The methods for this systematic review follow the Agency for Healthcare Research and Quality (AHRQ) Methods Guide for Effectiveness and Comparative Effectiveness Reviews (available at https://effectivehealthcare.ahrq.gov/products/collections/cer-methods-guide) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Moher et al. 2015). The final protocol of this review was registered on PROSPERO (Registration #: CRD42020194098). All methods and analyses were determined a priori.
Literature Searches
Initial searches were conducted on June 7, 2018, by APA staff using MEDLINE (PubMed), EMBASE, the Cochrane Library (Wiley), and PsychInfo (EBSCO). Subsequent searches were conducted by RTI. Searches differed in exact search strings; however, to ensure optimal recall, the RTI searches were reviewed in detail to ensure that the revised search strategy still detected all studies that met inclusion criteria of the original search. These searches were also conducted in MEDLINE, EMBASE, the Cochrane Library, and PsychINFO from January 1, 2018, to June 15, 2020. Additional overlapping update searches of MEDLINE and PsycINFO were run in April and September 2021. Our search strategies used a variety of terms, medical subject headings (MeSH), and major headings, and were limited to English-language and human-only studies.
To minimize retrieval bias, we manually searched reference lists of landmark studies and background articles on this topic for relevant citations that electronic searches might have missed.
Doctor Evidence Original Search Strategy
Search Date: June 7, 2018
PubMed search strategy for borderline personality disorder
Search ID#
Query
Results
#1
(“Borderline Personality Disorder”[Mesh]) OR (borderline [tiab] AND personality [tiab])
8,962
#2
(“animals”[MeSH Terms] OR animal [tiab] OR animals [tiab] OR rat [tiab] OR rats [tiab] OR mouse [tiab] OR mice [tiab] OR rodent [tiab] OR rodents [tiab]) NOT (“humans”[MeSH Terms] OR humans [tiab] OR human [tiab])
PsycINFO search strategy for borderline personality disorder
Search
Query
Limiters/Expanders
Results
S1
MM “Borderline Personality Disorder”
5,220
S2
DE “Borderline Personality Disorder”
7,857
S3
MA “borderline personality disorder”
4,192
S4
TI “borderline personality” OR AB “borderline personality” OR SU “borderline personality” OR KW “borderline personality”
11,400
S5
S1 OR S2 OR S3 OR S4
11,400
S6
(MM “Animals” OR DE “Animals” OR DE “Vertebrates” OR DE “Amphibia” OR DE “Birds” OR DE “Fishes” OR DE “Mammals” OR DE “Pigs” OR DE “Reptiles” OR DE “Rats” OR DE “Rodents” OR DE “Mice”)
329,022
S7
TI “animals” OR TI “animal” OR TI “mouse” OR TI “mice” OR TI “rodent” OR TI “rodents” OR TI “rat” OR TI “rats” OR SU “animals” OR SU “animal” OR SU “mouse” OR SU “mice” OR SU “rodent” OR SU “rodents” OR SU “rat” OR SU “rats” OR KW “animals” OR KW “animal” OR KW “mouse” OR KW “mice” OR KW “rodent” OR KW “rodents” OR KW “rat” OR KW “rats” OR AB “animals” OR AB “animal” OR AB “mouse” OR AB “mice” OR AB “rodent” OR AB “rodents” OR AB “rat” OR AB “rats”
426,155
S8
Limiters—Population Group: Animal
385,743
S9
S6 OR S7 OR S8
459,805
S10
Limiters—Population Group: Human
3,780,890
S11
TI “humans” OR TI “human” OR AB “humans” OR AB “human” OR SU “humans” OR SU “human” OR KW “humans” OR KW “human”
PubMed search strategy for borderline personality disorder
Search
Query
Results
#1
“Borderline Personality Disorder”[Mesh] OR “Borderline Disorder”[ti] OR “Borderline Personality Disorder”[tiab] OR “borderline-patient”[ti] OR “borderline patient”[ti] OR “borderline-patients”[ti] OR “borderline patients”[ti]
8,693
#2
#1 AND (“2018/01/01”[Date—Publication]: “3000”[Date—Publication])
EMBASE search strategy for borderline personality disorder
Search
Query
Results
#1
(‘borderline state’/de OR ‘borderline disorder’:ti OR ‘borderline-patient’:ti OR ‘borderline patient’:ti OR ‘borderline-patients’:ti OR ‘borderline patients’:ti OR ‘borderline personality disorder’:ti,ab,kw) AND [2018-2020]/py AND [english]/lim
