The 12-month prevalence of diagnosable psychiatric disorders in the U.S. general population is estimated to be between 26% and 30% (
1–
3). High rates of psychiatric disorders have also been reported among U.S. military service members (
4–
8); within the Department of Veterans Affairs (VA), an estimated 37% to 40% of veterans have a psychiatric disorder (
9–
11).
Many VA patients with psychiatric disorders have comorbid general medical problems and multiservice needs. Current diagnoses of posttraumatic stress disorder (PTSD) and major depression have been found to be independently associated with higher numbers of current health complaints and of health problems over a lifetime and in the past year (
12). Additionally, the mean years of potential life lost and standard mortality ratio for all causes of death are substantially increased among psychiatric patients compared with the U.S. general population (
13).
Understanding how veterans with psychiatric disorders perceive the quality of their VA health care is important because the presence of a psychiatric disorder may influence ratings of satisfaction with and utilization of health care and subsequent treatment outcomes. Several studies have examined satisfaction with inpatient care among veterans with psychiatric disorders. One study that examined veterans who had a primary psychiatric or substance use disorder and who were recently discharged from medical, surgical, and psychiatric units found that older age and better health were associated with increased satisfaction on all measures; the findings for gender and race-ethnicity were mixed. Additionally, schizophrenia, PTSD, major affective disorders, and alcohol and drug abuse were associated with increased satisfaction on several measures (
14).
Another study found that veterans with psychiatric diagnoses had lower levels of satisfaction with inpatient medical, surgical, or psychiatric care than those with general medical diagnoses. Additionally, having a mental health diagnosis and receiving treatment in a psychiatric program (rather than in a medical unit), age, and subjective physical health were the strongest predictors of satisfaction with inpatient care (
15). Finally, a study examining patient satisfaction at discharge from inpatient mental health treatment found that veterans who reported fewer symptoms, higher quality of life, and a higher level of functioning at admission were more satisfied with services and that patients with diagnoses of PTSD or a personality disorder were less satisfied with services (
16).
Only one study, to our knowledge, has examined satisfaction with outpatient health care among patients with psychiatric disorders in the VA. It focused on treatment in primary care and found that for most psychiatric disorders, patients with the disorder were less satisfied with their treatment than patients without the disorder (
17). Other related research has found that patients are more satisfied with the tangible aspects of their health care visits than with the subjective components. For example, patients who received a mental health service in the past year reported being more satisfied with the accessibility, environment, appropriateness, and affiliation and esteem aspects of their health care visits and less satisfied with the goal attainment and self-actualization aspects (
18).
Additionally, aged and disabled patients with psychiatric disorders reported being less satisfied with their follow-up care, doctor's concern for their overall health, the health information they received, and the overall quality of their care than did those without psychiatric disorders (
19).
Communication between providers and patients may be particularly important for determining satisfaction with the subjective components of the health care experience. For patients who received general medical services, the interpersonal processes that occurred during the health care visit, such as “eliciting and responding to concerns” and “deciding together,” were positively related to their satisfaction with physicians, with health care, and with recommending physicians (
20). Additionally, health service users who are older, black, or Hispanic or who have public insurance reported more positive communication with health care providers (
21). Little is known about the extent to which patient characteristics are associated with perceptions of positive communications and with satisfaction with and quality of outpatient health care experiences among patients with psychiatric diagnoses.
This study examined the perceptions among VA patients with psychiatric diagnoses of their experiences during outpatient general medical visits. We studied the impact of demographic and clinical characteristics on patients' perceptions of their experiences during outpatient health care visits using survey responses about provider attentiveness, confidence and collaboration in health care decisions, and overall quality of care.
These data will inform future efforts to treat veterans by improving the quality of care they receive, increasing their utilization of health care services, and improving their physical and mental health functioning. This research may also facilitate improvements in patient-provider communications and, in turn, in the overall quality of health care.
Methods
Data source
This study was based on secondary analyses of data from the Survey of Health Care Experiences of Patients (SHEP), an initiative managed by the Veterans Health Administration (VHA) Office of Quality and Performance that regularly solicits patient data on their most recent episode of inpatient or outpatient care. The survey uses a stratified random sample without replacement design and includes assessments of health status and demographic variables. For the outpatient survey, used in this study, a random sample is selected from patients who had a visit to a VA clinic in that month.
