Suicide is a serious public health challenge, ranking as the 11th most frequent cause of death in the United States. In 2004 suicide took the lives of over 32,000 Americans of all ages, and estimates of the number of attempts for every death suggest that an additional 380,000–780,000 individuals survived a suicide attempt in that year (
1,
2 ). Persons with mental and substance use disorders, the elderly population, youths, and people with general medical illnesses are at particularly high risk of attempting suicide (
3 ).
Among the causes of premature mortality among people with severe mental illness, deaths from external causes (suicide, accidental death, and homicide) rank second only to coronary heart disease (
4 ). Compared with other people at poverty levels, individuals with severe mental illness alone are twice as likely, and those with mental illness and a co-occurring substance use disorder are four times as likely, to die from these external causes (
5 ). These statistics are not surprising, given the vulnerability of people with severe mental illness to social and individual risk factors for suicide, including alcohol and drug use problems, childhood and adult victimization, sparse social networks, and, the best predictor of eventual completed suicide, prior attempts (
2,
6,
7,
8,
9,
10,
11,
12,
13,
14 ). Multiple and prolonged stressors such as these degrade a person's quality of life and contribute to social isolation and feelings of hopelessness (
5,
15 ).
Efforts to transform health and mental health care in the 21st century recommend that services be consumer and family driven—that is, that they support service users' treatment preferences, values, and capacity to participate in decisions about their care (
16,
17,
18 ). Although the voices and values of those who have survived suicide attempts would strengthen and benefit suicide prevention efforts, they are strikingly absent in most quantitative research on suicide (
19 ). Despite the vulnerability to suicide of people with serious mental illness and the large number who have survived attempts, we know little about how those with prior suicide attempts specifically cope during subsequent episodes of hopelessness and depression when they consider suicide again; what are their coping skills and supports? Participatory research provides a context in which affected communities participate in all phases of research (
20,
21,
22 ). In this study, consumers formulated the research questions, used their networks to implement a modified focus group methodology, and collaborated in coding and interpreting the data and in writing this report.
This survey was carried out in consumer-led forums held in community-based, consumer-operated drop-in centers, mutual-support groups, and education and advocacy programs throughout New York State. Compared with traditional mental health service settings, these environments are experienced by consumers as safe: they are more inclusive, more supportive of self-expression ("telling our stories"), and more supportive of personal choice and mutual respect (
23 ), and they are less stigmatizing than support groups designed for people without mental illnesses (
24,
25 ). In this article, we describe coping strategies used by individuals with a history of suicide attempts, with the goal of suggesting how suicide prevention efforts can be congruent with strategies that high-risk consumers have found helpful.
Methods
Sample flyers posted at peer-operated settings that offer a variety of community-based services (housing, case management, peer drop-in, and education and advocacy centers) invited individuals diagnosed as having mental illness and who had a history of attempting suicide to participate in the Hope Dialogue, a 1.5-hour conversation and workshop to examine techniques that individuals used to prevent a slide into darkness and despair. Fourteen dialogues were conducted in the winter of 2005–2006 with 205 consumers of public mental health services in large and small cities and in rural counties across New York (mean attendance=14, range=five to 41). This study was approved by the Nathan S. Kline Institute Institutional Review Board.
Those who wished to participate in the study completed survey questions about demographic characteristics and access to each of the following supports when they were feeling suicidal: peer, therapeutic, family, spiritual, and community. Respondents wrote up to five coping strategies in response to the query "If your darkness and despair escalated to actual thoughts of suicide, what has helped you in the past to not take that action?" Responses from a total of 198 participants (97% of attendees) formed the basis for this analysis. At the time of the survey, verbal consents were obtained from participants, and no identifying information was collected.