1,777
#2
‘borderline personality disorder’:ti,kw AND [english]/lim AND [1-1-2018]/sd
Cochrane Library search strategy for borderline personality disorder
Search
Query
Results
#1
(“Borderline Disorder” OR “Borderline Personality Disorder” OR “borderline-patient” OR “borderline patient” OR “borderline-patients” OR “borderline patients”):ti,ab,kw OR [mh “Borderline Personality Disorder”]
851
#2
#1 with Cochrane Library publication date from Jan 2018 to present, in Cochrane Reviews, Cochrane Protocols, Trials, Clinical Answers, Editorials and Special collections
PsycINFO (via ProQuest) search strategy for borderline personality disorder
Search
Query
Results
S1
if(“Borderline Personality Disorder”) OR mjsub(“Borderline Personality Disorder”) OR mainsubject(“Borderline Personality Disorder”) OR ti(“Borderline Personality Disorder” OR “Borderline Disorder” OR “borderline-patient” OR “borderline patient” OR “borderline-patients” OR “borderline patients”) OR ab(“Borderline Personality Disorder”)
Additional limits—Date: After January 01 2018; Language: English
PubMed search strategy for borderline personality disorder
Search
Query
Results
#1
“Borderline Personality Disorder”[Mesh] OR “Borderline Disorder*”[ti] OR “Borderline Personality Disorder*”[tiab] OR “borderline patient”[ti] OR “borderline patients”[ti]
9,260
#2
#1 NOT (“Animals”[Mesh] NOT “Humans”[Mesh])
9,258
#3
(#2) AND ((“2020”[Date—Publication]: “3000”[Date—Publication])) Filters: English
PubMed search strategy for borderline personality disorder
Search
Query
Results
#1
“Borderline Personality Disorder”[Mesh] OR “Borderline Disorder*”[ti] OR “Borderline Personality Disorder*”[tiab] OR “borderline patient”[ti] OR “borderline patients”[ti]
9,488
#2
#1 NOT (“Animals”[Mesh] NOT “Humans”[Mesh])
9,486
#3
(#2) AND ((“2020”[Date—Publication]: “3000”[Date—Publication])) Filters: English
Criteria for Inclusion/Exclusion of Studies in the Review
The criteria for inclusion and exclusion of studies are designed to identify research that can answer the key questions. The criteria are based on the population, intervention/exposure, comparator, outcomes, time frames, country and clinical settings, and study design (PICOTS).
Inclusion and exclusion criteria
Criteria
Include
Exclude
Participants/population
Age ≥ 13
Age < 13
Diagnosed with BPD as defined by DSM-IV, DSM-IV-TR, DSM-5 (Section II or Section III), or ICD-10
Individuals with borderline traits without a specific diagnosis
For mixed population studies, BPD must account for ≥ 75% of the total population
Diagnosed with BPD as defined by DSM-III-R
Subgroups of interest:
Studies in which the primary research focus is a different diagnosis with co-occurring BPD in a subset (< 75% of the total population)
Co-occurring mental disorder
Age
Gender
Race/ethnicity
Genotypes (related to treatment selection, treatment response, or adverse effects)
Intervention(s)/exposure(s)
Yoga
Complementary/alternative treatments not listed for inclusion
Exercise
Somatic therapies
Peer-support interventions
Bioenergetic analysis
Psychosocial support
Body psychotherapy
Safety planning
Core energetics
Service delivery approaches:
Hakomi
Stepped-care
Somatic experiencing
Collaborative care
Pharmacotherapies
Measurement-based care
Acetazolamide
Treatment setting comparisons
Ethosuximide
Face-to-face sessions
Felbamate
Group sessions
Fosphenytoin
Online programs
Lacosamide
Therapeutic community
Methsuximide
Video
Pentobarbital
Progressive muscle relaxation
Perampanel
Somatic therapies:
Primidone
Electroconvulsive therapy (ECT)
Rufinamide
Repetitive transcranial magnetic stimulation (rTMS)
Droperidol
Transcranial alternating current stimulation (tACS)
Systems Training for Emotional Predictability and Problem Solving (STEPPS)
Transference-focused psychotherapy (TFP)
Comparator(s)/control
Interventions listed above for inclusion
