There is compelling evidence from twin, family, and adoption studies to suggest that bipolar disorder is genetically transmitted (
1). Data from genetic linkage studies indicate the probability that familial bipolar disorder results from multiple genetic loci acting independently or in concert (
1–
4). Although results of genetic linkage studies of bipolar disorder have not been consistently replicated, positive evidence for linkage with chromosome 18 markers in bipolar families has been reported by three independent research groups (
2–
4). Furthermore, three groups have independently reported linkage of bipolar disorder to loci on human chromosome 21q (
5–
7).
If the disease-related mutations are identified for bipolar disorder, it will be possible to develop presymptomatic and prenatal tests for the disease. Consequently, options to take such tests, to abort a fetus that is at risk for developing bipolar disorder, or to test individuals at high risk will be available. Serious ethical considerations are involved with such options, especially given the probable complex inheritance pattern of bipolar disorder, the variation in age at onset and degree of severity of the disease, the availability of effective treatment, and the potential advantages that bipolar disorder may confer to some persons afflicted and to society (
8–
12).
The purpose of our study was to gain information about the attitudes of individuals with bipolar disorder and of their spouses toward some of the issues that are arising from advancing genetic research on bipolar disorder. There have been no previous studies comparing the knowledge and attitudes of bipolar patients and spouses with respect to genetic information; previous studies by Targum et al. (
13) and Frank et al. (
14) assessed the attitudes of bipolar patients and spouses toward marriage and childbearing. In addition, a recent study by Smith et al. (
15) evaluated the attitudes toward bipolar disorder and presymptomatic genetic testing among patients and health care providers.
METHOD
A 46-item questionnaire was distributed to 90 patients with bipolar disorder and to their spouses (a total of 180 questionnaires) between June and September 1993. Subjects with bipolar disorder were drawn from participants in the Johns Hopkins University bipolar disorder genetic linkage study, members of the Depression and Related Affective Disorders Association, and inpatients and outpatients of the affective disorders division of the Johns Hopkins University Hospital. An introductory letter describing the purpose and nature of the study was sent to 84 linkage study participants; this letter was followed, in turn, by a phone call from a researcher asking permission to send a questionnaire. Questionnaires were sent to 32 of the 84 linkage study participants and their spouses. Support group leaders of the Depression and Related Affective Disorders Association in Maryland, Pennsylvania, and Washington, D.C., were contacted to request permission to distribute questionnaires to their group members. Questionnaires were given to 52 of the members and their spouses. Some individuals completed the questionnaires at their group meeting, and others completed them at home and mailed them back. Questionnaires were also given to three outpatients and their spouses and to three inpatients and their spouses. To be eligible for the study, only one member of a married couple could have a diagnosis of bipolar disorder. All of the outpatient couples mailed the questionnaires back to us, while all of the inpatient couples completed them in the hospital.
After complete description of the study to all subjects, written informed consent was obtained. Patients and spouses were asked to complete the questionnaires independently. In most instances, a researcher was present to answer any questions that the subjects had. In instances where no researcher was present, the phone number of a researcher was given to the subjects so that they could call if they had any questions.
The questionnaire included 40 multiple-choice questions (20 of these in a Likert scale format and seven involving percentages), four questions requiring numerical answers, and two questions requiring an open, written response.
The subjects were asked to give social and demographic information and to designate the clinical diagnosis (bipolar type I or bipolar type II) of the affected member of the couple. Additional questions addressed the following issues: 1) the degree of knowledge that the subjects had about the genetics, severity, and rates of response to treatment of bipolar disorder; 2) the likelihood that these same individuals would take advantage of presymptomatic and prenatal genetic tests for bipolar disorder if they were to become available; 3) perceptions about the potential benefits and risks of knowing whether one carries a gene for bipolar disorder, and whether the benefits of knowing outweigh the risks; 4) whether knowledge that one was carrying a gene for bipolar disorder would affect decisions to get married and to have children; 5) preferences regarding the disclosure of bipolar disorder genetic information; 6) attitudes toward aborting a fetus with a gene for bipolar disorder; and 7) a comparison of subjects' attitudes in a wider range of situations that might justify abortion. We modeled several of the questions about abortion after those designed by Wertz et al. (
16).
