Antipsychotic medications are commonly prescribed to treat a variety of psychiatric disorders and symptoms among children and adolescents, although the manufacturers of these drugs have generally tested and marketed them for the treatment of psychotic disorders such as schizophrenia among adults. Studies have suggested that conventional antipsychotics are likewise effective for the treatment of schizophrenia in children and adolescents (
1,
2). However, as psychosis is rare in children and adolescents, these drugs are more often used to treat nonpsychotic phenomena such as aggression (
3,
4), hyperactivity (
5), Tourette's disorder (
6), and pervasive developmental disorder (
7,
8,
9,
10,
11). Moreover, Zito and associates (
12) found that antipsychotics were the most commonly prescribed class of drugs for children and adolescents treated as psychiatric inpatients and that the drugs were prescribed for disorders other than schizophrenia.
In 1989 the novel ("atypical") antipsychotic clozapine was marketed for the treatment of schizophrenia. Clozapine is unlike the conventional ("typical") antipsychotics in several ways, including its low incidence of extrapyramidal symptoms and its ability to blockade not only the D2 receptor but also the HT2 receptor. Clozapine's potential advantages over conventional antipsychotics include its usefulness for treatment-resistant schizophrenia. In addition, its use is rarely associated with the development of dyskinesias. Unfortunately, use of clozapine is associated with a higher than usual risk of agranulocytosis, which can be lethal.
Newer antipsychotics that are similar to clozapine in some ways have been marketed recently. They include risperidone, olanzapine, and quetiapine, all of which, like clozapine, are referred to as novel or atypical antipsychotics. Because they have a lower incidence of extrapyramidal symptoms, including an implied lower propensity for causing dyskinesia, they are prescribed to children and adolescents. However, industry-sponsored trials for these agents, as for most psychotropics, have generally excluded children and adolescents.
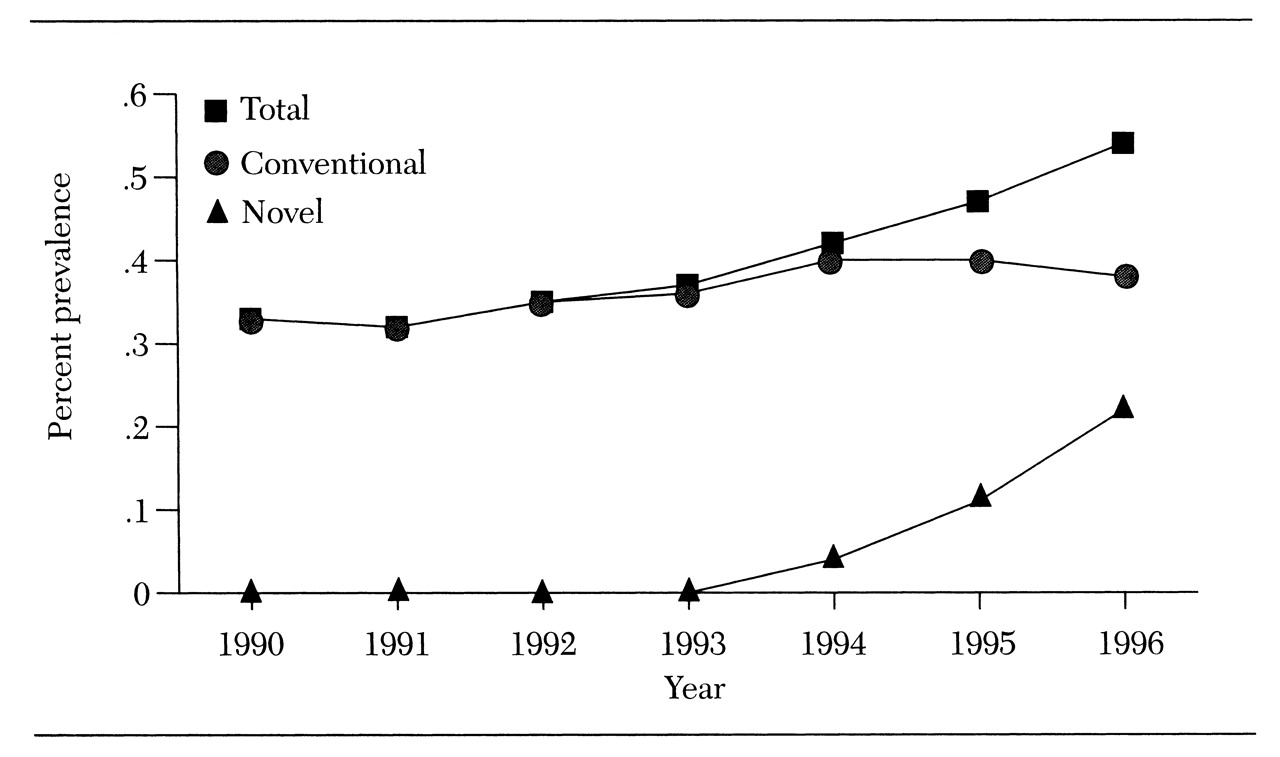
This column gives an overview of the evidence for the use of these agents in treating children and adolescents. Such an overview is timely because the administration of antipsychotics to children and adolescents is on the rise. For example, as
Figure 1 shows, among children and adolescents from a large Midwestern Medicaid population, usage increased by as much as a 63 percent between 1990 and 1996, due primarily to prescription of the novel antipsychotics (Zito JM, Safer D, Gardner J, unpublished data, 1998). Clozapine and risperidone were available during the period shown in the figure, but olanzapine and quetiapine were not yet available.