To ensure sufficient representation of primary and specialty care, a fixed number of patients were randomly selected from each of three groups—new primary care, established primary care, and specialty care—from each VHA clinic nationally (N>800 per group). For this study, the SHEP survey data were linked to VA administrative data on diagnosis and demographic characteristics of the respondents. The use of these data for research was approved by the institutional review board at the VA Ann Arbor Healthcare System.
Additional details of the survey methodology have been described elsewhere (
22).
Sample
The sample included veterans ages 18 and older with psychiatric disorders who completed SHEP during fiscal year (FY) 2005. We identified patients with psychiatric disorders on the basis of ICD-9 diagnoses in administrative data of anxiety, depression, bipolar disorder, PTSD, schizophrenia, or substance abuse. Only veterans who received care through the VA health care system were eligible to participate in the SHEP.
Dependent variables
Four questions were chosen from the SHEP as measures of the patients' perception of their experiences with health care providers and probable indicators of their satisfaction with care. Each was examined as an independent outcome. These dependent variables were “Did the provider listen to what you had to say?” “Were you involved in decisions about your care as much as you wanted?” “Did you have confidence and trust in the provider you saw?” and “Overall how would you rate the quality of this visit?” Possible responses to the first three questions were Yes, completely, Yes, somewhat, and No and an additional choice of “Nothing to discuss” for question 1. Responses to the fourth question were poor, fair, good, very good, and excellent.
Independent variables
The independent variables derived from administrative records included sex (male or female), age (18–34, 35–49, 50–64, and 65 and older), and service-connected disability (yes or no). Veterans with a disability rated at 10% or more resulting from their military experiences may qualify to receive certain VA benefits. Demographic variables derived from the SHEP were those not reliably recorded in the administrative data including race (white or nonwhite), marital status (never married; married or cohabitating; or separated, divorced, or widowed), education (high school or less or some college or more), and income (≥$30,000 or <$30,000). Additional covariates of interest included primary or secondary ICD-9diagnoses of anxiety disorders (300.00–300.02, 300.09–300.10, 300.20–300.23, and 300.29), depression (293.83, 296.2, 296.3, 298.0, 300.4, 301.12, 309.0, 309.1, 309.28, and 311), bipolar disorder (296.0–296.1, 296.4–296.8), PTSD (309.81), schizophrenia (295), or substance use disorders (291, 292, 303.0, 303.9, 304, 305.0, 305.2–305.9, excluding 305.x3, substance use disorders in remission), which were also ascertained from administrative data.
Analytic strategy
The survey weights functions of Stata10 were used to conduct all statistical analyses and facilitate the calculation of population-representative estimates. First we calculated weighted percentages and their corresponding standard errors to describe the distribution of demographic and clinical characteristics within the sample. Next we tested the bivariate associations of demographic and clinical characteristics with each of the four outcome measures of perceptions of health care experiences using chi square tests. Responses to questions 1–3 were classified as yes, no, and in the case of question 1, “Nothing to discuss.” Responses to question 4 were grouped as either poor or fair or as good, very good, or excellent. Finally, we conducted multinomial and logistic regression analyses to calculate adjusted odds ratios (AORs) with 95% confidence intervals (CIs) for the associations of demographic and clinical covariates with each of the four outcomes after adjustment for all of the independent variables.
Multinomial regression was used for the outcome of question 1 (“Did the provider listen to what you had to say?”) because it had three response options; logistic regression was used for the other outcomes. All study results used sample weights to adjust for survey nonresponse and for the complex sampling design. Therefore, results presented here represent population rather than sample estimates.
Results
Sample characteristics
In total, 261,962 veterans completed the SHEP in FY 2005, and 55,578 (21.2%) had psychiatric diagnoses and, therefore, were included in the study analyses. Given the large sample size, several of the independent variables were found to be significantly associated with perceptions of outpatient health care experiences in the bivariate and multivariable analyses. Although there are no existing guidelines, we defined clinical significance as an increase or decrease of 20% or more in odds of having positive health care experiences in the multivariable analyses.