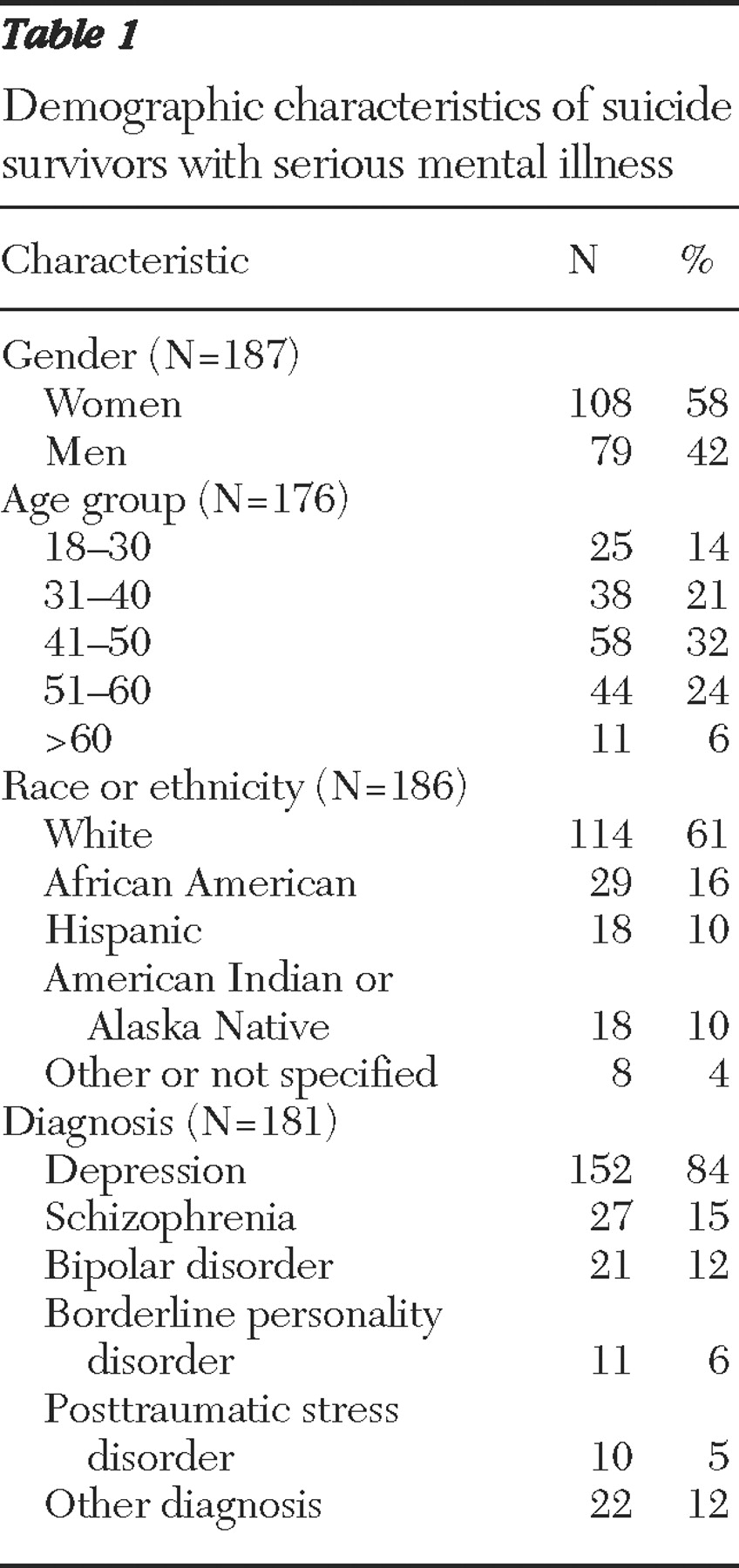
Sample characteristics
Table 1 shows participants' demographic characteristics. We compared study participants with 55,482 adults receiving mental health clinic and peer services in the 14 localities where the dialogues took place, using the most recently available data (2001) from a one-week survey of persons receiving mental health services from programs certified or funded by the New York State Office of Mental Health (
26 ). Whereas age and gender distributions of Hope Dialogue participants did not differ from the community sample, proportionately more Caucasians (
χ 2 = 10.88 df=1, p<.001) and fewer African Americans (
χ 2 =15.15; df=1, p<.001) and Hispanics (
χ 2 =16.26; df=1, p<.001) participated in the study than used community-based mental health services. The wording of the study question made mentioning other diagnoses optional, thus precluding detailed comparisons, but 84% of study participants did report a depression diagnosis compared with 39% (N=21,710) of the community sample. Other diagnoses reported in the table must be seen as low-end estimates.