Paired t tests were done on questions involving percentages, comparing a patient's and spouse's paired responses. McNemar chi-square statistics were used for paired categorical responses. We found no statistically significant differences in the responses to most questions. We have detailed the statistical analysis in this report only in instances where a statistically significant difference was found.
RESULTS
Of the 180 questionnaires distributed, 90 were returned to us. Thirty-four of the questionnaires received were completed by bipolar type I patients and their spouses, 42 were completed by bipolar type II patients and their spouses, and 14 were completed by couples for whom we were unable to ascertain the specific type of bipolar disorder in the affected individual. Of the 45 couples who responded, the patients in 16 were participants in the genetic linkage study, the patients in 23 were members of the Depression and Related Affective Disorders Association, and there were three outpatients and three inpatients of the affective disorders unit of the Johns Hopkins University Hospital. The majority of the questionnaires were fully completed; however, some questions were left blank by certain subjects.
The mean age of the respondents with bipolar disorder was 48 years (SD=10.7), and the mean age of the spouses was also 48 years (SD=12.6). Of the respondents with bipolar disorder, 31.1% (N=14) reported a diagnosis of type I disorder, 51.1% (N=23) reported a diagnosis of type II disorder, and 17.7% (N=8) were not sure which subtype of bipolar disorder they had. Most patients (88.9%, N=40) and spouses (82.2%, N=37) were in their first marriage. The number of biological children of patients and spouses ranged from one to six (for both, mean=1.9, SD=1.5). More than one-half of the patients (53.3%, N=24) and spouses (60.0%, N=27) were college graduates.
Knowledge of Rates of Response to Treatment
When asked to estimate what percentage of people with bipolar disorder have a total or excellent response to medical treatment, the mean estimate of the patients was 56.7%, and the mean of the spouses, 52.6%. The patients' mean estimate of the likelihood of having a good response to medical treatment was 61.5%, and the spouses' mean estimate was 59.5%. The mean estimate regarding patients having poor or no response to medical treatment was 25.9% for the patients and 30.3% for the spouses. It has been estimated that 60%–70% of patients with bipolar disorder will have a good response to mood stabilizers such as lithium or anticonvulsants (
1).
Knowledge of Probability of Inheritance
Both patients and their spouses were asked to give their estimate of the probability that a child will inherit a gene for bipolar disorder if one partner but not the other has bipolar disorder. The mean estimate was 46.7% for the patients and 41.4% for the spouses.
Attitudes Toward Genetic Testing for Bipolar Disorder and Disclosure of Genetic Information to Third Parties
The great majority of the subjects with bipolar disorder indicated that they would definitely or probably take a blood test to determine whether they are carrying a gene for bipolar disorder, and the majority of their spouses said that they too would want to know the results of such a test. Of the individuals with bipolar disorder, 85.4% (N=35 of 41) indicated that they would definitely take a blood test to determine whether they are carrying a gene for bipolar disorder, and 14.6% (N=6 of 41) said that they would probably take the test; however, of the spouses, only 46.3% (N=19 of 41) said that they would definitely take the test themselves, and 34.1% (N=14 of 41) said that they would probably take the test, a significant difference (χ2=18.8, df=1, p<0.001). Those spouses who were less certain about whether they would take advantage of genetic testing for bipolar disorder themselves may believe that their risk of carrying a gene is minimal in the absence of any clinical signs or symptoms of bipolar disorder. Furthermore, most of the spouses (85.4%, N=35 of 41) said that they would definitely or probably want to know the results of their affected partner's genetic test. Of note, when gender was looked at separately, there were no statistically significant differences between the responses of male patients and female patients on this issue. There were also no statistically significant differences between male and female spouses.
When the subjects with bipolar disorder and their spouses were asked whether minors (children under age 18) should be tested for a gene for bipolar disorder, the majority of the bipolar patients and the majority of the spouses said that minors should definitely or probably be tested. Among the bipolar individuals (N=40 for this question), 77.5% (N=31) said that minors should definitely or probably be tested, 12.5% (N=5) were uncertain, and 10.0% (N=4) said that they should definitely not or probably not be tested.
