Baseline study
Design and participants. Baseline assessments and follow-up assessments were conducted in 2001–2003 and 2004–2007, respectively, at the faculty and resident group practice of the Division of General Medicine, Columbia University Medical Center in New York City. Each year 18,000 adult patients account for approximately 80,000 outpatient visits to the practice. Patients are from the surrounding communities in northern Manhattan, and most are Medicaid or Medicare beneficiaries. Baseline study methods have been described in detail elsewhere (
31,
32 ).
Briefly, patients were systematically approached on the basis of the position of the seat that they freely selected in the clinic waiting room. Eligible patients were between 18 and 70 years of age, had made at least one prior visit to the practice, could speak and understand Spanish or English, were waiting for face-to-face contact with a primary care physician, and had no health problems that would prevent them from completing the survey. Of the 1,346 patients who met eligibility criteria, 1,156 consented to participate and completed the survey (86% response rate).
Information was collected on demographic characteristics. Social, family, and work functioning was assessed with the Sheehan Disability Scale (SDS) (
33 ). The Medical Outcomes Study Short-Form Health Survey (SF-12) (
34 ) and selected questions from the Social Adjustment Scale-Self Report (
35 ) were also used. For this study, the work item on the SDS was excluded from total SDS scores because only one-fifth of the sample was gainfully employed. Information about mental health treatment history, including the types of psychotropic medications prescribed during the past month, was reported by the patient.
All assessment forms were translated from English to Spanish and back-translated by a bilingual team of mental health professionals. Records were linked with the hospital administrative database to obtain the frequency of outpatient, inpatient, and emergency service contacts during the 12 months before the follow-up assessment as well as the ICD-9-CM diagnoses for each contact. The institutional review boards of Columbia University Medical Center and the New York State Psychiatric Institute approved the study protocol, and all participants provided informed written consent.
Screens for psychiatric disorders. Patients were screened for major depressive disorder, generalized anxiety disorder, panic disorder, and alcohol use disorder, using the PRIME-MD Patient Health Questionnaire (PHQ) (
28,
29 ). A drug use disorder module patterned after the PHQ alcohol use disorder module was also administered. Because of low prevalence rates, two pairs of disorders were combined for analytic purposes: alcohol and drug use disorders, and generalized anxiety disorder and panic disorder.
The Mood Disorder Questionnaire (MDQ) (
26,
27 ), which has also been validated in primary care (
36 ), was used to screen for bipolar spectrum disorder. Although the time frame of the MDQ is not restricted to the present, we considered a positive MDQ screen indicative of bipolar spectrum disorder even if the patient was not in a current episode, because bipolar disorder is considered a lifetime disorder.
Treatment for psychiatric disorders. Patients were asked, "Have you ever been treated for an emotional or mental problem?" and if yes, "When was the last time you were treated for an emotional or mental problem?" Patients were also asked, "Have you ever taken a prescribed medication for an emotional or mental problem?" and if yes, "When was the last time that you took a prescribed medication for an emotional or mental problem?" Both questions about the timing of treatment had the following response choices: more than one year ago, less than one year ago but not in the last month, and in the last month. Patients who had been treated or took medication less than one year ago were defined as currently receiving mental health treatment.
Follow-up study
Design and response rate. The mean±SD time between baseline and follow-up interviews was 3.7±.5 years. Our follow-up assessment included an extended interview administered by clinically trained, bilingual and bicultural interviewers who were blind to the initial clinical data. Of the 1,156 participants at baseline, 825 (71%) consented at baseline to be recontacted for a follow-up interview. Because of financial constraints, letters were sent to only the first 796 patients; thus 29 of the 825 consenting patients were not invited. Among those who were sent letters about the follow-up study, the follow-up clinical status of 70% (N=561) was determined. These patients were either interviewed at follow-up (N=519) or found to be deceased or unable to participate because of institutionalization or illness (N=42). The 561 follow-up participants represent 49% of the original sample of 1,156. Our interest was in 348 of the 561 patients who screened positive at baseline for at least one of the mental disorders and had not received mental health treatment during the year before screening.