Clozapine
Clozapine, a dibenzodiazepine, was approved for use in the U.S. in 1989, the first novel antipsychotic to be approved for use in this country. Clozapine was found to be effective in addressing treatment-resistant schizophrenia among adults (
13). However, patients who are prescribed clozapine must have weekly blood monitoring because use of the drug carries the risk of life-threatening agranulocytosis.
Studies of the use of clozapine with children and adolescents have been reported. Kumra and associates (
14) investigated the safety and efficacy of clozapine for treating childhood-onset schizophrenia by comparing clozapine to haloperidol in a randomized double-blind study. The subjects ranged in age from six to 18 years and had a history of poor response to antipsychotics. Clozapine at doses ranging from 25 to 525 mg per day (mean±SD dose=176±149 mg) was found to be more effective than haloperidol at doses ranging from 7 to 27 mg per day (mean±SD dose=16±8 mg). Clozapine was found to be particularly effective in treating negative symptoms.
The doses of haloperidol used in this study were higher than those used in other controlled trials of its effects in treating childhood-onset schizophrenia (
2) and in treating children with autism (
10), and the higher doses may have increased the ratings of negative symptoms among subjects who received haloperidol. A third of the subjects in the clozapine group experienced side effects, which included neutropenia and seizures. A number of other side effects, including excessive weight gain, have been noted with use of clozapine (
15).
A controlled clinical trial comparing the safety and efficacy of clozapine, olanzapine, and placebo for the treatment of childhood-onset schizophrenia is under way (
16). Results of open trials of clozapine for adolescents with childhood-onset schizophrenia (
17,
18) and case reports of its use for this group of patients (
19,
20,
21) have been published.
In summary, although clozapine shows promise in the treatment of childhood-onset schizophrenia, it is likely to be a treatment of last resort because of the risk of serious side effects such as neutropenia and seizures, and the need for frequent blood monitoring.
Risperidone
Risperidone, a benzisoxole derivative, was introduced to the market in 1993. To date no controlled trials of the use of risperidone for treatment of children and adolescents have been reported, although the literature includes reports on open trials and case studies.
Armenteros and associates (
22) reported on the short-term efficacy and safety of risperidone in an open trial involving ten adolescents with a diagnosis of schizophrenia. Risperidone was administered twice a day in doses that ranged from 4 to 10 mg per day (mean=6.6 mg per day). The investigators found that risperidone was efficacious but that its use was associated with weight gain, sedation, and extrapyramidal symptoms including acute dystonic reactions. Currently, Armenteros is conducting a double-blind and placebo-controlled study of risperidone for adolescents with schizophrenia. Several case reports and a retrospective chart review describe the use of risperidone in treatment of schizophrenia or psychosis (
23,
24,
25,
26,
27,
28).
Risperidone has been used to treat pervasive developmental disorder in small open trials (
29,
30,
31,
32), and a few case reports have described this use (
33,
34). Controlled trials of this drug for pervasive developmental disorder, as for schizophrenia, have been conducted with only adult subjects (
35).
The only reports of the use of risperidone in treatment of Tourette's disorder have been descriptions of open trials (
36) and a retrospective chart review (
37), although the findings suggest that the drug is efficacious. The most common side effect reported was weight gain. It is important to note that dyskinesias related to risperidone have been reported among children and adolescents (31, 38), and cases of hepatotoxicity have also been reported (
39).
In summary, risperidone has not been studied systematically and critically for use among children and adolescents, although such studies are under way. However, the reports to date are encouraging and suggest that risperidone may be useful for treating some children and adolescents.