Interventions listed as excluded above for interventions/exposures
Placebo
Treatment as usual
Wait-list control
Community treatment by experts
General psychiatric management
Standard group treatment
Standard psychiatric care
Structured clinical management
Outcomes
Pre-specified outcomes and outcome measures
Outcomes not listed, imaging markers, physiological markers, and biomarkers
A. BPD symptoms/diagnostic criteria
Outcomes that were not pre-specified, e.g., during post-hoc, exploratory analyses
1. Frantic efforts to avoid real or imaginary abandonment
2. Pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation
a. Inventory of Interpersonal Problems (IIP)
b. Distorted self-image
3. Identity disturbances: markedly and persistent unstable self-image or sense of self
a. Distorted self-image
4. Impulsivity
a. Impulsivity
b. Impulsive/behavioral
c. Risk taking behaviors
d. Lack of restraint
e. Barratt Impulsiveness Scale (BIS-11)
f. Multi-Impulsivity Scale (MIS)
5. Recurrent suicidal behavior, gestures, or threats; or self-mutilating behavior
a. Nonsuicidal self-injury
b. Suicide attempts
c. Suicide
d. Suicidal ideation
e. Self-destructive behavior
f. Beck Scale for Suicide Ideation (BSS)
g. Self-Harm Behavior Survey
h. Suicidal Behaviors Questionnaire (SBQ) and SBQ-R
i. Parasuicide History Interview (PHI)
j. Borderline Personality Disorder Severity Index (BPDSI) Parasuicidality Subscale
k. Columbia Suicide Severity Rating Scale (C-SSRS)
l. Deliberate Self-Harm Inventory (DSHI)
m. Self-Injurious Thoughts and Behaviors Interview-Self-Report
6. Affective instability, due to a marked reactivity of mood
a. Irritability
b. Mood swings
c. Difficulties in Emotion Regulation Scale (DERS)
d. Affective dysregulation
7. Chronic feelings of emptiness
8. Inappropriate intense anger or difficulty controlling anger
a. Aggression
b. Anger
c. Hostility
d. Aggressive behavior
e. Antisocial behavior
f. Spielberger State-Trait Anger Expression Inventory (STAXI)
g. Spielberger State-Trait Anger Scale (STAS)
h. Acting Out Scale (AOS)
i. Aggression Questionnaire (AQ)
j. Anger, Irritability, and Assault Questionnaire (AIAQ)
k. Overt Aggression Scale (OAS)
l. Buss Durkee Hostility Inventory (BDHI)
9. Transient, stress-related paranoid ideation, or severe dissociative symptoms
a. Dissociation
B. Scales for BPD
1. Borderline Personality Disorder Severity Index (BPDSI)
2. Zanarini Rating Scale (ZAN-BPD)
C. Other symptoms commonly found in individuals with BPD, but not part of the diagnostic criteria
1. Depression and Anxiety
a. Spielberger State-Trait Anxiety Inventory (STAI)
b. Symptom Checklist-90 (SCL-90)
c. Beck Anxiety Inventory (BAI)
d. Beck Depression Inventory (BDI)
e. Beck Hopelessness Scale (BHS)
f. Hamilton Rating Scale for Anxiety (Ham-A)
g. Hamilton Rating Scale for Depression (Ham-D)
h. Hospital Anxiety and Depression Scale (HADS)
i. Montgomery-Åsberg Depression Rating Scale (MADRS)
j. Patient Health Questionnaire (PHQ-9)
k. Brief Symptom Inventory (BSI)
l. Generalized Anxiety Disorder 7-item scale (GAD-7)
m. Patient Health Questionnaire–Adolescent
n. Patient Health Questionnaire: Somatic, Anxiety, and Depressive Symptoms
D. Functioning Scales
1. Global Adjustment Scale
2. Global Assessment of Functioning (GAF)
3. Quality of Life
4. Global Social Adjustment (GSA)
5. Global Severity Index (GSI)
6. Number of years with employment
7. Social Adjustment Scale (SAS)
8. Social and Occupational Functioning Assessment Scale
9. Social Functioning Questionnaire (SFQ)
10. Social History Interview (SHI)
11. Social Problem-Solving Inventory
12. World Health Organization—Disability Assessment Schedule (WHO-DAS)
E. Adverse events (AEs)
1. Rate of any AEs
2. Overall serious treatment-related AE rate
3. Specific serious treatment-related AEs
4. Study withdrawal due to AE
5. Study withdrawal for any reason
Timing
Treatment duration ≥ 8 weeks
Treatment duration < 8 weeks
