Rates of use
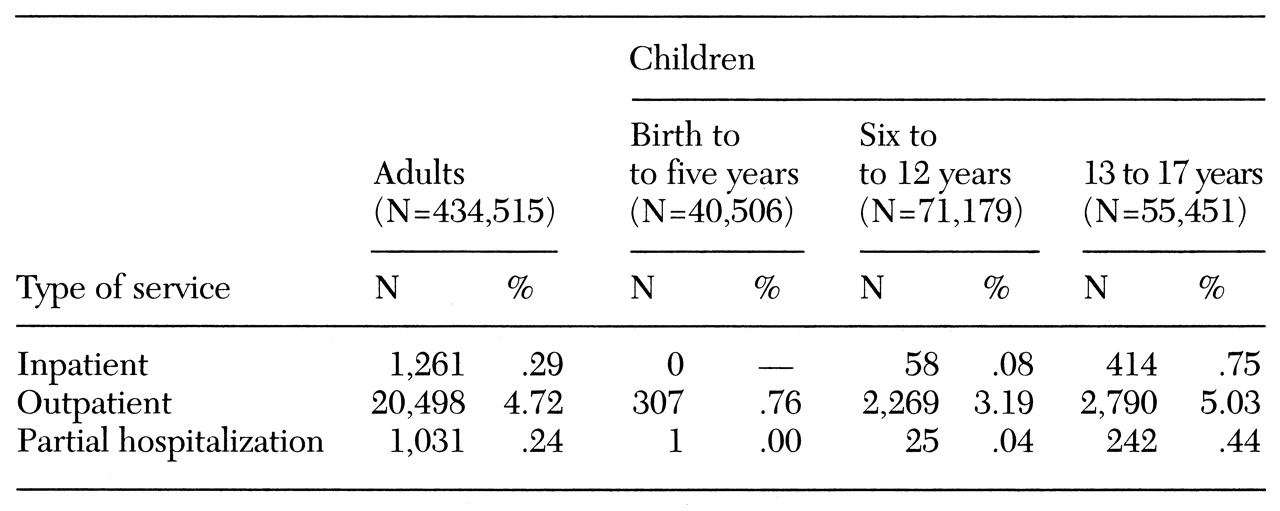
Table 1 reports rates of use of inpatient and outpatient care among adults and among children in the three age groups. The rate of use is the percentage of enrollees who used a service at least once during the one-year period. For example, .29 percent of adults used inpatient services at least once during the year.
Significant differences in use of inpatient services were found across age groups. Adolescents were more than twice as likely as adults to use inpatient services (χ2=301, df=1, p<.001 ) and about seven times as likely as children aged 6 to 12 (χ2=371, df=1, p<.001). Adolescents also had a slightly higher probability (6 percent) of using outpatient care than adults (χ2=10.7, df=1, p<.001), and younger children had lower rates of outpatient use than adolescents or adults (χ2= 276, df=1, p<.001).
Partial hospitalization rates were also higher for adolescents than for adults (χ2=37, df=1, p<.001). Among adolescents, .44 percent used partial hospitalization services, compared with .24 percent of adults. Very few children age 12 and under used partial hospitalization services.
We also investigated whether rates of use varied among adolescents by gender. Although outpatient use rates for male and female adolescents were similar, females were more likely to use inpatient services (χ2=6.4, df=1, p=.012). Among adolescents, .67 percent of boys used inpatient services, compared with .86 percent of girls.
Intensity of use
Children and adults differed in their intensity of service use and in rates of use. The hypothesis that the distribution of non-zero outpatient costs was the same for adults and for all children was rejected (z=12.4, p<.001), as was the hypothesis that the distribution of inpatient costs was the same for both groups (z=8.4, p<.001). When the comparison was limited to adolescents and adults, the same hypotheses were also rejected. Outpatient and inpatient costs differed significantly between adults and children.