Data
Respondents made 745 statements about coping strategies (averaging 3.8 per person). We used conventional qualitative research techniques to develop categories for data analysis (
27,
28 ). Grounded theory provides an iterative process in which multiple analysts examine qualitative data to identify coding categories. Here, two independent consumers categorized statements, two research scientists reviewed the categories and coding decisions, and all four coders agreed on consensus classifications where there were discrepancies. This process produced 16 categories: practicing spirituality (religious beliefs and practices), talking to someone and companionship, practicing positive thinking, using the mental health system, considering consequences of suicide to people to whom one is close, using peer supports, doing pleasurable things, protecting oneself from harmful means, doing grounding activities, considering consequences to oneself, doing structured tasks, maintaining sobriety, finding a safe place, helping others, seeking emotional outlets, and resting.
We describe the frequency distributions of different coping strategies in two ways. First, we considered only the initial responses (N=198), assuming that the first statement implicitly reflected an individual's most accessible and salient coping strategy; second, we considered all responses equally (N=745). We compared the rank-ordered distribution of the first-named strategy by respondents' gender, age, racial-ethnic group, and presence of a depression diagnosis.
Results
Coping strategies
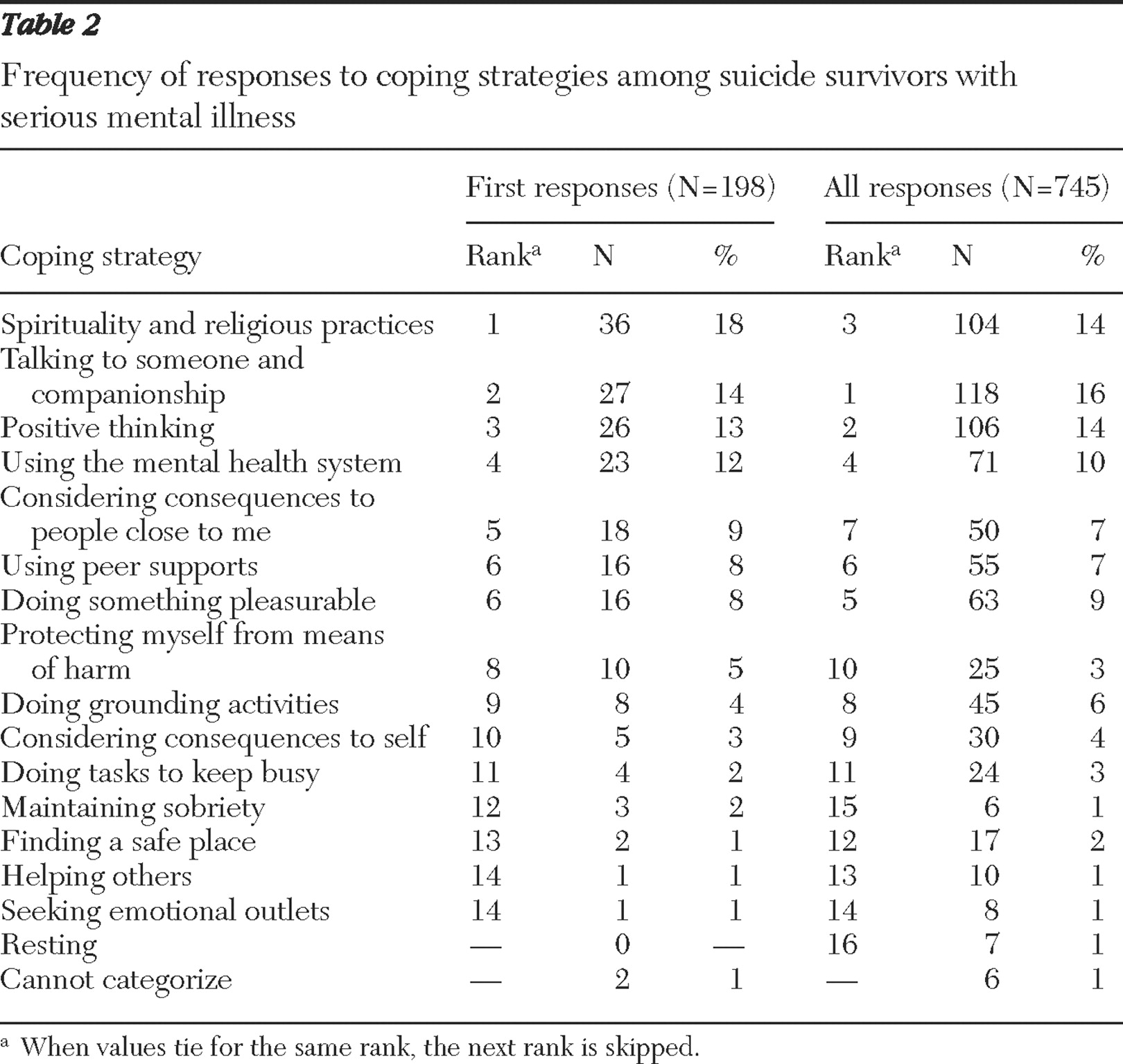
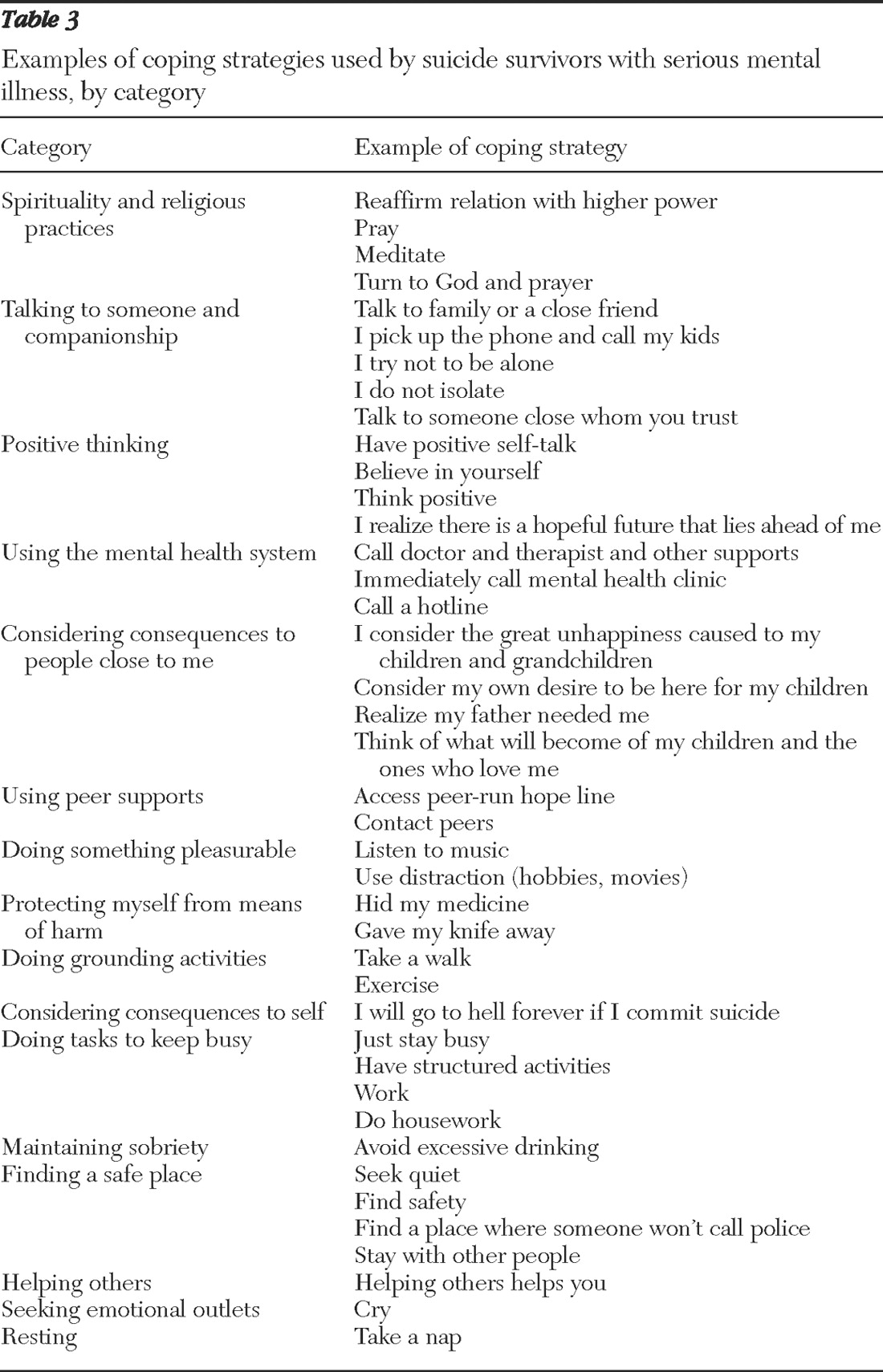
Table 2 shows the categories of initial and total responses ordered by the frequencies of the first responses, and
Table 3 provides examples of statements made by respondents in each of the broad categories. The three most frequently identified coping strategies, accounting for 45% of those named, were spirituality (18%), talking to someone and companionship (14%), and positive thinking (13%). These categories included statements about recognizing external sources of hope, avoiding isolation and keeping communication open, and not ruminating about the things that are going wrong. Each of these positive coping strategies counteracts hopelessness, isolation, and despair—all of which are closely associated with completed suicide.
The strategy of using the mental health system, which includes crisis hotlines, emergency services, or speaking to a therapist, was the fourth most cited, accounting for 12% of the narratives. Considering the consequences to key people in one's life (particularly immediate family members) and seeking out peer support were the next noted coping strategies, underscoring the importance of social networks to persons living in the community. Pleasurable activities serve to distract and refocus individuals, whereas avoiding the means to attempt suicide can protect the individual from dangerous and lethal impulses. When all responses were analyzed, a slightly different picture emerged. Talking to someone moved to the top of the list, positive thinking emerged as the second most frequently noted, which was followed by spirituality. Using mental health services remained at the fourth rank.