Setting/context
Very high Human Development Index (HDI) countries*
All other countries
Study design
RCTs phase 2 | 3 | 4
Single-arm dose-finding trials
Nonrandomized clinical trials (N≥ 50):
Observational, noncomparative
Phase 1 | 2 | 3 | 4
Case reports/series
Observational studies, comparative (N ≥50)
Prognostic course/factor studies
Cross-sectional
Modeling studies
Prospective cohort
Pre-clinical
Retrospective cohort
Narrative reviews
Nonconcurrent cohort
Systematic reviews/meta-analyses (will be used for hand searches)
Case-control
Pooled analyses of controlled studies
BPD = borderline personality disorder; KQ = key question; N = sample size; NA = not applicable; RCT = randomized controlled trial.
*Very high HDI countries: Andorra, Argentina, Australia, Austria, Bahamas, Bahrain, Barbados, Belarus, Belgium, Brunei Darussalam, Bulgaria, Canada, Chile, Croatia, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hong Kong, China (SAR), Hungary, Iceland, Ireland, Israel, Italy, Japan, Kazakhstan, Korea (Republic of), Kuwait, Latvia, Liechtenstein, Lithuania, Luxembourg, Malaysia, Malta, Montenegro, Netherlands, New Zealand, Norway, Oman, Poland, Portugal, Qatar, Romania, Russian Federation, Saudi Arabia, Singapore, Slovakia, Slovenia, Spain, Sweden, Switzerland, Taiwan**, United Arab Emirates, United Kingdom, United States, Uruguay.
**The United Nations does not recognize Taiwan (i.e., Republic of China) as a sovereign state and does not include it in the HDI report. However, Taiwan’s government calculated its HDI to be 0.885, based on 2014 data and using the same methodology as the United Nations. This HDI value would place Taiwan among countries in the “very high” human development category and will be included in this report.
Literature Review, Data Abstraction, and Data Management
To ensure accuracy, two reviewers independently reviewed all titles, abstracts, and full-text articles. We used Distiller SR, an online tool to conduct systematic reviews, to screen the literature (DistillerSR, Evidence Partners, Ottawa, Canada). We resolved discrepancies by consensus or by involving a third, senior reviewer.
All results at both title/abstract and full-text review stages were tracked in an EndNote® bibliographic database (Thomson Reuters, New York, NY). Appendix I presents the list of studies excluded (with reasons) at the full-text level.
We designed, pilot tested, and used a structured data abstraction form in DistillerSR to ensure consistency of data abstraction. We abstracted data into categories that included (but were not limited to) the following: study design, eligibility criteria, intervention, methods of outcome assessment, population characteristics, sample size, attrition, results, and adverse event incidence. A second team member verified abstracted study data for accuracy and completeness.
Assessment of Risk of Bias of Individual Studies
To assess the risk of bias of studies, we used the Risk Of Bias In Non-randomised Studies of Interventions (ROBINS-I) (Sterne et al. 2016) for nonrandomized controlled studies, and for randomized controlled trials (RCTs), we used the Cochrane Risk of Bias 2 tool. Two independent reviewers assessed the risk of bias at the study level and also considered rating bias at an outcome level if methodological limitations might affect different outcomes in a different way (e.g., lack of blinding might increase the risk of bias for quality of life but not for overall mortality). We assigned a “high risk of bias” rating to studies that had very serious limitations in design or conduct that might invalidate findings regarding all or individual outcomes. Disagreements between the two reviewers were resolved by discussion and consensus or by consulting a third member of the team. Risk of bias diagrams were generated using the Risk-Of-Bias VISualization (robvis) tool (McGuinness and Higgins 2021; see Appendix E).
