospective judgment). Therefore, there is good reason to hold Mr. B morally accountable, which also suggests that retributive justice carries much significance in this case.
At first glance, it appears that the argument based on the right to confidentiality favors not seeking prosecution of Mr. B, because doing so would result in persons having access to information that he has a right to keep private and would likely wish to keep private. However, as explained above, because of the risk of additional assaults, this right either carries little significance in this case or else is nonexistent.
This ethical analysis can now be summarized as follows: the arguments based on fiduciary obligations, duties to staff members, retributive justice, and the limits of self-sacrifice all favor prosecution, and much significance can be attached to each of these arguments; an argument based on compassion can be made in both directions, and each argument will be relatively weak because of the countervailing force of the opposing argument; and the argument based on the right to confidentiality carries little significance. It follows that it would be ethically justifiable in this case to refer the patient to the criminal justice system for consideration of prosecution.
Conclusions
When deliberating about prosecuting assaultive psychiatric patients, mental health professionals should comprehensively incorporate ethical considerations into their decision-making process in order to arrive at reasoned justification for the resulting decision. Such a comprehensive approach takes account of the professional virtues in clinical judgment and practice, especially compassion, self-effacement, and self-sacrifice. This virtues-based approach serves to protect and promote the interests of patients and to prevent strong feelings from undermining clinical judgment.
We emphasize that decisions about seeking prosecution of assaultive patients should not become formulaic (
36 ). Mathematical weights cannot be assigned to each of the considerations we have identified. Instead, individual decisions are a matter of considered judgment. Our argument-based approach suggests, however, that the apparent disinclination to seek criminal prosecution of assaultive psychiatric patients may not be ethically justified.
Acknowledgments and disclosures
The authors report no competing interests.