Bivariate analyses
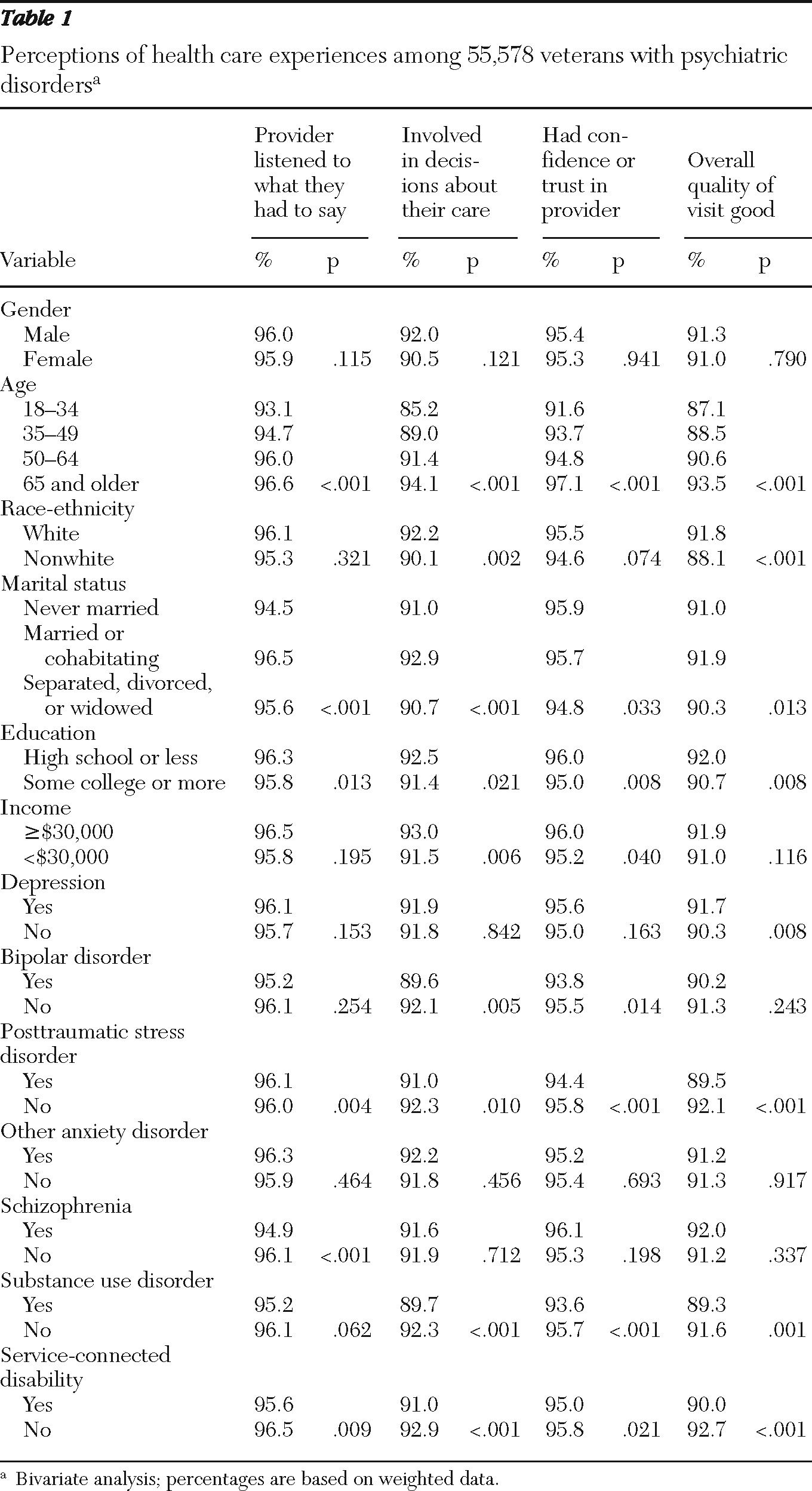
Most (96%) veterans with psychiatric disorders reported that their provider listened to what they had to say. In bivariate analyses, veterans who were younger than 49, who were unmarried (never married or separated, divorced, or widowed), who had some college education, and who had a service-connected disability were less likely to report that their provider listened to what they had to say (
Table 1). Veterans with PTSD were more likely and those with schizophrenia were less likely to report that their provider listened to what they had to say.