Clinically assessed psychiatric disorders. At follow-up, major sections of the Structured Clinical Interview for DSM-IV-TR (SCID) Axis I Disorders (
37 ) were administered by experienced, clinically trained interviewers who prepared a narrative summary of the interview. Based on all available follow-up data, one of the authors (MMW) completed best-estimate diagnoses blind to the initial screening status (
38 ). The diagnostic reviewer and the interviewer discussed any wide discrepancies. Current disorders were categorized as major depressive disorder, anxiety disorder (generalized anxiety disorder or panic disorder), substance-related disorder (including alcohol or substance abuse or dependence and alcohol- or substance-induced mood, anxiety, or psychotic disorder), and bipolar spectrum disorder (bipolar type I or II disorder or bipolar disorder not otherwise specified). Disorders were considered present if they were rated as "definite" or "probable," except for substance-related disorders, which were also considered present if rated as "possible" because of a tendency for patients to underreport substance-related disorders (
39 ).
Data analysis
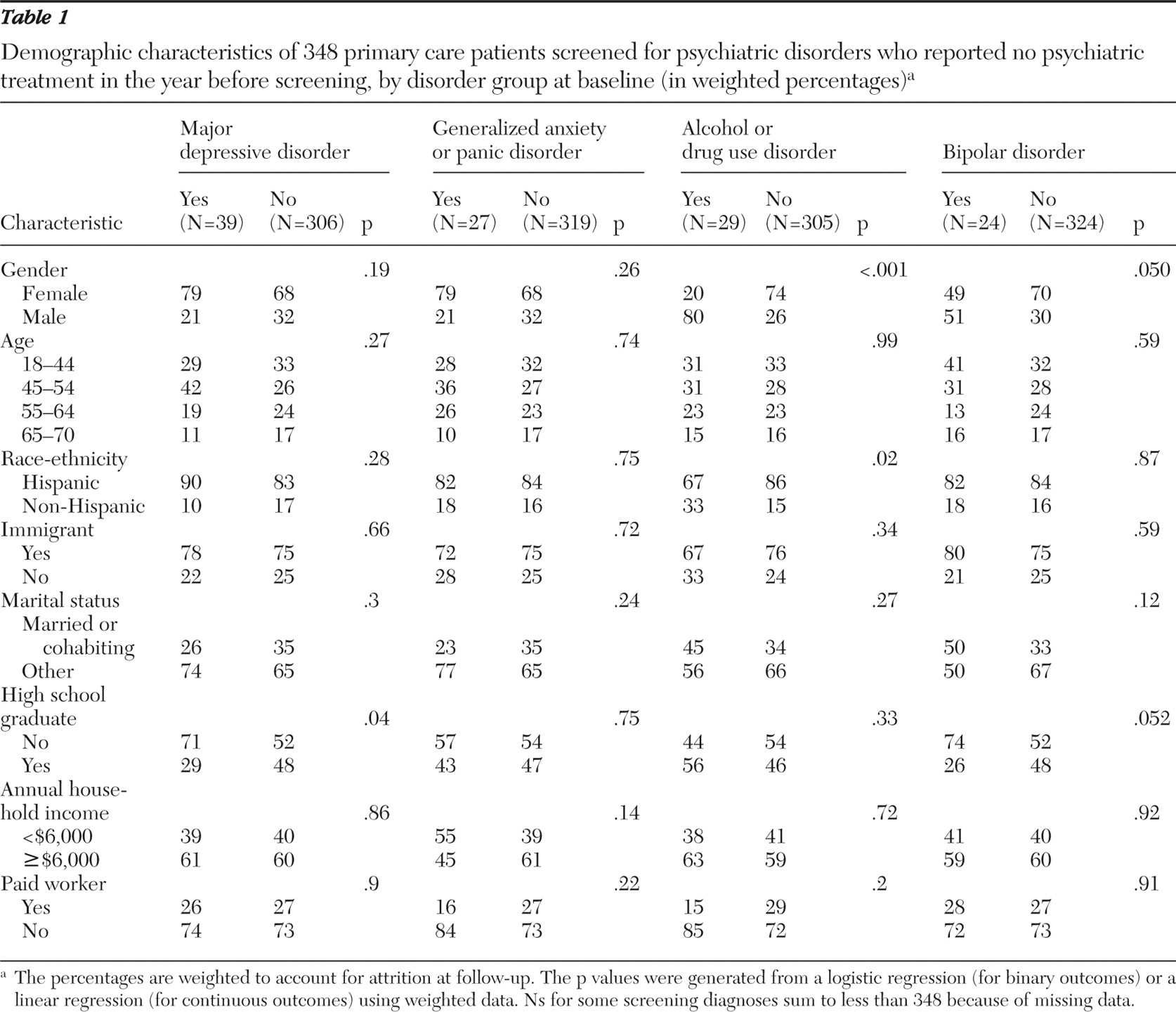
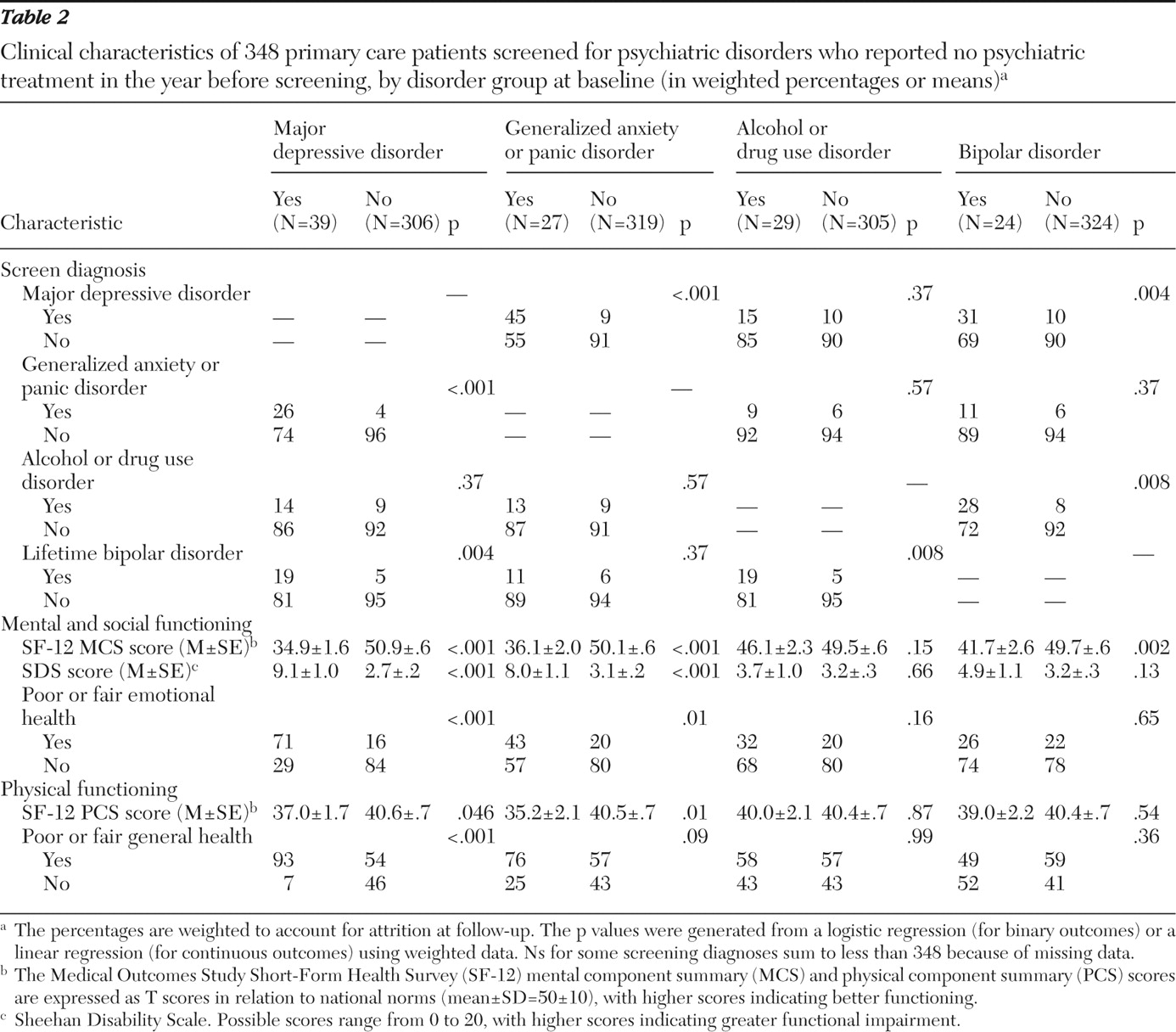
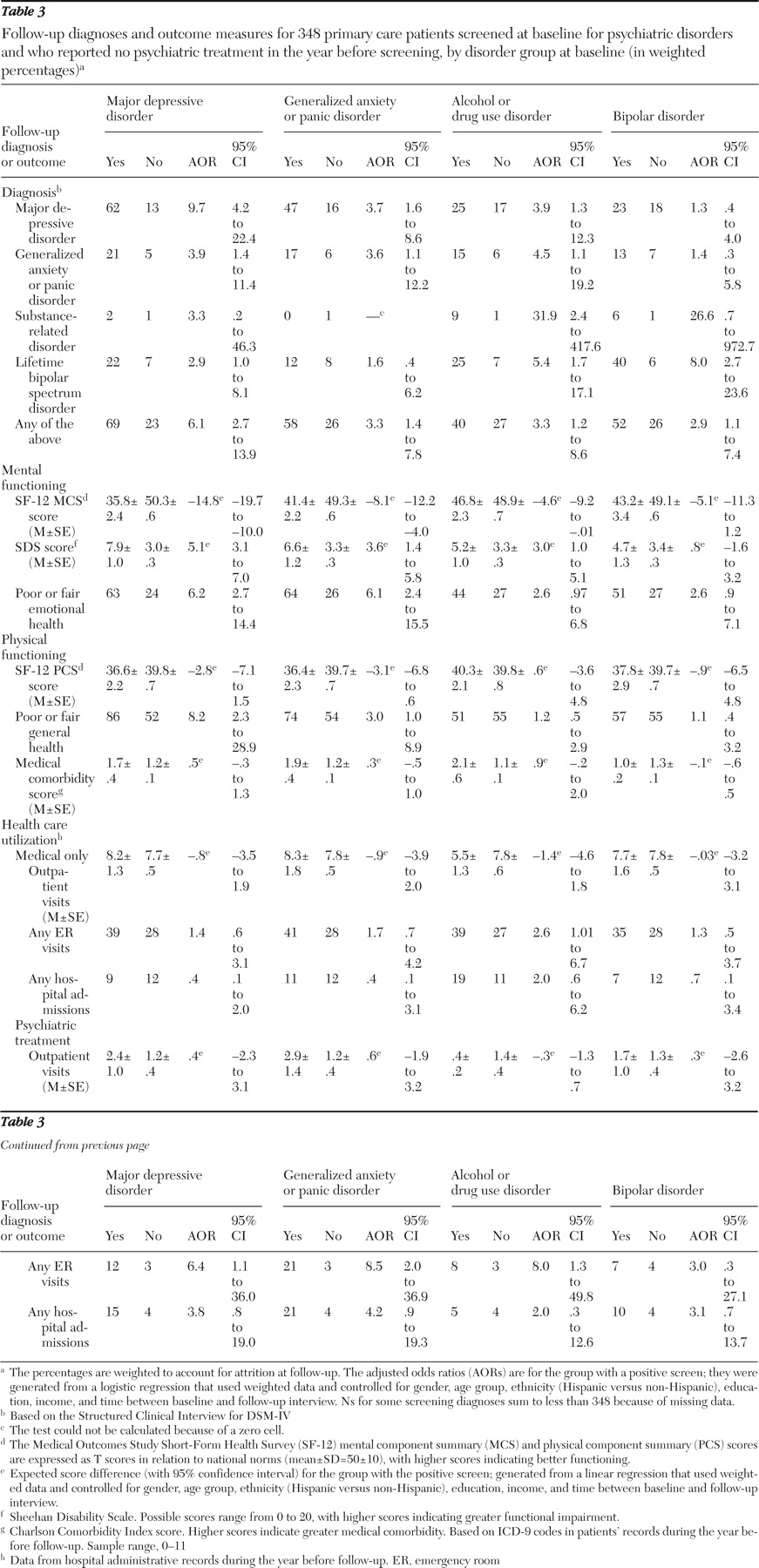
Our primary analyses were restricted to the 348 patients who screened positive for a disorder at baseline and who reported that they had not received mental health treatment in the year before screening. For each of the screened disorders (major depressive disorder, generalized anxiety disorder or panic disorder, alcohol or drug use disorder, and bipolar disorder), we compared patients by screening status (positive or negative) on various measures that were assessed at follow-up, including clinical diagnoses based on the SCID and health and functioning. Using hospital administrative records for the 12 months before each follow-up assessment, we compared baseline screen-positive and screen-negative groups on total number of outpatient visits, emergency department visits, and hospital admissions. We separated all visits and admissions into those that included at least one mental disorder diagnosis (
