Prevalence rates of bipolar disorder are similar among African Americans, Hispanics, and non-Hispanic whites (
1,
2,
3 ), ranging from 2% to 4% (
3,
4,
5 ). Several studies have reported treatment differences for African Americans, such as fewer psychiatric medications and fewer classes of these medications (
6,
7 ), fewer outpatient visits (
8 ), and higher psychiatric hospitalization rates than for whites (
9 ). A previous study compared baseline demographic, illness, and treatment characteristics of African-American, Hispanic, and non-Hispanic white groups in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) (
10 ). Compared with non-Hispanic whites, African Americans and Hispanics reported fewer medications prescribed and Hispanics had fewer recent specialty care visits, after adjustment for socioeconomic differences. No differences in overall severity of mood symptoms, quality of life, and psychiatric comorbidity were observed, although African Americans' scores on measures of two psychotic symptoms (psychotic thought and insight) indicated greater severity than for the other two groups and comorbidity rates differed between groups (
10 ).
It is not known whether U.S. Hispanics, African Americans, and non-Hispanic whites with bipolar disorder have differential responses to mental health treatments. One clinical trial of haloperidol treatment for acute mania reported higher remission rates for Latinos than for whites and a trend toward higher remission rates with olanzapine for Latinos (
11 ). In any study of race-ethnicity and treatment outcomes, consideration of socioeconomic differences is crucial in interpreting outcomes across race-ethnicity, given the average lower income and education level and higher rates of uninsured among U.S. African Americans and Hispanics compared with non-Hispanic whites (
12 ).
In this study we examined treatment outcomes for the first year in STEP-BD for African Americans, Hispanics, and non-Hispanic whites. Baseline data in STEP-BD indicated that Hispanics and African Americans differed from each other in demographic and cultural characteristics. Thus each group was separately matched to a group of non-Hispanic whites with similar demographic characteristics. Previous analyses of STED-BD data showed that both minority groups reported less intensive treatment. Therefore, we hypothesized that non-Hispanic whites would respond to treatment and recover at higher rates than African Americans and Hispanics in the areas of manic symptoms, depressive symptoms, and overall functioning.
Methods
Overview
Participants were enrolled in STEP-BD, a prospective naturalistic study conducted between November 1999 and November 2004 (
13 ). STEP-BD had a total of 22 U.S. participating sites, 13 of which accounted for over 90% of the enrolled participants (
14 ). Participants from racial-ethnic minority groups were enrolled nationally—African Americans were recruited at 18 of the 22 sites, with no site accounting for more than 25%; 20 sites contributed to the Hispanic sample, with no site accounting for more than 35%.
Patients enrolled for the main STEP-BD study were at least 15 years of age and met
DSM-IV criteria for bipolar I, bipolar II, or bipolar disorder not otherwise specified; cyclothymia; or schizoaffective disorder, bipolar subtype. Patients could enter the study in any clinical state. Exclusion criteria were limited to unwillingness or inability to comply with study assessments, inability to give informed consent, immediate need for detoxification, and inability to speak English. The study was approved by local institutional review boards. Recruitment methods included advertisements and enrollment of existing clinic patients from academic medical centers, most of whom had private or public insurance to pay for STEP-BD treatment. In the second year of STEP-BD, community-based clinics were added as sites. After procedures were fully explained, written informed consent was obtained from all participants. STEP-BD methods are described in more detail elsewhere (
13,
14 ).
Participants in the study reported here were a subset of the 4,107 participants who had either bipolar I or II disorder and who were included in the final STEP-BD data set. African-American participants (N=155) were compared with a group of non-Hispanic white participants (N=729); frequency matching on gender, income, education level, and insurance status (yes or no) was used. Hispanic (N=152) and non-Hispanic white (N=822) participants were matched on the same variables and compared. These four variables were used for matching because the groups differed on these variables at baseline. Age was not included as a matching variable because groups were similar in age. Frequency matching is a commonly used procedure that ensures that both groups have similar distributions (proportions) of key variables (
15 ). Frequency matching improved statistical power because comparisons could be made with a large subgroup of non-Hispanic whites without control for confounding variables in the analyses (
16 ). Frequency matching was selected rather than one-to-one individual matching so that missing data for a participant in one group would not require deletion of similar data from the comparison population.
