Little research has been conducted on constant observation (
1,
2). Except for our pilot study, which explored 14 suicidal inpatients' experiences of being constantly observed (
3), we are aware of no studies that have elicited inpatients' participation in determining whether therapeutic effects other than physical protection occur during constant observation. This study expands on our previous findings, identifies additional therapeutic effects, and reports on inpatients' perceptions of which specific aspects of constant observation are therapeutic.
Methods
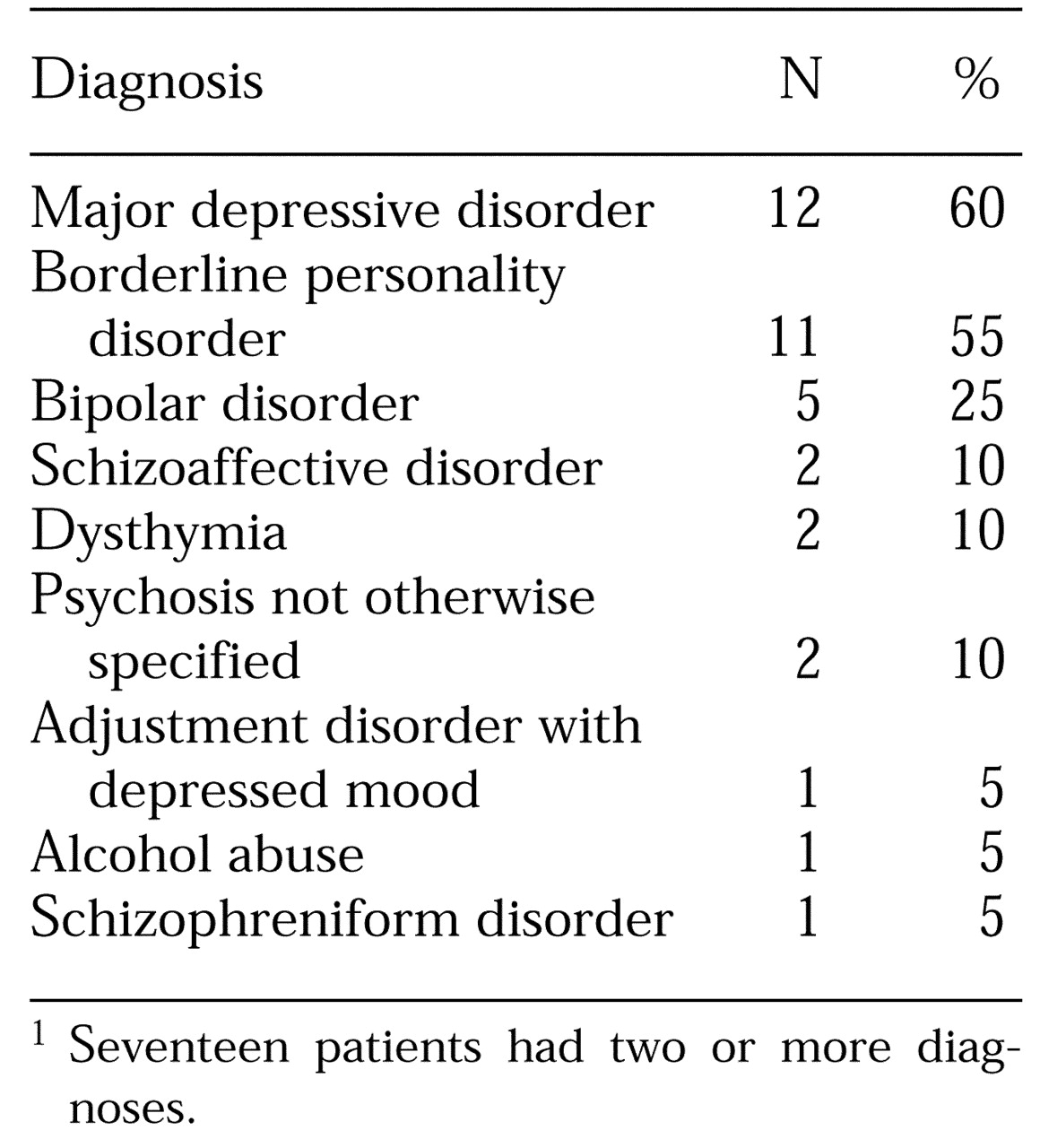
The sample consisted of 20 suicidal adult inpatients—seven men and 13 women—who had been placed under constant observation within two weeks before being interviewed for the study in November 1996. The participants, whose mean age was 32, were selected nonrandomly from three psychiatric facilities. Twelve were patients at a state-owned psychiatric institution, and eight were patients at one of two general medical centers with psychiatric inpatient units. Participants' psychiatric diagnoses were based on
DSM-IV criteria (
4). The diagnoses varied (
4) and are shown in
Table 1.