Approximately 91.9% of veterans with psychiatric disorders reported that they were involved in making decisions about their care. In bivariate analyses, veterans who were younger than 49, were nonwhite, were unmarried (never married or separated, divorced, or widowed), had some college education, had incomes under $30,000, and had a service-connected disability were less likely to report that they were involved in making decisions about their care. Those with diagnoses of bipolar disorder, PTSD, or substance use disorder were also less likely to report that they were involved in decision making about their care.
Almost all (95.4%) veterans with psychiatric disorders reported that they had confidence and trust in their provider. Bivariate analyses found that veterans were less likely to report they had confidence and trust in their provider if they were younger than 65; were separated, divorced, or widowed; had some college education; had incomes under $30,000; and had a service-connected disability. Those with diagnoses of bipolar disorder, PTSD, or substance use disorder were also less likely to report they had confidence and trust in their provider.
Most (91.2%) veterans with psychiatric disorders reported that the overall quality of their visit was good. In bivariate analyses, veterans were less likely to report that the overall quality of their visit was good if they were younger than 65; were nonwhite; were separated, divorced, or widowed; had some college education; and had a service-connected disability. Those with diagnoses of depression were more likely and those with PTSD or substance use disorders were less likely to report that the overall quality of their visit was good.
Multivariate analyses
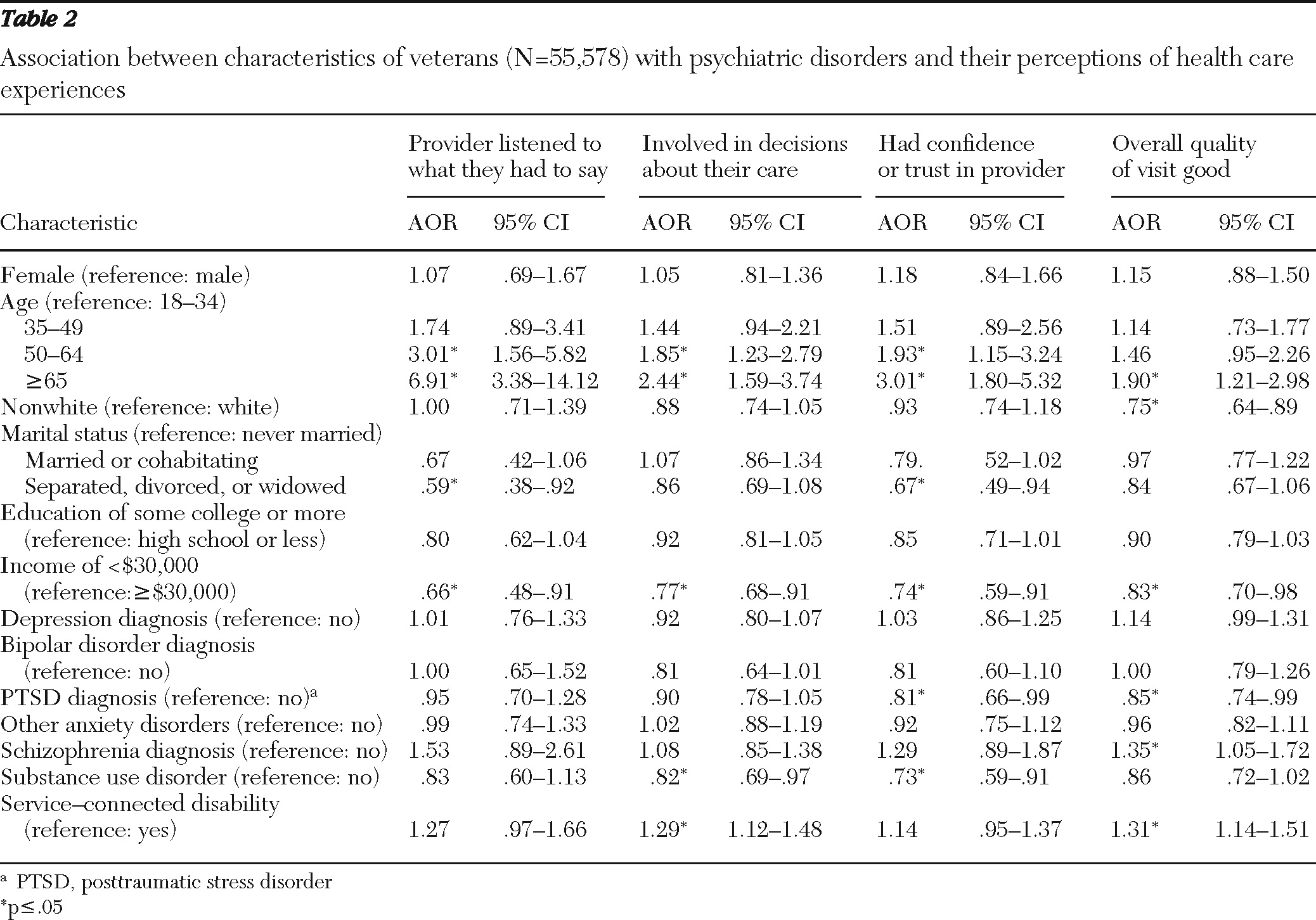
Multivariable analyses found that veterans with psychiatric disorders who were older than 50 were at increased odds of reporting that the provider listened to what they had to say (
Table 2). Additionally, those who were separated, divorced, or widowed or who had an income under $30,000 were at decreased odds of reporting that their provider listened to what they had to say.
Veterans who were older than 50 and did not have a service-connected disability were at increased odds of reporting that they were involved in making decisions about their care. Those who had incomes under $30,000 and those who had a substance use diagnosis were at decreased odds of reporting being involved in making decisions about their care. Veterans who were older than 50 were at increased odds of reporting that they had confidence and trust in their provider. The odds of reporting confidence and trust in their provider were decreased for veterans who were separated, divorced, or widowed; those with incomes under $30,000; and those with PTSD or a substance use disorder diagnosis.