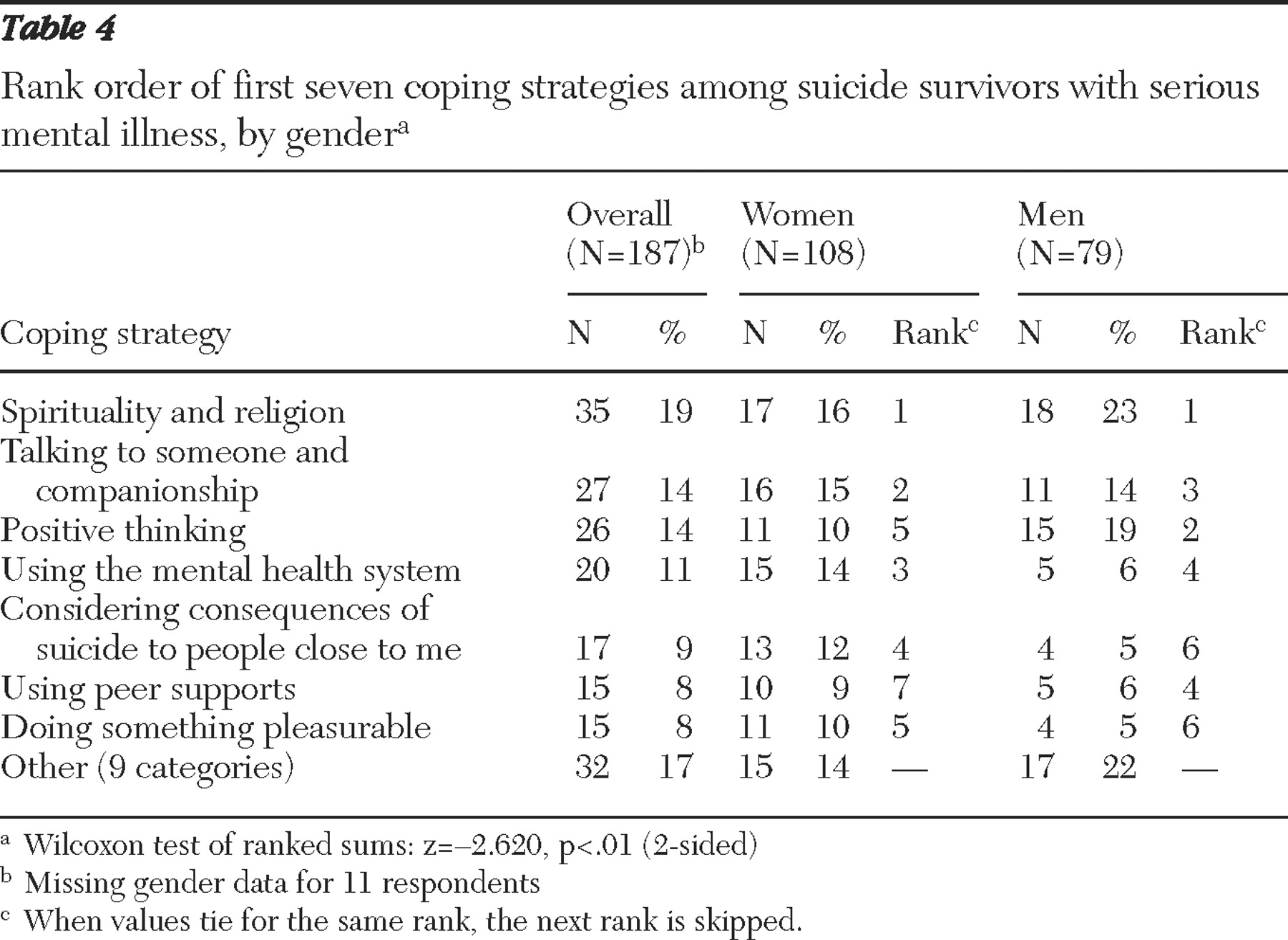
A Wilcoxon test of ranks was performed to determine whether the rank distribution differed by respondents' gender, age, racial-ethnic groups, and depression diagnosis. The ranking of first-named coping strategies, displayed in
Table 4, differed only for gender (z=-2.62, p<.01). Whereas men and women indicated spirituality as their first strategy, the table shows that a greater proportion of men cited this and positive thinking than women did. Women were more likely to cite using the mental health system and considering the consequences of their suicide to people close to them.
Availability of supports
Respondents were asked whether family, therapeutic, peer, spiritual, and community supports were available to them when they were feeling suicidal. Respondents most frequently said that family (N=111, 54%), therapeutic supports (N=111, 54%), and peer supports (N=102, 50%) were available. Eighty-one respondents (40%) said that spiritual supports and 49 (24%) said that community supports were available. Availability of supports did not translate into first choices for coping with suicidal thoughts, however, and some participants stated specifically that they would not bring this topic up with family members.
Discussion
Limitations
Study results are based on self-report by a convenience sample of people with severe mental illness and a history of attempting suicide who use consumer-operated drop-in centers across New York State. Participants may not represent the population at high risk of suicide; they were recruited in mutual-support settings. Women, Caucasians, and persons with depression diagnoses were overrepresented, and those with a schizophrenia diagnosis were underrepresented compared with users of community mental health services in the same localities. Furthermore, because we did not ask respondents specific questions about their suicidal history, it is not clear to what extent the sample represented those at highest risk.
The overrepresented groups in this sample are also more likely to have attempted suicide (
2,
29 ) and may have greater access to social networks that support positive coping. Depression may have been overrepresented because participants may have found the condition more salient than schizophrenia to self-report in the context of a conversation about suicide. Also suicide ideation is mood driven among individuals with schizophrenia (
30 ), who are highly likely to have additional psychiatric conditions (
29 ). Suicide survivors with schizophrenia diagnoses in the study settings may have chosen not to participate in the dialogues. Finally, overrepresentation of mood disorders in a study sample where 85% of participants were over age 30 is consonant with findings that most suicide deaths among individuals with schizophrenia occur during their 20s (
31 ), whereas suicide rates are more constant, although still elevated across the life span, among people with depression (
32 ).