Participants self-identified their race or ethnicity by choosing one of the following options: white or Caucasian (non-Hispanic white); black or African American; Native American, Eskimo, or Aleut; Asian or Pacific Islander; no primary race; and other. Participants were then asked whether they were of Hispanic or Latino background and also for their country of origin (such as Mexico or Cuba). If participants answered yes to Hispanic or Latino background, they were included in the Hispanic group irrespective of race. Because of small samples, participants in four of the groups were not included in the analyses—Native American, Eskimo, or Aleut; Asian or Pacific Islander; no primary race; and other.
Outcomes and measures
Results are based on assessments conducted during the first year of STEP-BD participation. The Montgomery-Asberg Depression Rating Scale (MADRS) (
17 ) was used to assess depression symptoms, and the Young Mania Rating Scale (YMRS) (
18 ) was used to assess manic symptoms. Clinicians rated patients on the Global Assessment of Functioning (GAF) (
19 ) (0, least functional, to 100, most functional). For clinical status, the Clinical Monitoring Form (CMF) was used (
13 ). Intraclass interrater reliability coefficients for the CMF range from .83 to .99. CMF mood status is based on
DSM-IV criteria for depression, mania-hypomania, and mixed episodes. A CMF score for mania or depression symptoms greater than 3 indicates a subsyndromal state (moderate mood disorder symptoms that do not meet full
DSM-IV criteria for an episode). Recovered status is indicated by a CMF score of less than 2 (moderate symptoms for at least eight weeks). Medications prescribed during the year were not examined. Psychiatrists were certified on these measures and used evidence-based practice procedures throughout the course of the study.
The Mini-International Neuropsychiatric Interview (MINI Plus Version 5.0) (
20 ) was used at baseline to assess current comorbid anxiety disorders (panic disorder, agoraphobia, social phobia, obsessive-compulsive disorder, and posttraumatic stress disorder) and alcohol and drug use disorders (abuse and dependence). The baseline psychiatric assessment included ratings of four psychotic symptoms as present or absent: paranoid ideation, ideas of reference, hallucinations, and delusions. No structured questions or definitions for the four terms were provided. The rating of psychotic symptoms was separate from the symptom ratings on the MADRS, YMRS, and MINI Plus assessments. [A definition of another outcome measure, proportion of days well, and a description of missing and censored data are presented in an online supplement to this article at
ps.psychiatryonline.org .]
Statistical analysis
We compared groups on three outcome measures of treatment response: depression symptoms, manic symptoms, and GAF score. Recovery was measured as attaining recovery status from the index episode (as measured by the CMF) with no subsequent mood episode over the one-year period. Survival analysis was used to compare the time to response and recovery. The YMRS and MADRS outcomes were measured at three, six, nine, and 12 months. For GAF and CMF outcomes, the number of time points differed by the participant's number of psychiatric visits; the average number of visits after baseline for the first year was eight. We used Fisher's exact test to compare the proportion of participants responding to treatment over the one-year period.
Participants were included in the response and recovery analyses if they had baseline data and any outcome data after one year. A participant missing 12-month data but with any outcome data after one year was considered censored (not meeting criteria) at 12 months. A participant who had no data after nine months was not included.
For depression symptoms (MADRS) and manic (YMRS) symptoms, response was defined as a 50% improvement over the baseline score that was maintained through all subsequent time points in the first year. For the GAF, response was defined as a score higher than 60 that was maintained throughout the first year. Because of variation in timing of visits, the one-year point for the final CMF (mood episode) rating ranged between 330 days and 380 days. All patients included in survival analyses were experiencing a clinical mood episode at baseline as determined by the CMF; inclusion was not otherwise restricted by baseline scores on the YMRS, MADRS, or GAF.
Survival analyses were repeated including psychotic symptoms (yes or no) as another independent variable because of the baseline group differences. Logistic regressions with interactions were used to examine any interaction between race-ethnicity and psychotic symptoms. Using multiple CMF clinical status ratings for the entire sample, we employed t tests to compare groups on the proportion of days well over the first year. All statistical analyses were two-tailed, and statistical significance was set at ≤.05. Selection of the comparison groups with frequency matching and the statistical analyses were carried out using SAS, version 8.02.