There was more of a gradation in respondents' views about testing a fetus. While 43.9% (N=18) of 41 patients and of their spouses said that they would definitely or probably test a fetus, 39.0% (N=16) of the patients and 41.5% (N=17) of the spouses felt that they would definitely not or probably not test a fetus. Respondents also expressed more uncertainty about testing a fetus than about testing minors: 17.1% (N=7) of 41 patients and 14.6% (N=6) of 41 spouses were uncertain about testing a fetus.
When asked about the disclosure of genetic information to third parties, the large majority of patients and spouses indicated that they would want their genetic information to be given to their doctor but not to their insurance company. Of the individuals with bipolar disorder, 75.0% (N=30 of 40) said that they would definitely or probably want researchers to give their genetic information to their doctor, and the majority of their spouses (65.0%, N=26) expressed the same view. When asked whether they would want researchers to give their genetic information to their insurance company, the majority of individuals with bipolar disorder (76.9%, N=30 of 39) and the majority of their spouses (84.6%, N=33), said that they would definitely not or probably not want this to be done.
Overall, patients and spouses were in agreement about their attitudes toward genetic testing and the disclosure of genetic information to third parties.
Benefits and Risks of Having Bipolar Disorder Genetic Information
The bipolar patients and spouses were asked to choose from a variety of reasons for undergoing genetic testing those that they believed were potential benefits of knowing whether they or their spouse carries a gene for bipolar disorder. Of the benefits that they acknowledged, they were asked to mark those that they felt were most important. The majority (67.5%, N=27 of 40) of both patients and spouses indicated that the most important benefit was “to obtain treatment to prevent attacks.” The second most important benefit selected was “I think that I (or my spouse) have the gene, and I want to be more certain of that.” This was ranked most important by 12.5% (N=5) of the patients and by 5.0% (N=2) of their spouses. Both of these potential benefits were ranked more important than “to decide whether or not to have children,” “to decide whether or not to get married,” and “to make financial plans.”