The individuals who provided constant observation were 13 hospital staff members, including registered nurses and mental health technicians, and seven minimally trained lay workers or sitters. The duration of the episodes of constant observation ranged from four hours to six days, with a mean of 48 hours.
Twelve participants had previous experience of constant observation, ten during past hospitalizations. For 14 participants, constant observation was implemented at the time of admission, for two it was implemented a few days following admission, and for four participants constant observation did not occur until months following their admission.
Information about the inpatients' experiences of constant observation was gathered through qualitative research methods based on extensive in-depth interviews. Each participant was interviewed at least twice. Further interviews were conducted for clarification and depth. A total of 47 interviews were conducted with the 20 participants, and 44 were audiotaped. The interviews of three patients who refused to be audiotaped were recorded in writing, and additional demographic information was collected from the charts. Themes were identified and validated by both authors and one outside expert in qualitative research. Analysis was consistent with Hutchinson's recommended management (
5) of grounded theory data.
Results
The participants identified both therapeutic and nontherapeutic aspects of constant observation. Therapeutic effects were defined as those leading to improvement in symptoms or a higher level of well-being. They fell into two categories—those related to observers' attitudes or behaviors, which were labeled observer interventions, and those unrelated to the observer, labeled extraneous factors. During the interviews the participants primarily focused on observer interventions.
Observer interventions
Thirteen of the 20 participants emphatically expressed positive feelings toward the observers, particularly when they perceived them as friendly and willing to help. One participant spoke about the importance of observers' support: "They are 100 percent important. Because you don't have the family. You don't have the support during the hospitalization. You don't have any close ties. . . . So they are your support. And if you don't have that, you are going to suicide. It's frightening being over the hump and looking back knowing that was what it was going to depend on."
The participants perceived both therapeutic and nontherapeutic interventions from the observers. Therapeutic interventions included the observers' optimistic attitude, acknowledgment of the patient, distraction of the patient from thoughts of suicide, emotional support, and protection.
Optimism.
All 20 participants stressed the importance of the observer's positive attitude. Observers perceived as optimistic were described as caring, helpful, and hopeful. The participants noted that observers' optimistic attitudes stimulated problem solving and induced a hopeful attitude as well as a positive self-concept. One participant said, "After a while, wow, I guess there's really something about killing myself that might not be such a good idea, since all these people seem to think that it's worth making an incredible effort to make me not do it. You internalize what they think."
Acknowledgment.
All 20 participants said that they believed observers' acknowledgment or recognition of them as unique and meaningful human beings was fundamental to the development of a helpful therapeutic relationship with the observer. Observers' behaviors that demonstrated acknowledgment included the use of basic social rules, such as greeting the participant, introducing themselves, showing empathic acknowledgment of emotions, demonstrating respect, and showing interest in the patients' well-being. As one participant put it, "I think having somebody speak to you makes a more positive experience. I mean a million times more positive. It's beyond qualification how important it is. Just come in and talk to you."