Results
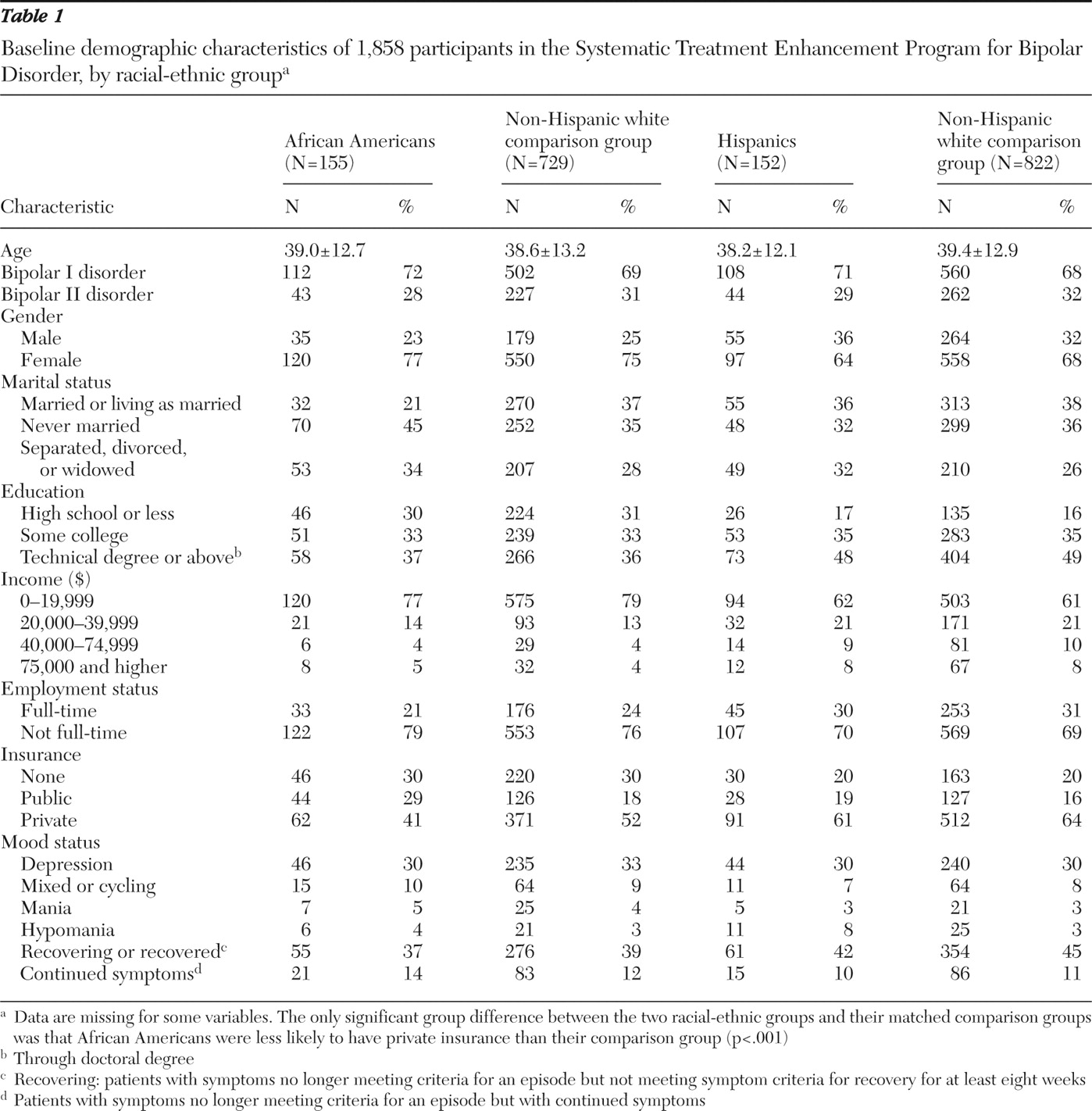
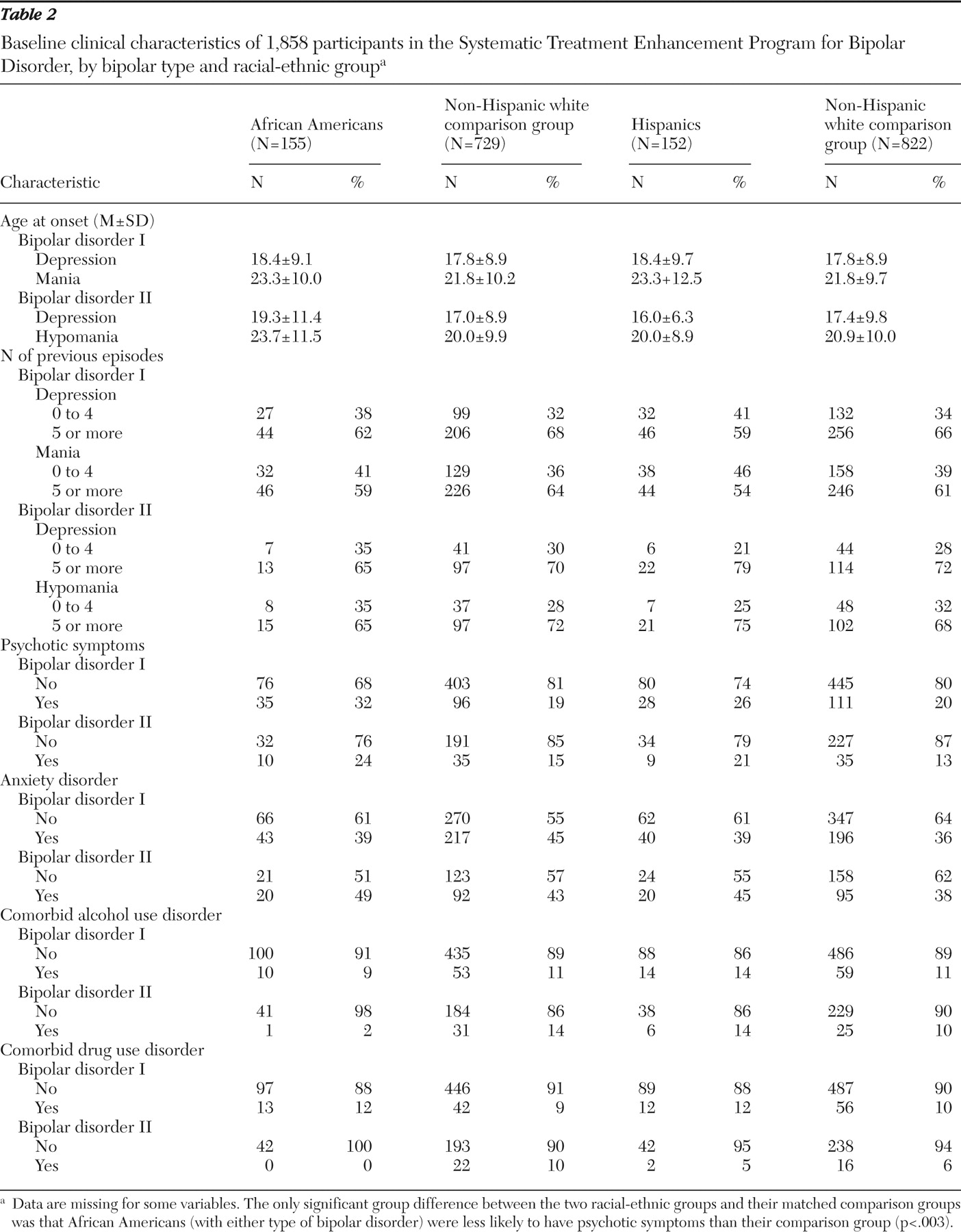
Tables 1 and
2 present data on demographic and illness characteristics. Among the 152 Hispanic participants, 55% (N=83) were Mexican, Mexican American, or Chicano; 14% (N=22) were Puerto Rican; 6% (N=9) were Cuban or Cuban American; and 25% (N=38) were of other Hispanic backgrounds. African-American participants were less likely than their matched comparison group of non-Hispanic white participants to have private insurance and to be married or living as married; they were more likely to have psychotic symptoms at entry (32% versus 19% for bipolar I disorder and 24% versus 15% for bipolar II disorder).
Among the 112 African Americans with bipolar I disorder, 75% (N=84) were female; the percentage of women was 84% (N=36) for those with bipolar II disorder. In the non-Hispanic white comparison group the percentages of women were 72% (N=361) and 82% (N=186), respectively. Among Hispanics with bipolar I disorder, 63% (N=68) were female; the percentage was 66% (N=29) for those with bipolar II disorder. In the non-Hispanic white comparison group, the percentages were 67% (N=373) and 71% (N=185), respectively. Baseline clinical and demographic variables were distributed similarly by bipolar type (I and II) in the racial-ethnic groups. That is, no statistically significant differences in the distribution of gender, psychotic symptoms, anxiety, age, and age at first episode of depression or mania were found by bipolar type for African Americans and their non-Hispanic white comparison group or for Hispanics and their comparison group. Comorbidity of alcohol and drug use disorders was not analyzed because of small cell sizes. [The online supplement includes a table comparing mean baseline scores on the MADRS, YMRS, and GAF for the groups.]