Data Synthesis
We summarized all included studies in narrative form and in summary tables that tabulate the important features of the study populations, design, intervention, outcomes, setting, country, and results. If we found three or more similar studies addressing an outcome of interest, we considered quantitative analysis (i.e., meta-analysis) if studies were similar (in population, interventions, comparators, and outcomes). For all analyses, we used random-effects models (restricted maximum likelihood random effects) to estimate pooled effects. To determine whether quantitative analyses were appropriate, we assessed the clinical and methodological heterogeneity of the studies under consideration following established guidance (Gartlehner et al. 2012). If we conducted meta-analyses, we assessed statistical heterogeneity in effects between studies by calculating the chi-squared statistic and the I2 statistic (the proportion of variation in study estimates attributable to heterogeneity). We examined potential sources of heterogeneity using sensitivity analyses. When quantitative analyses were not appropriate (e.g., due to heterogeneity, insufficient numbers of similar studies, or insufficiency or variation in outcome reporting), we synthesized the data qualitatively.
Grading the Certainty of Evidence for Major Comparisons and Outcomes
We graded the certainty of evidence of relevant outcomes based on current Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidance (Balshem et al. 2011). Developed to grade the overall certainty of a body of evidence, this approach incorporates five key domains: 1) risk of bias, 2) inconsistency, 3) indirectness, 4) imprecision of the evidence, and 5) reporting bias. It also considers other optional domains that may be relevant for some scenarios. These included plausible confounding that would decrease the observed effect and strength of association (i.e., magnitude of effect) or factors that would increase the strength of association (i.e., dose-response effect). Two reviewers assessed each domain for each selected outcome and resolved differences by consensus discussion. We documented all decisions regarding up- or down-grading the certainty of evidence to ensure transparency. We used GradePro to develop summary of findings tables for the guideline panel.
A2–14 describes the grades of certainty of evidence, which reflect the certainty of the body of evidence regarding a specific outcome.
Definitions of the grades of certainty of evidence
Grade
Definition
High
We are very confident that the estimate of effect lies close to the true effect for this outcome. The body of evidence has few or no deficiencies. We believe that the findings are stable (i.e., another study would not change the conclusions).
Moderate
We are moderately confident that the estimate of effect lies close to the true effect for this outcome. The body of evidence has some deficiencies. We believe that the findings are likely to be stable, but some doubt remains.
Low
We have limited confidence that the estimate of effect lies close to the true effect for this outcome. The body of evidence has major or numerous deficiencies (or both). We believe that additional evidence is needed before concluding either that the findings are stable or that the estimate of effect is close to the true effect.
Very low
We have no evidence, we are unable to estimate an effect, or we have no confidence in the estimate of effect for this outcome. The body of evidence has unacceptable deficiencies, precluding reaching a conclusion.