Nine participants reported that their dysphoria decreased as a result of observers' acknowledgment, five described feeling less lonely, four reported reduced anxiety, and five stated that their feelings of well-being increased.
Distraction.
Seventeen participants noted that the distractions provided by an observer were highly therapeutic. They identified such distracting activities as engaging in crafts, playing cards, listening to or playing music, taking walks, playing sports, and engaging in social talk. "In my opinion," one participant said, "distraction is the most important, especially when someone is thinking about suicide, because it puts their mind on other things. It takes their mind away from the issue of suicide and you have less time to think about it."
As a result of the distracting activities, five participants reported fewer negative thoughts, decreased anxiety and dysphoria, and a renewed sense of normalcy. In addition, 12 participants described a temporary interruption of suicidal impulses; they noted that if these impulses returned, they were less intense. The participants distinguished between passive distractors, such as listening to music, and active distractors, such playing cards or sports, and called the latter more therapeutic.
Emotional support.
Sixteen participants perceived observers' supportive interventions as beneficial. Such interventions were described as encouragement and support in expressing feelings and in problem solving. Ten participants noted that observers' encouraging behavior and affirmations of participants' self-worth were helpful in increasing their self-esteem, exploring new options, and instilling hope. One participant said, "You know, it is simple compassion. When you feel that someone is there, it means a lot . . . . It's like someone cares."
Ten participants reported that as a result of observers' emotional support, they experienced a decrease in suicidality.
Protection.
All 20 participants acknowledged that constant observation was instituted for their protection. However, seven specifically emphasized this therapeutic benefit. One called it the essential part of constant observation: "The essential part is knowing there is protection there, you know. I feel safer from my impulses." The seven participants perceived themselves as powerless over strong suicidal impulses; three experienced command hallucinations related to suicide. The physical presence of the observer produced feelings of relief by allowing participants to no longer fear their inability to preserve internal control. Four participants believed that the protective aspect of constant observation literally saved their lives.
Eight participants reported that they closely watched the observers' actions at the same time that they were searching for available means to attempt suicide. Among the means they identified were several objects useful for hanging, as well as plastic bags and ledges high enough from which to "jump and smash my head against the floor." However, the participants concluded that due to the constant vigilant presence of the observer and the limited availability of these means, such attempts would prove futile. In their view, the protective environment allowed time for other therapeutic interventions to take place, which altered their dysphoria or suicidal ideation.
Nontherapeutic observer interventions
The participants experienced uncomfortable and at times distressing feelings related to observers' attitudes or behavior, such as lack of empathy, a lack of acknowledgment, failure to provide information about constant observation and the role of observers, or observers' physical presence, such as a lack of privacy or personal space and a feeling of confinement.
Lack of empathy.
Eleven participants perceived some observers to be unempathetic or remote. Behaviors seen as showing a lack of empathy included not responding to the participant's initiation of a conversation and perceived hostile facial expressions. The participants reported that these behaviors were not only unhelpful but also deleterious to their self-esteem. One participant stated, "They don't care. You get that feeling quite often. It just kind of supports that hopeless kind of feeling that life isn't worth living and nobody cares about anything." Such encounters did little to alleviate hopelessness, and six participants noted that they increased their anxiety or aggravated their dysphoria.
Lack of acknowledgment.
Eleven participants described behaviors that they perceived as a lack of acknowledgment from observers; these perceptions sometimes overlapped with perceptions of a lack of empathy. Such behaviors included observers' reading books, appearing distracted or uninterested in the participant, and acting like the participant was a burden. "At times you get the feeling that you are not even here," a participant said. "Like, you are walking in space and nobody sees you, acknowledges your existence. And that is not helpful." Nine participants reported that the perceived behaviors promoted anger, and five said they experienced increased anxiety.
Lack of information.