The study methodology, which asked people to write up to five things they do when in deepest despair, may have identified only strategies uppermost in people's minds, which in turn may have been affected by participation in the dialogues themselves. Also, it would be useful to understand whether social, therapeutic, and spiritual supports are prominent and accessible coping strategies in a more ethnically representative sample.
Coping with thoughts of suicide
This research focused on strategies that people with psychiatric illness who survived suicide use to cope with their thoughts and impulses when in despair (
33 ). Their voices have been virtually unheard. Participants reported anecdotally that the dialogues provided a safe place to share the supports and strategies they have used to prevent suicidal thoughts from shutting down their lives.
The capabilities framework is an emerging approach to conceptualizing, studying, and acting on opportunities for social justice for people with psychiatric disability (
34,
35 ). The framework emphasizes the importance of determining the life dimensions most valued by people with lived experience—here, of coping with suicidal thoughts. Nowhere do key vision statements for suicide prevention (
3,
16 ) acknowledge the importance of shared communities of meaning (
25 )—self-help and mutual-support groups, for example—that people with mental illness construct, operate, and use. This study's results indicate that religious beliefs and practices, companionship, and a social network of family and peers are key coping strategies for people with a history of attempted suicide. Reported levels of reliance on formal mental health services were ranked lower, which raises questions about how responsive these services are to the articulated needs of consumers in crisis.
Spirituality
For coping, consumers most frequently relied on spiritual beliefs and practices rather than formal church affiliation. These practices support the pursuit of personal meaning and connectedness apart from the everyday world (
36,
37 ) and help in countering hopelessness, the single most consistent risk factor for suicide (
38,
39,
40,
41,
42,
43,
44,
45,
46 ) and a hallmark in the lives of people with mental illnesses (
36 ). Important reasons to live—including concern for children, family, and friends—cited by survivors in this study and other studies (
37 ) often fail to mitigate suicidal behavior (
38 ).
Religious faith and spirituality are generally associated with positive mental health outcomes and high levels of well-being: access to social supports, resilience to stress, emotional calmness and stability, inner strength and empowerment, sense of well-being, and lower risk of suicide (
47,
48,
49 ). Trauma survivors report that spirituality sustains recovery partly by transforming anger and disempowerment—both suicidal risk factors—into self-agency (
50 ). But some data suggest that clinicians may miss the benefit of spirituality in suicide contexts (
51 ) because they rate spiritual needs of patients with severe mental illness quite low, whereas patients themselves frequently rate spiritual needs higher than either housing or income benefits (
36 ).
Social support and positive coping
The capabilities framework applied to mental health highlights the essential role of connectedness in recovery, and the importance of social environments in providing opportunities for doing and being in everyday life (
52 ). Social structures can also minimize aspirations of persistently deprived groups, so that individuals internalize limited or maladaptive preferences, desires, and expectations to adapt to what is feasible (
34 ). People with positive psychotic symptoms and suicidal ideation are less optimistic about their conditions, feel less empowered to manage them, and hold more negative beliefs about themselves and others than those with no suicidal ideation (
30 ). This strongly internalized stigma can cause or maintain the avoidant coping styles associated with hopelessness, low self-esteem, and poor social functioning (
53,
54,
55,
56 ). And avoidance extended to services and social networks can potentiate suicide risk (
57 ). In contrast, active, problem-centered coping, such as positive thinking—ranked third in this study—fosters positive social functioning and self-efficacy among people with severe mental illness (
58,
59 ) and is associated with self-help involvement (
59 ). Cognitive-behavioral approaches to learning, modeling, and supporting these coping skills are effective and available for mental health practice, especially in wellness self-management (
58 ).