Olanzapine
Olanzapine is an novel thienobenzodiazepine introduced to the market in 1996. No controlled trials of olanzapine in treatment of children and adolescents have been reported, although, as mentioned above, a controlled trial comparing clozapine, olanzapine, and placebo for childhood-onset schizophrenia is under way. Kumra and colleagues (
16) reported on an open trial in which olanzapine was effective for symptoms of childhood-onset schizophrenia. In this study eight subjects aged ten to 17 years were treated with olanzapine in doses ranging from 12.5 to 20 mg per day (mean±SD dose=17.5±2.3 mg). The main side effects were increased appetite, constipation, nausea or vomiting, headache, somnolence, insomnia, difficulty concentrating, sustained tachycardia, transient elevation of liver transaminase levels, and increased agitation. During the trial period, abnormal movements and extrapyramidal symptoms were minimal.
The remainder of the literature on olanzapine consists of case reports of its use in treatment of Tourette's disorder (
40), pervasive developmental disorder (
30), and mental retardation (
41). Controlled studies of this novel antipsychotic in the treatment of children and adolescents are needed.
Quetiapine
Quetiapine fumarate is a novel dibenzothiazepine (
42) first marketed in 1997. There are no published controlled trials examining its use in the treatment of children and adolescents. McConville and associates (
43) reported results from an open-label study of the pharmacokinetics and tolerability of this agent among ten adolescents with psychotic disorders who were between ages 12 and 17. Subjects received the drug twice a day for 21 days, and doses were increased in a stepwise fashion to 100 mg per day and then to 400 mg per day. The results suggested that quetiapine may be tolerable in short-term usage and may hold promise as a treatment for this population.
In some animal studies, quetiapine was found to be associated with the development of cataracts. Although no clear evidence suggests that lens changes will occur in humans, the possibility cannot be ruled out. The manufacturer recommends that patients' lenses should be examined for signs of cataracts before beginning the drug and at six-month intervals while on the drug (
44). Again, controlled studies of this novel antipsychotic involving children and adolescents are lacking.
Discussion
The novel antipsychotics show promise in the treatment of some psychiatric disorders among children and adolescents. However, the promise may be related more to the novel agents' similarities to the conventional antipsychotics, for which we have more data and experience, than to the limited data on the novel agents themselves. Although controlled trials of the novel antipsychotics are being conducted, few such studies have been completed.
The lack of controlled trials is not surprising—with the exception of stimulants, few psychoactive agents have been tested in controlled clinical drug trials involving children and adolescents (
45). The lack of controlled trials is of particular concern when one considers the high rate of psychotherapeutic drug treatment among children and adolescents (
46,
12), especially in light of the sociological issues and controversy surrounding the use of these agents for the young (
47). Furthermore, psychotropic medications are administered clinically to children and adolescents, often for prolonged periods of time. From the data available, it is difficult to assess the effects that the novel antipsychotics will have on learning and cognition, areas of importance in developing children and adolescents.
Because these drugs are likely to be used for the long term, it is important to investigate the risk of dyskinesias among children and adolescents. It should not be forgotten that the conventional antipsychotics were used for several years before drug-related dyskinesias were described. In a prospective study of haloperidol in treatment of children with autism, dyskinesias were found to occur. This finding led to the recommendation that the drug be withdrawn periodically to assess the need for its continued use and to observe for withdrawal dyskinesias, which may be an early form of tardive dyskinesia (
10). This recommendation should also apply to the novel antipsychotics, particularly as data on their long-term use among children and adolescents are lacking.
Perhaps of greater concern is the potential effect these drugs may have on weight gain. Weight gain is a risk factor for many health conditions, including cardiovascular diseases and diabetes (
48), and can affect patients' self-esteem and their willingness to comply with treatment.
Unlike the conventional antipsychotics, the novel agents, apart from risperidone, generally do not cause increases in prolactin. By increasing prolactin, conventional antipsychotics may cause amenorrhea and thereby decrease the fertility of female patients. Thus, when female patients are switched from conventional to novel agents, the possibility of pregnancy may be increased.
Conclusions
Very few systematic studies of the novel antipsychotics in the treatment of children and adolescents have been done. Many psychopharmacologists say that the conventional antipsychotics play a reduced role in modern treatment of adults. Although conventional antipsychotics may also eventually play less of a role in the treatment of some diagnoses among children and adolescents, we need more data before such a conclusion can be drawn. It is understandable that those who thoughtfully treat children and adolescents often prescribe drugs that have not been labeled or studied for use in this population. However, more efforts to systematically study the effects of the novel antipsychotics among children and adolescents are crucial, particularly as evidence suggests an increase in clinical usage.
Acknowledgment
This work was partly supported by grant MH-00979 from the U.S. Public Health Service to Dr. Malone.