By 1990 mental health organizations began to recognize the benefits of empowerment for persons with psychiatric disabilities. As a result, 22 state mental health agencies currently have policies promoting consumer empowerment (
1). However, little systematic research has used empowerment as a mental health outcome measure.
In a recent study, Rogers and associates (
2) set out to "further define and operationalize the construct of personal empowerment from the perspective of consumers, survivors, and former patients and to construct and validate a scale that can be used in a variety of settings." The result of their work is the 28-item Empowerment Scale (
2). Analysis of data collected with the Empowerment Scale demonstrated five factors—esteem, power, activism, control, and anger.
Rogers and colleagues found that characteristics of respondents such as race, gender, and marital status were not significant predictors of empowerment. Their sample included participants from six consumer-operated programs, one in each of six states. Additional testing of the Empowerment Scale included an inpatient population and a sample of college students (
3,
4), but the authors of the instrument stressed that further testing is needed to determine the scale's ability to measure differences among known populations.
If the Empowerment Scale is intended to be used in a variety of settings, clearly one area of greatest potential use is in adult outpatient programs operated by mental health agencies. To date, the Empowerment Scale has not been examined with a large diverse state mental health population. The purpose of this study was to confirm the psychometric properties of the instrument and define predictors of empowerment by distributing the Empowerment Scale to an entire state mental health system via a mass mailing.
Methods
Participants
Two thousand outpatients age 18 years and older were randomly selected from a centralized database of all clients receiving publicly funded mental health services in South Carolina. Sampling criteria limited inclusion to consumers with at least five contacts with a community mental health center during a four-month period (August 1997 through November 1997).
Survey packets were mailed to the 2,000 clients in a mass mailing. A one-page letter was sent one week before the survey packet to inform consumers why completing the survey was beneficial for quality improvement in the mental health system. The letter reassured them that responses to the survey would remain confidential. Participation was encouraged, and consumers were informed that failing to respond would not affect them in any way. The survey packet included the four-page survey, a one-page demographic sheet, and a return envelope.
A total of 283 completed surveys were returned, for a response rate of 16.5 percent. Coincidentally, another 283 surveys were returned unopened due to incorrect addresses.
The 283 completed surveys reflected the state mental health population in gender, race, age, and employment (
5). A total of 190 respondents were female (67 percent), 178 were Caucasian (64 percent), 191 were unemployed (69 percent), and 175 were between the ages of 36 and 55 years (62 percent). Respondents had more educational experience than the general state mental health population.
Demographic variables were dummy coded to allow for descriptive statistics and more sophisticated analyses. Correlations and reliability analyses were used to test the internal consistency of the empowerment subscales. Stepwise multiple regression of demographic variables was conducted to determine predictors of empowerment. Finally, a factor analysis was conducted to confirm the original factor structure of the instrument developed by Rogers and colleagues.
Results
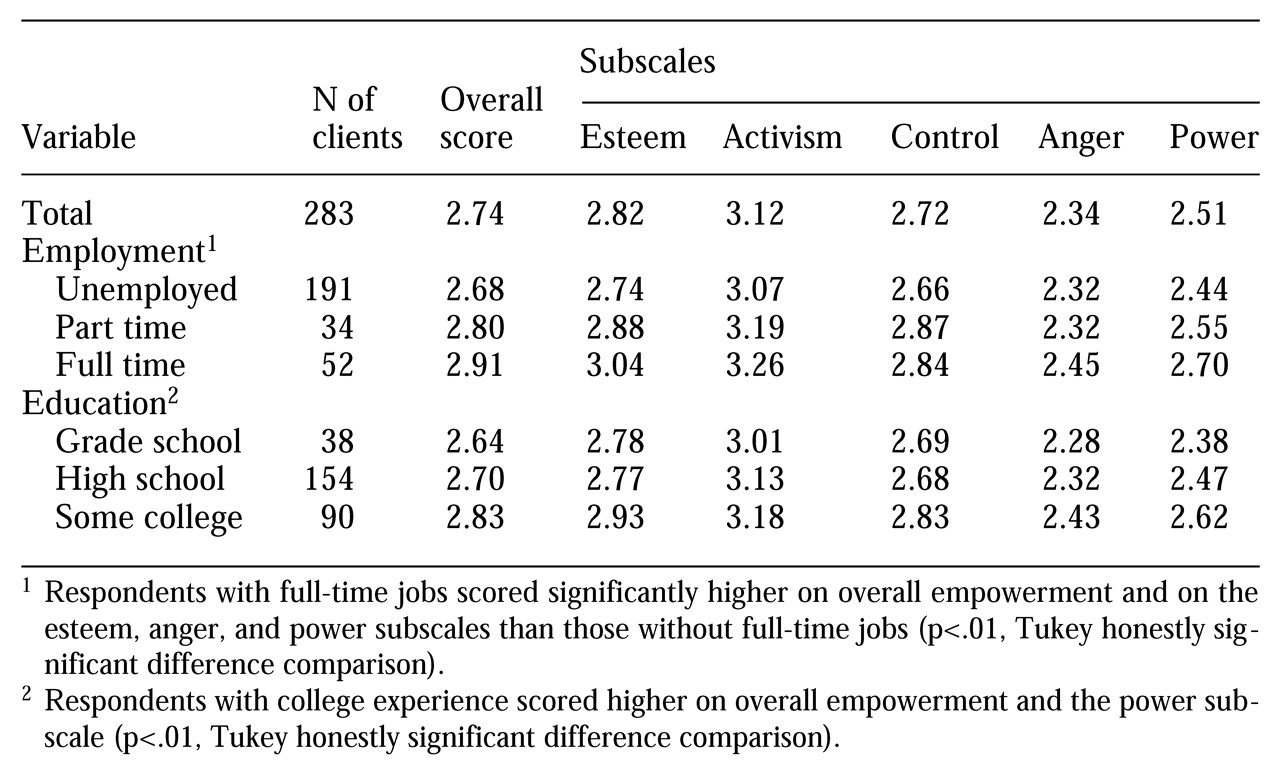
An overall empowerment score for each respondent was obtained by summing the scores of individual items and dividing by the total number of items. The overall mean score for the sample was above the midpoint for the instrument. Out of a possible score of 4, which indicates a high level of empowerment, the mean±SD score was 2.74±.34, which is somewhat lower than the mean score of 2.94±.32 in the Rogers study.