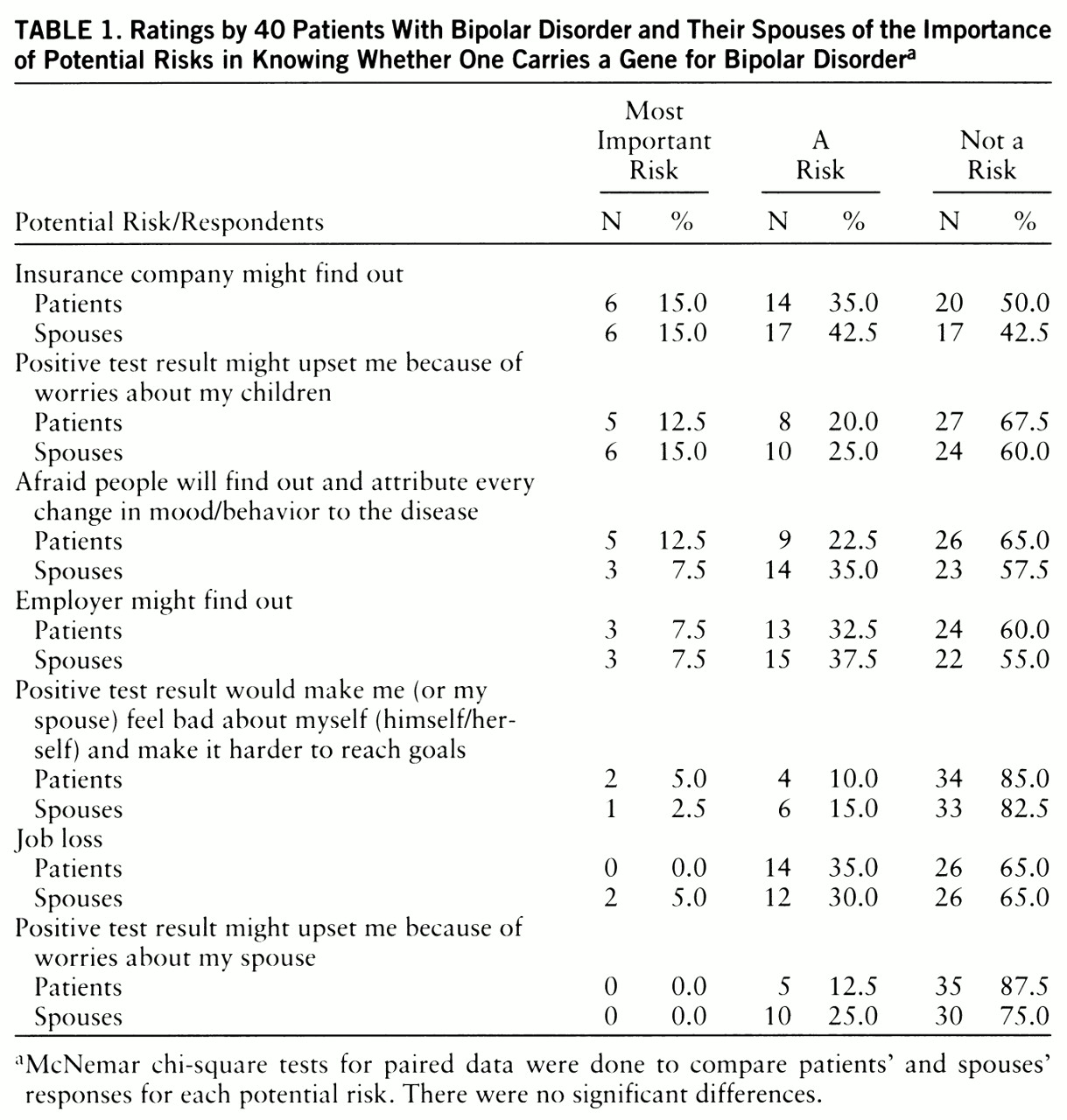
The bipolar patients and their spouses were next asked to choose from a variety of reasons for genetic testing those that they felt were potential risks of knowing whether they or their spouse carries a gene for bipolar disorder. They were also given the option of indicating that there are no real risks of knowing. In addition, of the reasons they acknowledged, they were asked to mark those that they felt were most important. There was less agreement between patients and spouses about the risks of knowing their bipolar disorder genetic information than there was about the benefits of knowing. Responses are shown in
table 1. Twenty-five percent (N=10 of 40) of the patients felt most strongly that there were no real risks of knowing their bipolar disorder genetic information. This response was ranked most important by the patients more frequently than any of the risks that were proposed. Among the patients, the prospect of their insurance company finding out was most frequently selected as the most important risk. Among the spouses, two risks were most frequently selected as most important: the prospect of their insurance company finding out and the prospect that a positive test might upset them because of worries about their children. When gender was looked at separately, there were no statistically significant differences between the responses of male patients and female patients or between those of male and female spouses on any of the questions that addressed potential risks. In addition, there were no significant differences between the attitudes of patients and spouses regarding the relative importance of various benefits and risks of knowing whether one carries a gene for bipolar disorder.
The vast majority of the bipolar patients and their spouses indicated that the benefits of knowing whether they or their spouses carry a gene for bipolar disorder outweigh the risks. None of the respondents said that the risks outweighed the benefits of genetic knowledge. Only 22.0% (N=9 of 41) of the patients and 14.6% (N=6) of their spouses were uncertain. Moreover, there were no statistically significant differences in responses to this question between male patients and female patients or between male and female spouses.