The seven participants who had no previous experience with constant observation had little understanding of its purpose, what it entailed, or criteria for its termination. They complained about not understanding the role or training of the observers, and some noted that the observers did not provide information in a helpful way. For example, one participant noted, "They were constantly correcting me on what I could and couldn't do. They were saying it in a way that wasn't nice; it was just very abrupt: 'You can't do that.'"
Two participants reported that they learned about constant observation through a trial-and-error process, which at times produced anxiety, frustration, or irritability. Two participants mentioned that they would have found an information sheet helpful, with particular attention to observers' professional training, degrees, and duties.
Lack of privacy.
The single most uncomfortable and embarrassing aspect of constant observation for ten participants was lack of privacy, particularly during use of the bathroom. Eight females and two males complained about the lack of privacy, and it was particularly distressing for the two participants who reported histories of sexual abuse and for the two who experienced paranoia. "I don't like it because you don't have any privacy," one participant stated. "You don't dress, take a shower, or go the bathroom. You always have someone with you. It's embarrassing."
Five participants reported feelings of anger over the lack of privacy, and five reported disruption in daily hygiene and elimination.
Invasion of personal space.
The participants also complained about lack of personal space. Seven participants complained of feeling claustrophobic due to the close proximity of the observer, which produced increased anxiety and irritability. "Everyone has their boundaries, and when you're on one-to-one, even though they are clear across the room most of the time, it feels like they are right there in your face," noted one participant.
Confinement.
Five participants found lack of freedom during constant observation to be very unpleasant. They described a lack of freedom as the inability to walk around unsupervised and to shower at will. One said, "Can't walk. I can't leave the TV room. . . . I'd see all these other patients walking about free and I'd think, 'Why can't I do that?'"
As a result of lack of privacy, invasion of personal space, and confinement, 15 participants reported relief when constant observation was discontinued. Two participants informed researchers that they lied about their degree of suicidality to hasten the termination of constant observation.
Therapeutic and nontherapeuticextraneous factors
To a lesser degree participants attributed therapeutic effects during constant observation to factors not related to the observer, called extraneous factors. Therapeutic extraneous factors included improved sleep during this time, receiving medication, and the passage of time. A nontherapeutic extraneous factor was noise.
Sleep.
Fourteen participants experienced sleep deprivation before being placed on constant observation. Eight reported that their sleep improved during constant observation, and four attributed the improvement to the sedating effects of their medication. Two others attributed the improvement in sleep to the protective aspects of constant observation that allowed them to relinquish internal control over their suicidal impulses, which induced relaxation. These participants also reported that sleep improvement decreased their negative thinking and suicidal ideation and impulses. As a participant observed, "Sleep makes me feel better. It helps because I got a chance, both my body and my brain had a chance, to rest. . . . It gets me off negative thoughts."
Medication.
Seventeen participants were on multiple medications during constant observation, and seven perceived that they benefited from the medications. "I had so much Ativan in my system. . . . It helped me. I woke up and I was in a different frame of mind," one said. Four participants stated they experienced medication-induced improvement in sleep, and three noted a decrease in command hallucinations while medicated. Two participants believed medication improved their dysphoric mood, and six believed that medication would stabilize their mood later in the hospitalization.
Fifteen participants reported that recovery from suicidal ideation or impulses during constant observation required a variety of therapeutic interventions in addition to medications, such as support, protection, and distraction.
Passage of time.
Six participants believed that their dysphoric moods or suicidal feelings improved due to the passage of time while on constant observation. One participant said, "Your mind isn't static. It doesn't stay in one place. You drift into wanting to kill yourself. As much as you drift into it, you can drift out of it. So having time, just the time, even if nothing else happened, just the time allows you the ability to change your mind."
Noise.
Loud and disruptive noise was disturbing to some participants during constant observation. Two of the three hospitals in the study routinely conducted constant observation in dayroom settings with a television turned on. Five of the 13 participants who were exposed to television noise complained of experiencing additional stress, particularly when soap operas and talk shows were on. One participant complained, "I'd like to get away from that TV because I had to be in the dayroom. And I felt stretched because I had to tolerate talk shows and soap operas."