ICD-9-CM codes 290–319) and those that included no mental disorder diagnosis. Because emergency department visits and hospital admissions were relatively rare, we coded each variable as any versus none. The Charlson Comorbidity Index (
40 ) was used to compare the general medical status of the groups. In all analyses, we adjusted for the number of days between baseline screening and the follow-up interview.
Data weighting. We used the propensity weighting method (
41 ) to adjust for potential attrition bias (unit nonresponse bias) after the baseline assessment. To the extent that correlates of nonresponse can be identified, the follow-up sample (N=519) was weighted to represent the baseline sample (N=1,156). Nonresponse patterns were examined at four sequential stages: refusal to be recontacted (N=331); absence of a follow-up letter (N=29); inability to locate (N=146); and refusal of the follow-up assessment, poor health status, or death (N=131).
For each of the four stages, we performed the following procedure. A binary logistic regression model was constructed with unit response versus nonresponse as the outcome, and variables from the baseline study were entered as candidate predictors by using stepwise selection criteria (to enter, p=.20; to stay, p=.05) and allowing for up to two-way interactions. At each stage, the weight for each patient was the reciprocal of the probability of the predicted response. Information about the baseline variables that significantly predicted response versus nonresponse at each of the four stages is available upon request.
The weights from each of these four models were multiplied to produce an overall weight for each of the 519 follow-up participants. To minimize undue effects from excessively high or low weights, we performed a quantile split of the overall weights to produce six weighting classes. Each member of a weighting class was assigned the mean weight for that class (
41 ). Final weights ranged from 1.486 to 3.610, and summed to 1,156, the size of the baseline sample. All analyses were weighted and were conducted with SAS, version 9, specifically the SURVEYFREQ, SURVEYMEANS, SURVEYREG, and SURVEYLOGISTIC procedures. The level of significance was set at .05 (two-tailed).