Primary outcomes
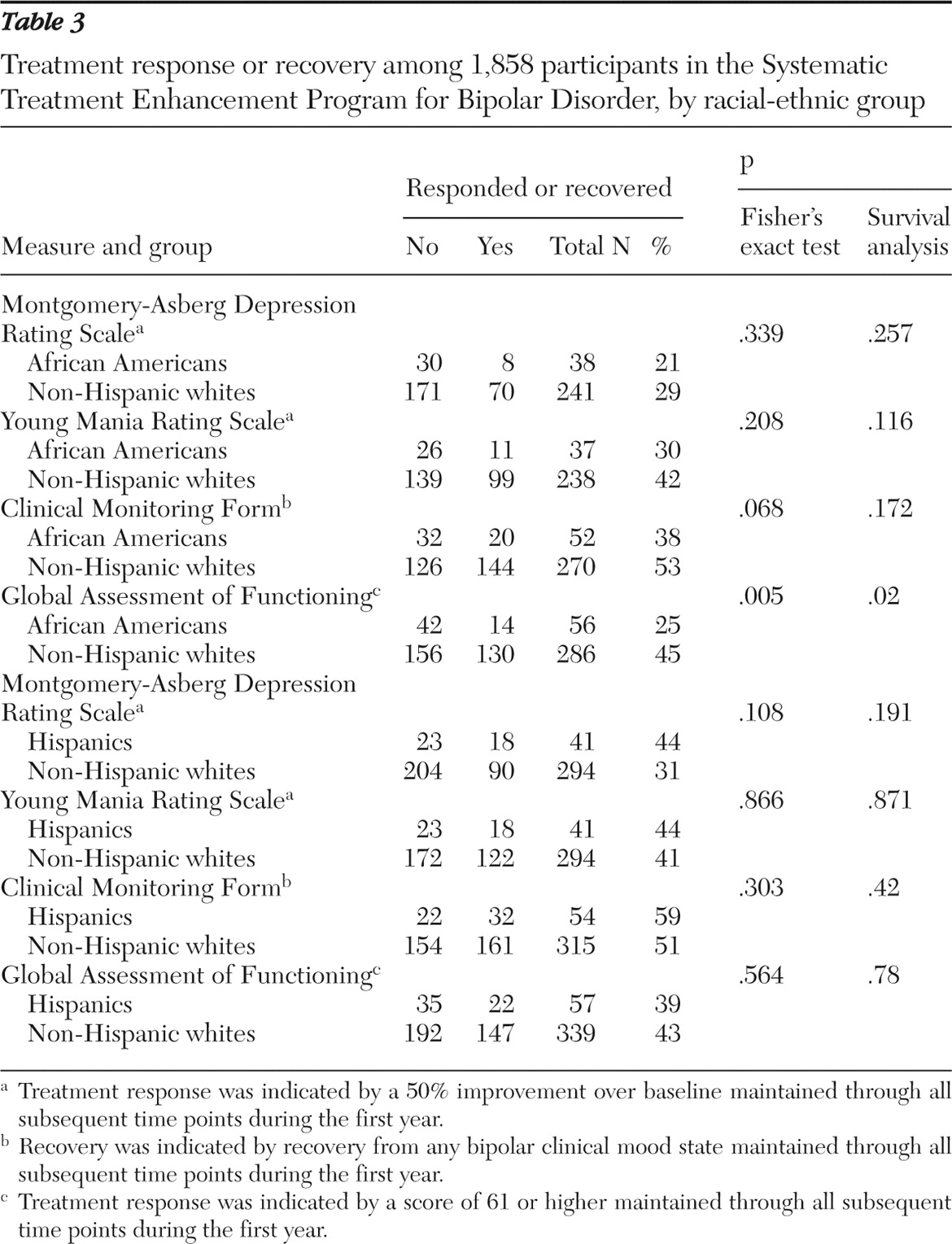
For depression symptoms as measured by the MADRS, none of the comparisons indicated statistically significant differences in either time to 50% improvement or the proportion of participants who responded to treatment (
Table 3 ). For manic symptoms as measured by the YMRS, no significant between-group differences were found in time to 50% improvement or in the proportion who responded. The timing and proportion of patients who recovered from the index mood episode (as measured by the CMF) did not differ significantly between the racial-ethnic minority participants and their respective control groups. However, there was a trend toward a significant difference in recovery rates between African-American patients and their non-Hispanic white counterparts (38% and 53%, respectively; p<.07). African Americans were less likely than non-Hispanic whites to attain and maintain a GAF score greater than 61 (p=.005). The proportion of responders as measured by the GAF was also significantly lower for African Americans than for non-Hispanic whites (25% and 45%; p=.02). Time to response and proportion of responders as measured by the GAF were similar for Hispanic patients and their non-Hispanic white counterparts (
Table 3 ).