For our sample, the Cronbach's alpha for the instrument suggested a high internal consistency (alpha=.85, N=264), which parallels that in the Rogers study (alpha=.86, N=261). In our study, Cronbach's alphas for the five subscales were .91 for esteem, .67 for activism, .66 for control, .60 for anger, and .55 for power.
Analysis of variance indicated a significant difference between groups on overall empowerment by employment status (F=10.39, df=2,274, p<.001) and education level (F=6.21, df=2,279, p=.002). In the stepwise multiple regression, race, gender, and age did not predict empowerment scores. As shown in
Table 1, respondents with full-time jobs scored significantly higher on overall empowerment and three of the five factor subscales. Respondents with a college education or some college experience scored higher on overall empowerment. Education level was associated with higher scores on the power factor.
Eight of ten correlations between the empowerment subscales were significant (p<.05). Finally, a principal components analysis with an orthogonal (varimax) rotation confirmed the empowerment subscales delineated in the study by Rogers and colleagues. The eigenvalues were 5.37 for esteem, 2.01 for power, 2.38 for activism, 1.99 for control, and 1.94 for anger.
Discussion and conclusions
An increasing number of studies have consistently demonstrated that the Empowerment Scale has a high internal consistency and stable factor structure. Rogers and colleagues (
2) asserted that empowerment is an "equal opportunity" construct, with no delineations by demographic variables. However, it has been noted that empowerment is predicated on "having access to information and resources . . . [and] learning skills that the individual defines as important" (
5). The study reported here differs from previous research by suggesting that education level and employment status predict levels of empowerment in the outpatient consumer population. Either our measure of empowerment needs refinement, or education and employment, which are key quality-of-life outcomes, relate closely to the empowerment social agenda (
6).
To shed more light on this matter, a longitudinal examination of participants in vocational rehabilitation programs using the Empowerment Scale could be undertaken. Another avenue of inquiry could focus on whether consumer empowerment is fostered by involving consumers in all levels of policy decisions and service delivery (
1,
7). The Empowerment Scale also could be tested with consumers employed in key positions of mental health systems. Clearly, further examination of employment status and perception of personal empowerment is warranted.
A central concern in this study is the low response rate of 16.5 percent, which may bias the results and limit the generalizability of our findings. Our data collection methods could not account for the potential data lost by those who chose not to respond. On the other hand, to cast as wide a net as possible, a mass mailing was the only fiscally responsible option.
It was assumed that the dataset represents an entire state population of adult outpatient clients based on random selection of respondents statewide with five or more visits. The final sample of 283 clients is larger than the sample in the study by Rogers and colleagues (
2). However, the low response rate and the elevated level of education among respondents suggest that education and employment should not be assumed to be predictors of empowerment without further controlled tests.
In the continuing push toward managed behavioral health care and accountability, mental health organizations will increasingly require valid self-report measures of program outcomes. The Empowerment Scale taps into the current concerns of mental health consumers and their families, and continued demonstrations of its validity should help it gain strength and popularity as a feedback mechanism to promote positive changes in the mental health system.