Discussion and conclusions
The participants in this study viewed constant observation not only as a protective intervention but as one that had therapeutic benefit. The primary perceived benefit was obtained through observer's specific interventions, and other benefits were from extraneous factors.
Most therapeutic benefits were attributed to the observers' being perceived as having a positive attitude and engaging the participants in active supportive interventions. Distraction, in particular, was commonly mentioned. Distracting activities induced short-term reduction of suicidal impulses. Study participants reported that even if the impulses returned, they had decreased in intensity. This finding is consistent with cognitive therapists' conclusion that distracting or diverting activities decrease dysfunctional thoughts, including suicidal thoughts and impulses (
6,
7).
Not surprisingly, participants found observers' acknowledgment of them as unique and meaningful human beings to be therapeutic. Acknowledgment, similar to what has been described as recognition or validation in the psychiatric literature (
8,
9), reduced anxiety, loneliness, and dysphoria and was instrumental in building observer-participant relationships. On the other hand, perceived lack of acknowledgment and empathy from observers produced anger or anxiety.
These findings support the belief that patients respond to effective staff interventions. The importance of staff awareness of such dynamics reaffirms the need for careful planning and supervision of observers' behavior and interventions.
Adverse effects associated with the intrusiveness of constant observation, such as lack of privacy, intrusions into personal space, and feelings of confinement, were also reported. These effects, which are rarely reported in the literature, ranged from mild discomfort—for example, disruptions in daily hygiene and elimination—to worsening of symptoms, such as increased anxiety and irritability. Two participants admitted that they lied when they said that their suicidal ideation was no longer present so that constant observation would be discontinued.
Patients on constant observation who request privacy while using the bathroom and while showering present clinical dilemmas. On the one hand, as this study and others have found (
10), some patients search for means with which to commit suicide during constant observation and closely watch observers for lapses in vigilance. On the other hand, as this study and others have also found (
3,
11,
12), some patients' symptoms worsen during constant observation, which may be a result of its intrusive nature. Decisions about privacy must be based on the professional and legal judgments of the clinician, the treatment team, and policy makers. For patients whose symptoms appear to worsen during constant observation, a risk analysis reassessment should be conducted to determine the appropriateness of this procedure.
To a lesser degree, the participants perceived therapeutic benefits from interventions not related to the observer, the extraneous factors. They included sleep promotion, medication, and the passage of time. Improved duration and quality of sleep decreased participants' affective instability and dysphoria and increased their ability to control suicidal ideation and impulses. This finding emphasizes the need for staff awareness of the sleep patterns of patients during constant observation, because improved sleep may play a role in decreasing suicidal ideation.
A nontherapeutic extraneous factor was noise—in particular, television noise—which increased anxiety for some participants. Constant observation should probably not be conducted in areas with television or other noisy activities, and staff should elicit the patient's preference in this regard.
The results of this study support the view that constant observation can be both a therapeutic and a protective intervention, and that much of the therapeutic benefit derives from an observer's attitudes and behaviors. This view may raise objections from health professionals who believe that observers' approach should be more impersonal and detached, and that those who play a more active and supportive role are inadvertently rewarding patients' suicidal behavior by allowing them to obtain increased staff attention.
Assuming that the participants in our study were candid, our findings do not support the idea that patients obtain a secondary gain from constant observation. In fact, most participants were happy to have the procedure discontinued, mainly because of its confining aspects. Seeking secondary gain may be a less common goal than some staff suspect, shared by only a small subgroup of patients.
Participants in our study preferred observers whose interactions were kind and supportive rather than impersonal and detached. Maris and associates (
13) state that "any treatment of a suicidal patient that relies on impersonal means alone (e.g., the prescription of medication, seclusion, restraint, checks, etc.) is second rate" and add that "the heart of the treatment is the relationship with the therapist." To this we add the relationship with the observer as well.