When analyses included data for participants regardless of clinical status at study entry (that is, when participants who were not in a clinical mood state at baseline were included), the proportion of days well in the first year was similar for African Americans and their non-Hispanic white counterparts (41% and 45% of days well; p=.25) and for Hispanics and their non-Hispanic white counterparts (44% and 48%, p=.09).
Outcomes by bipolar subtype
We examined whether the proportion of days well in the first year differed between African Americans and Hispanics with bipolar I or II disorder and their respective comparison groups (race-ethnicity × bipolar subtype interaction) (data not shown). The interactions were not significant for comparison of African Americans and their non-Hispanic white counterparts (p=.09) or for Hispanics and their comparison group (p=.20). Thus the associations between race and outcome did not appear to be moderated by bipolar subtype. We also conducted survival analyses to determine whether bipolar subtype was an independent predictor of time to recovery. No differences were found in time to recovery for any of the primary outcomes (YMRS, MADRS, CMF, and GAF, p<.10 for all).
Outcomes by presence of psychotic symptoms
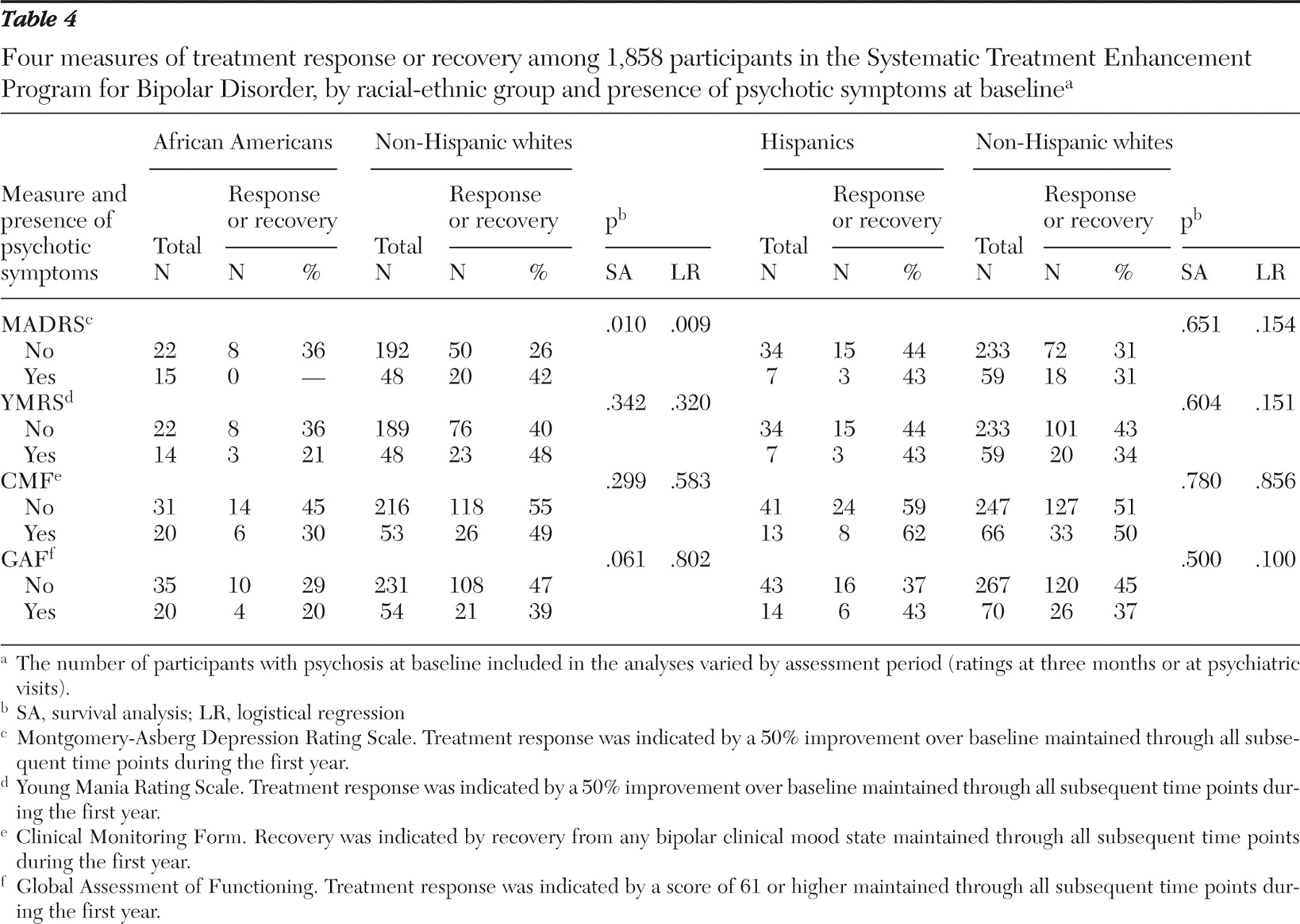
Table 4 shows response and recovery rates by whether participants had psychotic symptoms (yes or no) at baseline. For depression symptoms, a significant difference was found between African Americans and their non-Hispanic white counterparts in time to response (p=.01) and proportion of responders (p=.009) by whether or not they had psychotic symptoms. Among African Americans with psychotic symptoms at baseline, none showed a response in terms of their depression symptoms. In contrast, African Americans without baseline psychotic symptoms had higher response rates than their non-Hispanic white counterparts (
Table 4 ).