The final set of analyses examined perceptions of overall quality of care. Veterans who were 65 years and older, had a service-connected disability, and had a schizophrenia diagnosis were at increased odds of reporting that the overall quality of their visit was good. Those who were nonwhite, had an income below $30,000, and had a diagnosis of PTSD were at decreased odds of reporting that the overall quality of their visit was good.
Discussion
This study examined the perceptions among VA patients with psychiatric diagnoses of their experiences during outpatient health care visits using a large nationally representative sample of veterans. Most (91%–96%) VA patients with psychiatric disorders evaluated their outpatient health care experiences positively, but the rates were somewhat lower than those among veterans (95%–98%) without psychiatric disorders. These findings are generally consistent with past research that has found that 93% of aged and disabled patients in a community sample reported that they were “satisfied” or “very satisfied” with the overall quality of their health care (
19).
Demographic and clinical characteristics were important predictors of who was less likely to make positive evaluations of their health care experiences. In general, those who were older and who did not have a service-connected disability were more likely to evaluate their outpatient health care experiences positively and those who were nonwhite and had incomes under $30,000 were less likely to evaluate their outpatient health care experiences positively.
Additionally, those with diagnoses of schizophrenia were more likely to and those with diagnoses of PTSD and a substance use disorder were less likely to evaluate their outpatient health care experiences positively. This study provides new information about patients who are less satisfied with their outpatient health care and could inform ways of improving health care experiences and subsequent health outcomes.
Among veterans with psychiatric disorders, younger age, minority race or ethnicity, and being married or previously married predicted a negative evaluation of the health care experience in at least one of the four domains assessed. These findings suggest that there is an opportunity to improve clinical practice and design health care services to better serve certain patients. These results may also have implications for improvements to mental health services, as past research has found that these characteristics are related to rates of mental health service utilization and treatment dropout. Specifically, those who are aged 18 to 34, are married, and are of a minority race or ethnicity are less likely to receive mental health treatment (
23–
25), and dropout rates for mental health treatment are higher for those who are younger and of minority race or ethnicity (
26–
28).