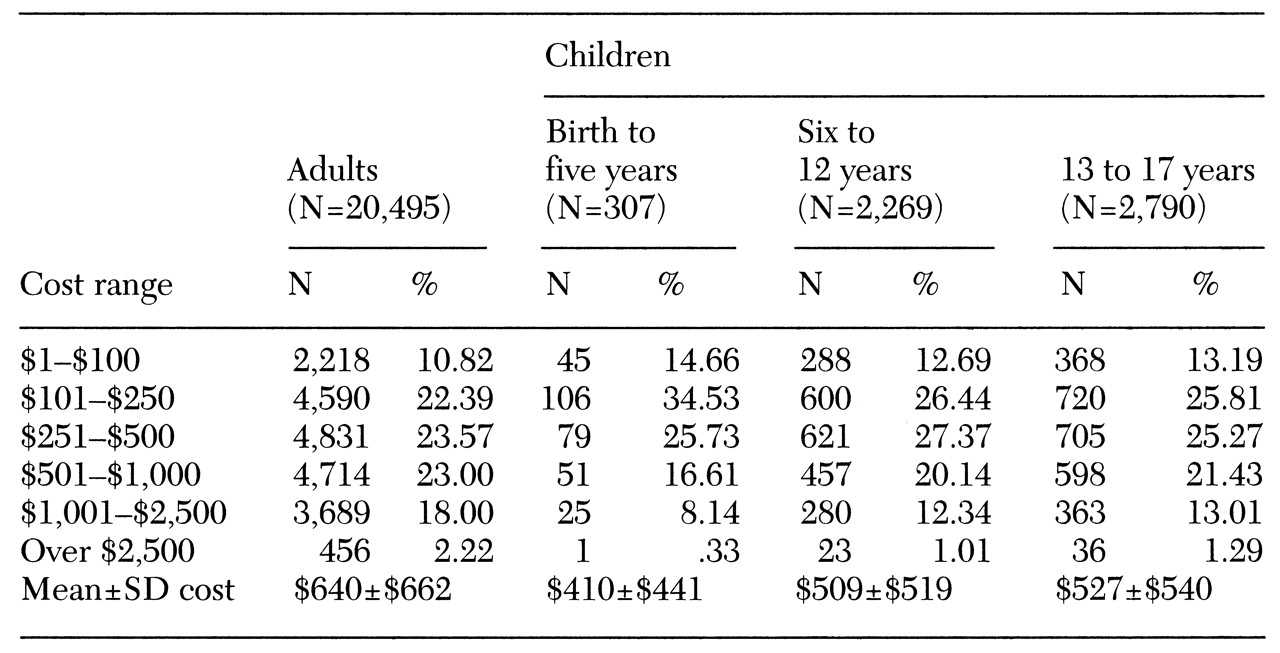
Table 2 reports the different ranges of costs for adults and children of different ages who used outpatient services. For example, 10.8 percent of adults who used outpatient services had total annual outpatient costs between $1 and $100, while 2.2 percent had costs over $2,500. The percentages in each of the columns sum to 100 percent, as data for each user is distributed in only one cost cell.
Children were more likely than adults to have outpatient costs between $1 and $500 (z>5, p<.001) and less likely than adults to have outpatient costs over $500 (3<z<9.5, p<.002). Among adult outpatient users, 43 percent had costs over $500, compared with 25 percent of very young children, 33 percent of children aged 6 to 12, and 36 percent of adolescents. The percentage of adults with outpatient costs over $2,500 was twice the percentage of adolescents (z=3.2, p<.001).
As
Table 2 shows, adults who used outpatient services had an annual mean cost of $640. The mean±SD cost among all children was $513± $526. Very young children had somewhat lower costs than other children. The mean annual cost of outpatient services among children from birth to age five who used these services was $410, compared with $509 and $527 for children aged seven to 12 and 13 to 17, respectively.