For the GAF a similar trend was observed: African Americans with psychotic symptoms at baseline had longer times to response than their white counterparts (p=.06). No interactions between race-ethnicity and psychotic symptoms were found for either minority group for response of manic symptoms or recovery in terms of overall clinical status. No interactions were found for Hispanics and their comparison group.
Discussion
We examined illness outcomes in racial-ethnic groups matched on key socioeconomic factors. Compared with their non-Hispanic white comparison groups, African-American and Hispanic patients with bipolar disorder who received care in STEP-BD experienced similar levels of response in terms of depression (MADRS), mania (YMRS), and proportion of days spent well in the study year. However, African Americans had lower global functioning on the GAF than their white counterparts, a difference that was not seen for Hispanic patients and their comparison group. In addition, a trend toward worse overall clinical status over the study year as measured by the CMF was observed for African Americans compared with their non-Hispanic white counterparts. For depression response as measured by the MADRS, African Americans with psychotic symptoms at baseline had poorer outcomes than non-Hispanic whites with psychotic symptoms at baseline.
It appears that psychotic symptoms in bipolar disorder contribute to poor recovery among African Americans to a greater degree than among non-Hispanic whites or Hispanics. It has often been reported that African Americans have higher rates of schizophrenia diagnoses than mood disorder diagnoses compared with rates reported for non-Hispanic whites (
21,
22,
23,
24 ). In the non-Hispanic white comparison groups in this sample the proportions with psychotic symptoms at baseline (13%–20%) were more similar to the proportions for the entire STEP-BD sample (17%), whereas the proportions of African Americans and Hispanics with psychotic symptoms differed from the proportions in the overall sample. Psychological, social, and biological hypotheses have been proposed for the higher rates of psychosis among immigrant populations of African origin (25); some have suggested that they result from inaccurate symptom assessment or racial biases.
Increased attention to current and previous psychotic symptoms that takes into account an individual's racial-ethnic and socioeconomic background should improve the accuracy of diagnosis and symptom characterization. During STEP-BD clinical assessments, some behaviors of African Americans or their symptom reports may have been misinterpreted as psychopathology instead of being more accurately attributed to sociocultural background. For example, a persecutory delusion might be viewed more accurately as primarily anxiety driven rather than as a psychotic symptom. A clinician may misinterpret depressive symptoms as negative symptoms associated with schizophrenia. What is labeled a "lack of insight" resulting from psychosis might be more accurately seen as a lack of familiarity with illness terminology and with mental health service systems. Some African-American patients' mistrust of mental health providers may be interpreted as paranoia instead of as culturally consistent and perhaps reasonable (
26,
27 ).