Improvements to health care services may come in the areas of building rapport and developing ways to include patients in decisions about their health care. These recommendations are consistent with the finding that those who were younger were less likely to report that they felt that they had been involved in making decisions about their care, that the provider had listened to them, and that they had had confidence or trust in the provider. Future work is needed to determine whether providers treat younger patients differently or whether younger patients tend to perceive similar experiences more negatively.
As the conflicts in Afghanistan and Iraq continue, U.S. military service members are returning to the states with high rates of mental health and substance use problems (
6,
9,
29). Being younger and of low income, as are many of the service members engaged in these conflicts (
6,
9,
30,
31), places veterans at increased risk for developing mental health and substance use problems (
30,
32). The results from our study indicated that younger and low-income veterans are also less likely to have positive experiences with their outpatient health care providers. These results indicated that VA treatment providers should take extra care to meet the health care needs of recent returnees.
PTSD and substance use disorders were associated with a decreased likelihood of a positive report on at least one of the outcome measures. The symptoms related to these psychiatric disorders may contribute in part to negative perceptions by these patients of their experiences with health care providers and make it more difficult for them to engage in treatment. In either case, it may be of benefit for general medical providers to give special attention to engaging and building rapport with patients with a psychiatric history. Psychoeducation for both physicians and psychiatric patients may be helpful in this regard. Consistent with past research (
14), veterans with schizophrenia were more likely to report that the overall quality of their visit was good. Veterans with this type of chronic and severe psychiatric condition may benefit from being able to receive long-term psychiatric services in a comprehensive health care system that can also assist with practical (for example, employment and housing) and general medical needs.
Several limitations of this study should be noted. The SHEP relies on self-report data; therefore, recall and reporting biases were possible. The ICD-9 codes used in patient selection included both primary and secondary diagnoses, and VA administrative data contain somewhat unreliable secondary diagnosis codes. The SHEP does not include data on the providers' level of training, a variable that may also have an influence on care. Because the study examined outpatient health care experiences among patients with psychiatric disorders, we did not examine patients without psychiatric disorders. Future studies that also include veterans without psychiatric disorders would provide an additional context for these results.
Additionally, because this study examined outpatient health care experiences in several sectors of care, the results may have been affected by differences within specific clinics. The SHEP is a cross-sectional survey, so the temporal relationship between clinical characteristics and evaluation of outpatient health care experiences could not be established. Finally, the generalizability of these data might be limited to only veteran populations.
Conclusions
The results of this study indicated that patients with psychiatric disorders had generally positive perceptions of the quality of their outpatient health care at the VA. Those who were less likely to evaluate their health care experiences positively, namely those who were younger, from minority racial or ethnic groups, or of low income, were also those who have been found in previous research to be at risk for dropping out of mental health treatment. This study also suggested that because many U.S. Operation Enduring Freedom-Operation Iraqi Freedom service members who present to the VA are younger, are low income, and have PTSD or substance use problems or both, service members returning from current conflicts are less likely to have positive experiences with health care providers and to comply with treatment.
These findings provide new information that may inform the development of interventions for certain patient populations aimed at improving satisfaction with outpatient health care and compliance with treatment recommendations and treatment outcomes. In the past, the SHEP survey results related to racial and gender disparities have led to changes in health care delivery; the data presented would be similarly likely to help efforts to build rapport between doctors and patients and include patients in decisions about their care.
Acknowledgments and disclosures
This work was supported by the Advanced Fellowship Program in Mental Illness Research and Treatment, Office of Academic Affiliations, Department of Veterans Affairs (VA); a career development award from VA Health Services Research and Development (HSR&D) (CD2 07-206-1); a service grant from HSR&D (IAC 08-099); and a grant from the National Institute on Drug Abuse (1R21DA026925). The views expressed in this report are those of the authors and do not necessarily represent those of the VA.
The authors report no competing interests.