In 2002 in the United States, mental health mutual-support groups served over 41,000 people, self-help organizations had over one million members, and consumer-operated services served over a half-million clients and members (
60 ). Our results suggest that these environments may help diminish the stigma of suicidal thoughts and counteract feelings of hopelessness, worthlessness, and isolation, particularly because a majority of persons with mental illness do not receive formal treatment (
61 ). These services may also ameliorate risk by supporting participants to more effectively use traditional services (
62 ). In fact, potentially coercive and adverse consequences of engaging with traditional crisis services may be a factor in consumers' preferring peer environments to speak about this taboo topic, and more generally to access help through reciprocal, supportive relationships that psychiatric disability disrupts (
63,
64,
65,
66 ). Peer services reduce hospitalization rates and lengths of stay (
67,
68,
69 ) and may improve consumers' communication with physicians about medications and side effects, motivating them to develop wellness plans that identify pleasurable activities to support self-management (
70,
71 ). Perhaps most important, "like selves" model recovery and offer hope, empowerment, and enhanced self-esteem (
72 ).
Trusted therapist
Respondents also reported using traditional services, especially trusted therapists, during times when they contemplate suicide. Studies show that strong, enduring, mutually trusting relationships with clinicians support consumers who are facing potentially devastating challenges or taking positive risks to achieve recovery (
73,
74 ). With such support, people with psychiatric conditions, including those experiencing little pleasure and who are socially withdrawn, can develop and use positive skills to cope with stress and symptoms and to maintain and improve their wellness (
58 ).
Other aspects of the formal mental health system, such as emergency services or crisis hotlines, were not preferred, perhaps because suicidal thoughts are an instance where mental health consumers perceive that "telling is risky business" (
75 ), with potentially negative external consequences that are difficult to overcome. But not telling is risky too, contributing to isolation, rumination, and despair. By mandating therapeutic communication as privileged communication, successful suicide prevention programs have shifted the perception of help seeking from a reflection of weakness to evidence of strength and personal responsibility (
76,
77 ). Key vision statements also recognize that encouraging people to seek effective help for behavioral health problems and suicide will erode associated stigma and silence (
3,
16 ).
Large-scale suicide audits indicate that more responsive services could prevent many suicides (
78 ). Suicide survivors suggest that responsive behavioral emergency guidelines would incorporate availability of peer support throughout a crisis; hopeful, respectful listening and support; collaborative treatment decisions that consider consumers' reported medication experience; contact with their trusted therapists; and postdischarge support for survival, social, and mental health needs (
79,
80,
81,
82 ). In contrast, suicide follow-up services focus on medication, health, and sometimes counseling (
83,
84 ). Active psychosis is more salient in emergency admissions of suicidal individuals than known risks, including male gender, older age, any major psychiatric disorder, lack of stable housing, an ongoing clinical relationship, or low levels of access to timely outpatient follow-up (
85 ). Further, service strategies to minimize other-directed violence can be instructive for minimizing self-directed violence: engaging people before and during a crisis with personal and peer support; providing stable housing and employment; and addressing isolation, poverty, and substance use (
86 ).
Conclusions
Personal experiences of coping with suicidal thoughts are minimally available to support suicide prevention efforts, partly because of stigma associated with these thoughts and partly because of the singular focus on crisis that characterizes official responses to them. Furthermore, the dual stigmas of mental illness and attempted suicide are destructive to self-esteem and positive coping, leaving people truly on their own in some of their most vulnerable hours. Services that fail to fully understand a person's pervasive depression and hopelessness or to provide ongoing therapeutic support miss opportunities to prevent suicide (
78 ). Our results suggest that prevention efforts should acknowledge mental health consumers' broader reliance on spiritual, family, and peer supports and trusted therapists. Tools that support wellness, integrate consumers' personal "medicine" into their use of formal mental health services (
87 ), and incorporate advanced directives into crisis services (
82,
88 ) provide frameworks for a more consumer-driven system of care. Suicide prevention initiatives must acknowledge peers, families, and spiritual networks as key frontline responders to suicidal crises and provide them tools, training, and access that allow them to be sources of solace and hope in ways that indeed are responsive to lived experience.
Acknowledgments and disclosures
This study was supported in part by grant P20-MH0781880 from the National Institute of Mental Health. The authors acknowledge the technical contributions of David Bertollo, B.A., to the analysis of these data and the implementation support of the Mental Health Empowerment Project.
The authors report no competing interests.