Results of Literature Search and Literature Screening
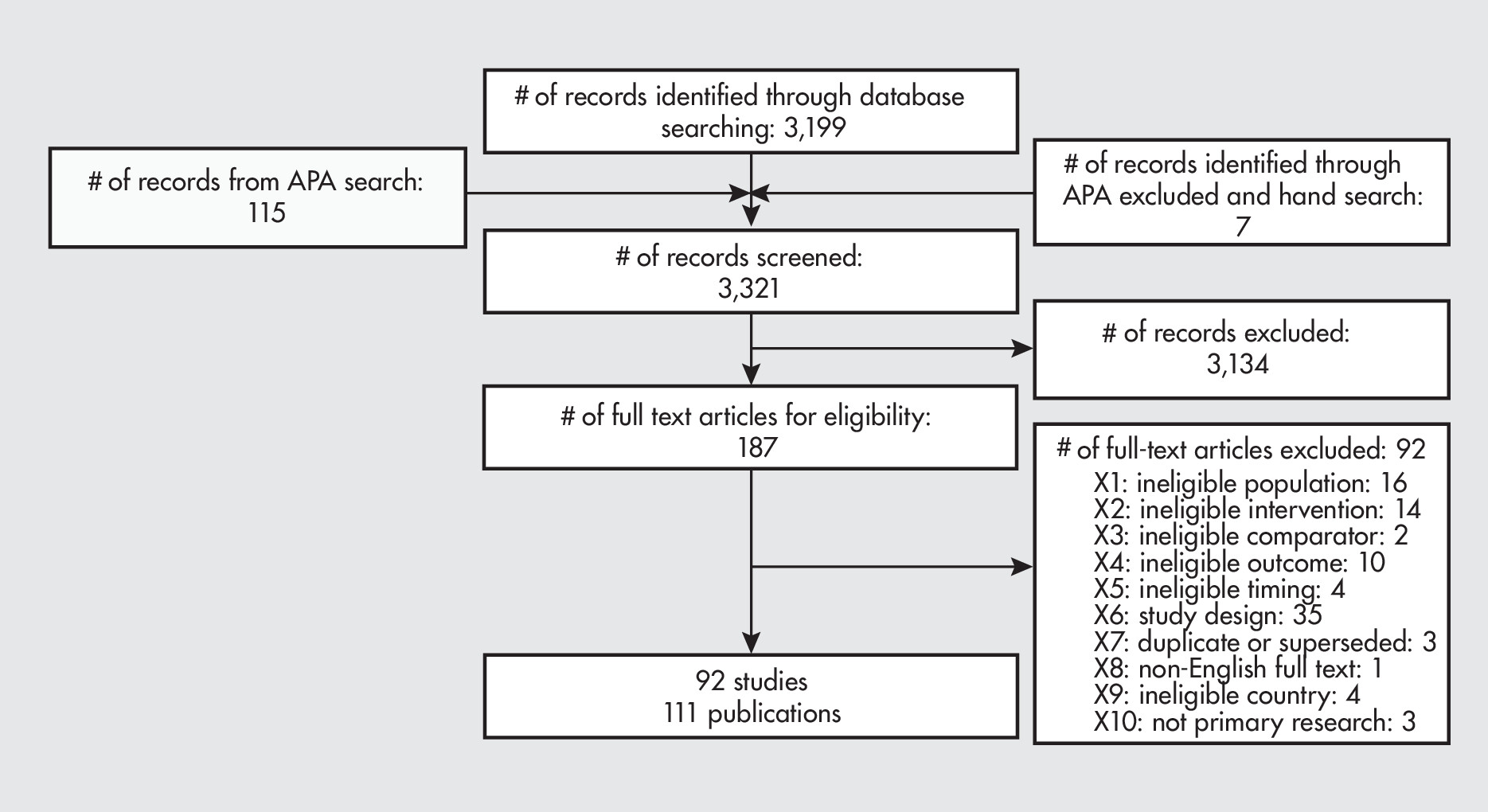
We screened 3,321 titles and abstracts from our literature searches. This represents 3,206 records from database and hand searches plus 115 studies previously included by a comparable search conducted by Doctor Evidence, of which we excluded 32 references. Overall, we identified 92 studies reported in 111 publications that met inclusion criteria (A2–1).
PRISMA flow chart.
APA = American Psychiatric Association; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
APA = American Psychiatric Association; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Table 1
PubMed search strategy for borderline personality disorder
Table 2
EMBASE search strategy for borderline personality disorder
Table 3
Cochrane Library search strategy for borderline personality disorder
Table 4
PsycINFO search strategy for borderline personality disorder
Table 5
PubMed search strategy for borderline personality disorder
Table 6
EMBASE search strategy for borderline personality disorder
Table 7
Cochrane Library search strategy for borderline personality disorder
Table 8
PsycINFO (via ProQuest) search strategy for borderline personality disorder
Table 9
PubMed search strategy for borderline personality disorder
Table 10
PsycINFO (via ProQuest) search strategy for borderline personality disorder
Table 11
PubMed search strategy for borderline personality disorder
Table 12
PsycINFO (via ProQuest) search strategy for borderline personality disorder
Table 13
Inclusion and exclusion criteria
Table 14
Definitions of the grades of certainty of evidence
Reference #1
Request Username
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.