The distributions of outpatient costs among adolescents significantly differed by gender (z=1.8, p=.08). Females had a greater probability of having costs of outpatient care over $2,500 (z=1.7, p=.09) and a 22 percent lower probability of costs less than $100 (z=2, p=.04).
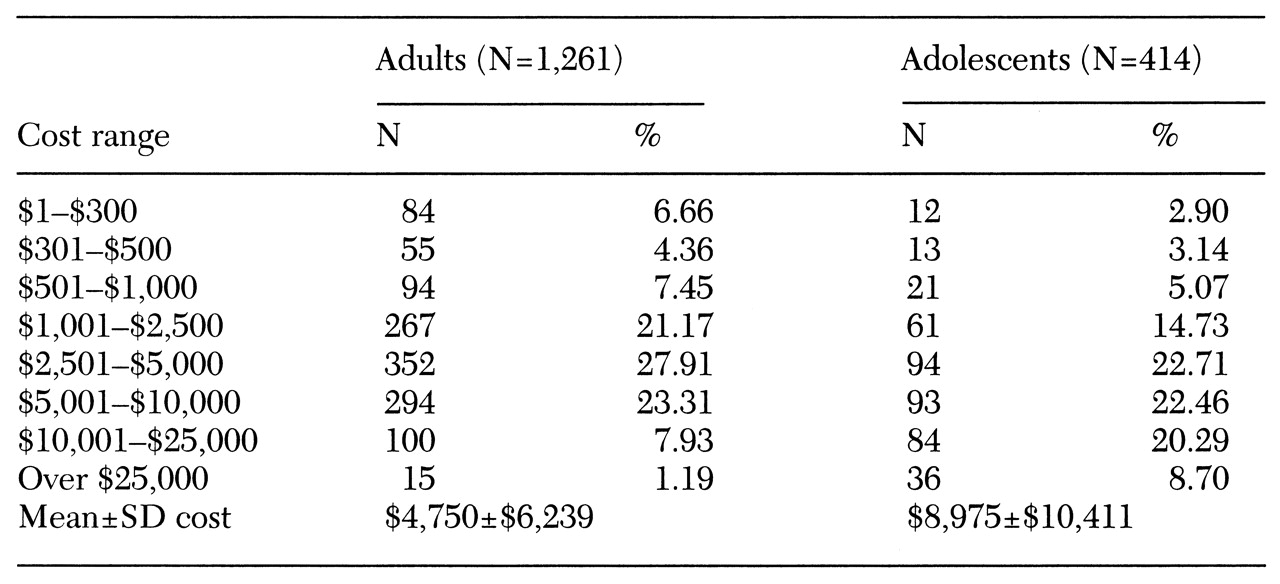
Table 3 shows the distributions of inpatient costs for adults and adolescents among users of inpatient services. Children younger than 13 were excluded because of the low rate of use in this group. The differences in inpatient costs for adults and adolescents are striking: adolescents were significantly less likely than adults to have inpatient costs lower than $5,000 and much more likely to have inpatient costs over $10,000. At almost every cost level below $5,000, children were underrepresented compared with adults (1.7<z<2.9, p<=.09). At the two cost levels above $10,000, children were overrepresented compared with adults (z=7, p<.001, for the next highest level and z=7.7, p<.001, for the highest cost level).
The percentage of adolescents with costs between $10,000 and $25,000 was two and a half times higher than the percentage of adults at this cost level. The percentage of adolescents with costs over $25,000 was seven times higher than the percentage of adults. Among adults who used inpatient services, the mean annual cost was $4,750, more than $4,000 less than the mean cost among adolescent users of inpatient services.
No statistically significant differences were found in partial hospitalization costs for children and adults. Overall, 33 percent of users of partial hospitalization services (30 percent of adolescents and 33 percent of adults) had costs less than $1,000, while less than 10 percent of users (8 percent of adults and 10 percent of adolescents) had costs over $5,000.