This study was a retrospective medical record review of veteran decedents identified by county medical examiners as having completed suicide in the state of Oregon between 2000 and 2005. Approvals for this study were obtained from the local VAMC institutional review board (exempt status) and from the Oregon Public Health Division.
Data sources and population
OVDRS provided death certificate data for decedents aged 18 and over who completed suicide in Oregon between 2000 and 2005. OVDRS data included the last four digits of each decedent's Social Security number, name, date of birth, date of death, cause of death, veteran status, sex, race-ethnicity, highest level of education, and marital status. The OVDRS defines suicide death by
ICD-10 codes X60–X84, and Y87.0 as the underlying cause of death on death certificates. In a previous nationwide comparison of Vietnam-era veteran death certificates and medical review data, death certificate recording of suicide was 90% sensitive and specific (
12 ).
We matched OVDRS data to administrative data from the VISN 20 Data Warehouse using the last four digits of the Social Security number, name, and date of birth. The VISN 20 Data Warehouse contains data extracted from the electronic patient record files of regional VA facilities; it is updated monthly, and reliability checks are performed regularly. The VISN 20 Data Warehouse has been used in previous studies of utilization of services and medications (
13,
14 ). Veteran status was assigned if the decedent was designated as a veteran by either VISN 20 or OVDRS data. A national comparison between death certificates and the U.S. Census Bureau's Population Survey indicated that the designation of veteran status on death certificates agrees 95% of the time with baseline veteran status (
15 ). On the basis of utilization data extracted from the VISN 20 Data Warehouse, we identified 114 veterans who had received health care services at any of the programs or clinics belonging to the VAMC system in the 12 months before death. Receipt of services was defined as any contact, including phone, prescription refill, inpatient stay, and outpatient visit. Using medical record review, we then identified the 112 veterans who had one or more phone or in-person contacts with health care personnel characterized by two-way communication between the patient and health care personnel. These did not include phone messages, letters, or requests for prescription refills. This group (N=112) constituted the sample for this study.
We manually reviewed patient medical records for the 112 veterans to determine whether any clinician assessed the veteran for symptoms of depression, a substance use disorder, PTSD, or suicidal ideation. These psychiatric features were chosen on the basis of evidence of association with suicide risk (
7,
8,
9,
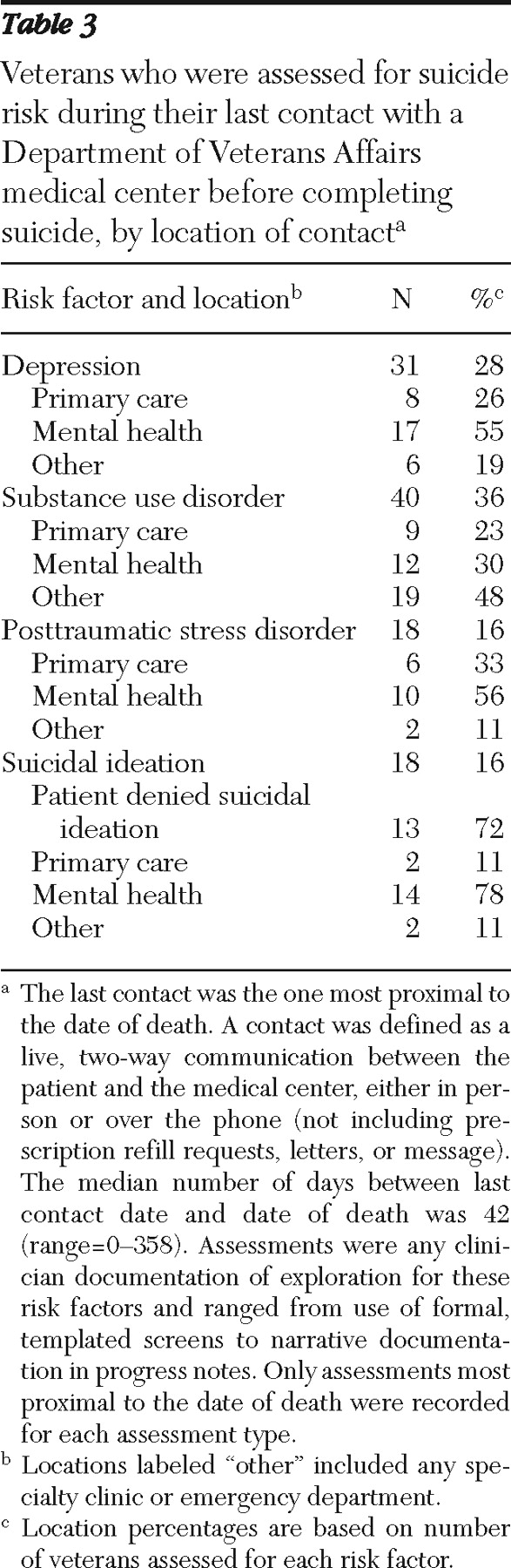
10 ). Assessment was defined as any clinician-documented exploration of these risk factors, ranging from use of formal, templated screening tools to narrative in progress notes. Although screening tools were in use during the time frame of this study for depression, substance use, and PTSD, formal screening tools for suicidal ideation were not. For each of these risk factors, we recorded the assessment (if any) most proximal to the date of death. We also report whether this assessment occurred within 30 days before death and whether it occurred during the contact most proximal to the date of death (last contact).
When the patient record documented current suicidal ideation, we also recorded whether the clinician documented assessment of additional suicide risk and protective factors (
16 ), either that day or within 30 days. This included discussion of previous attempts; determination of passive versus active suicidal ideation; documentation of hopelessness, impulsivity, recent losses or stressors, access to lethal means, and social support; and arrangement for clinical follow-up. Passive suicidal ideation was defined as having thoughts about suicide or about being better off dead but no specific ideation about methods or intent to harm oneself. Active suicidal ideation included expressing a desire to die, identifying a possible method, or specific planning or intent.
For each veteran's last contact, we recorded clinician-documented reasons for the contact (either a routine follow-up or a patient-initiated contact for a new or exacerbated medical concern) and whether the clinician noted any emotional distress. Last contacts were considered to be follow-ups if the patient and clinician discussed conditions previously known to the clinician and if the visit was not clearly initiated by the patient's concern over exacerbation of a known problem. Emotional distress was indicated by documentation of distress over a particular general medical or mental health concern (diagnoses were not sufficient) or difficulty coping with stressful life events. We also recorded whether the patient had received non-VA health care during the year before death, as indicated by outside medical records embedded in the VA electronic record or VA clinician notation in progress notes.
After initial testing and subsequent refinement of a medical record review checklist and development of a codebook, two trained reviewers (LMD and MCC) reviewed each patient's chart. When there were disagreements, a third reviewer (SKD or KCD) arbitrated.
Demographic data were extracted from OVDRS data, and ICD-9-CM diagnostic and utilization data for the year before death were extracted from the VISN 20 Data Warehouse.
Setting
The VAMC is a general medical and surgical teaching facility with five primary care clinics, which served approximately 42,000 veterans enrolled during the study period (2000–2005). Two primary care clinics located in a metropolitan area served approximately 28,000 patients during this period. Clinics were also located in another medium-sized city (serving 6,000 patients) and two rural locations (serving 1,000 and 4,000, respectively). Since 1998, all inpatient and outpatient progress notes, prescription refills, and phone contacts have been maintained in a systemwide electronic patient record system.