A previous study found that African Americans were more likely than whites to endorse schizotypal personality traits on a self-report instrument (
28 ). To better understand the higher rates of psychotic symptoms in bipolar illness among African Americans, it may be useful to include additional measures to help explain outcomes, such as assessing mistrust of health care professionals and experiences of discrimination. Investigators should consider incorporating scales that more comprehensively assess psychotic symptoms and administering such scales along with measures of other symptoms in bipolar disorder. Semistructured rating scales that systematically assess symptoms across ethnic groups are recommended (
29 ). A semistructured approach would also allow for clinical judgment in regard to contextual factors; for example, a clinician could ask additional questions to ascertain whether a patient has interpreted a question as intended (
30 ). The Bipolar Inventory of Symptoms Scale includes structured questions for assessing symptoms, operationally defines levels of severity, and yields a discrete psychosis factor as one of five fundamental domains (
31,
32 ). Alternatively, scales commonly employed for assessing schizophrenia, such as the Brief Psychiatric Rating Scale and the Positive and Negative Syndrome Scale, would be adequate for assessing psychotic symptoms. For both instruments, there is preliminary data on validity for use with persons with schizophrenia from ethnic minority groups (
33,
34,
35 ); however, both have the disadvantage of including numerous items that are uncharacteristic of bipolar disorders.
The results did not support our hypothesis that Hispanic patients would have lower recovery rates. Research on mental health treatment outcomes suggests that when evidence-based practices are applied competently and socioeconomic differences are considered, outcomes are generally similar for Hispanics and non-Hispanics (
36,
37 ). The single published study of medication treatment of bipolar disorder among Latinos, most of whom were non-U.S. Latinos, reported that in some instances Latinos improved at greater rates than whites (
11 ).
Participation by a diverse sample at multiple sites across the United States is a strength of this study. In addition, STEP-BD is the only prospective comparison of outcomes of bipolar disorder among patients from three U.S. racial-ethnic groups. By using frequency-matched groups, we were able to compare African Americans and Hispanics with non-Hispanic whites of similar socioeconomic status, an essential step in comparing outcomes across racial-ethnic groups.
This study has numerous limitations. Because of the demographic characteristics of STEP-BD participants, the generalizability of the results to uninsured persons with bipolar disorder across racial-ethnic groups may be limited. Most participants in our sample had private insurance rather than public insurance, whereas persons with serious mental illness in community samples are likely to have public insurance (
38 ). Although patient groups were matched by insurance status (yes or no), African-American patients were less likely to have private insurance than participants in the comparison group. It is important to note that although we strove to maintain a socioeconomic balance across groups, other differences that may exist between racial-ethnic groups were not addressed in this study. For example, an examination of treatment adherence would provide valuable information because persons from racial-ethnic minority groups often report lower adherence to medication treatment for psychiatric disorders (
39 ). This study did not examine medication treatment. Medication regimens varied depending on psychiatrists' clinical decisions for each patient. Future studies are needed to examine patterns of medication and psychosocial care by racial-ethnic group; if differences are found, studies should assess their impact on outcomes. Several factors that contribute to quality of treatment may have differed by site, particularly at sites with socioeconomic differences, and these factors were not measured in this study. Such factors include provider competence, the extent of community resources, and ease of access to the clinic and to medication. Understanding adherence, quality of treatment, and access to care is an important concern in outcomes studies in which race-ethnicity is examined (
12 ).
The GAF rating includes symptom assessment, and thus generalizability to other quality-of-life outcomes is limited. Psychotic symptoms were not assessed with a validated rating scale. Smaller samples in some subanalyses (
Table 4 ) limited power to detect differences between the groups, and those analyses should be replicated. A similar limitation exists in regard to gender. In this study, about 75% of African-American participants and 65% of Hispanic participants were female. In STEP-BD, 58% of the sample was female, closer to general population estimates. Thus recruitment of persons from racial-ethnic minority groups in STEP-BD was particularly challenging in regard to African-American males. In STEP-BD, current alcohol and drug use comorbidity averaged 10%–15%, whereas in a national study rates of current alcohol and drug comorbidity were 29% and 17%, respectively (
40 ). Thus generalizability of the results to the general population is more limited for males and for persons with comorbid substance use disorders. Analyses of comorbidity and symptom profiles by bipolar type—types I and II—could further elucidate predictors of differential outcomes by race-ethnicity. Study dropout rates were higher in both minority groups than in their comparison groups, and the analyses did not include data from those who dropped out. Thus outcomes are most generalizable to patients who remain in a study and a course of treatment. Finally, focused comparisons of African Americans and Hispanics are recommended to further elucidate racial-ethnic similarities and differences.
Results for Hispanics should be interpreted in the context of the degree of acculturation, which was generally high in STEP-BD (
41 ). Acculturation was not evaluated in the study reported here, although all persons who participated in STEP-BD were required to be fluent in English. Further studies are needed to assess outcomes for Spanish-speaking persons with bipolar disorder in the United States.