Attitudes Toward Abortion
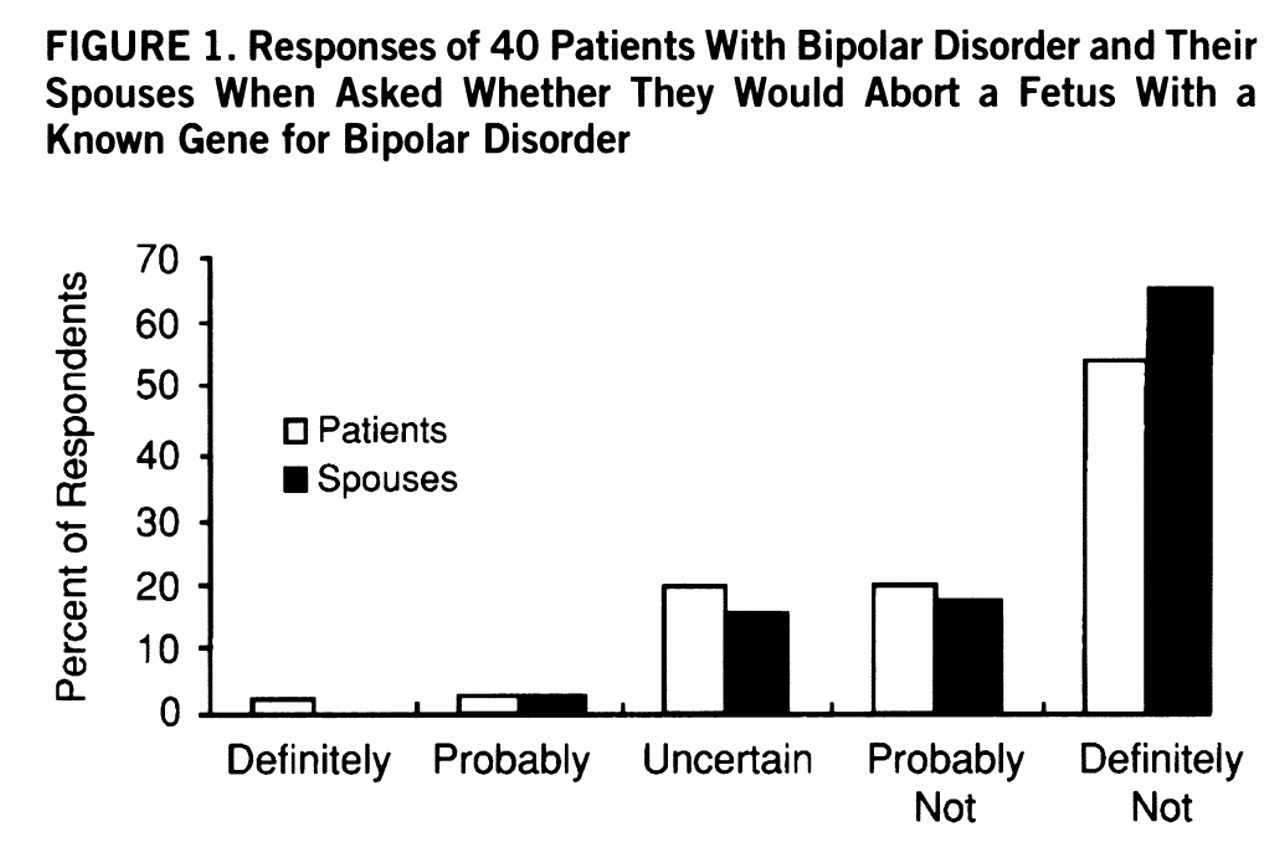
Figure 1 shows patients' and spouses' attitudes toward aborting a fetus that carries a gene for bipolar disorder. When asked about this, the majority of the patients with bipolar disorder, 55.0% (N=22 of 40) and their spouses, 65.0% (N=26) said that they would definitely not abort the fetus.
Patients and spouses were also asked about their attitudes toward abortion under other genetic risk circumstances (e.g., increased genetic risk of a serious, painful or debilitating, incurable neurologic disorder or extreme untreatable obesity). The majority of both the patients and their spouses expressed the opinion that abortion was definitely not or probably not justified in any of these cases. They were most inclined to justify abortion in the case of a serious, painful, and incurable neurologic disorder beginning at age 40, with 22.0% (N=9 of 41) of the patients and 24.4% (N=10) of their spouses indicating that they would definitely or probably choose to abort a fetus that would develop such a condition.
In addition, there were no significant differences in responses to any of the questions regarding abortion between male and female patients or between male and female spouses.
Attitudes Toward Marriage and Childbearing
Most respondents—92.1% (N=35 of 38) of the patients and 78.9% (N=30 of their spouses—said that they would have definitely or probably gotten married even if a blood test had detected a gene for bipolar disorder. In addition, the majority of respondents—55.0% (N=22 of 40) of the patients and 57.5% (N=23) of their spouses—said that knowing that they or their spouse had a gene for bipolar disorder would definitely not or probably not have deterred them from having children.
There were no statistically significant differences between patients' and spouses' predicted attitudes toward marriage and childbearing given this genetic information. However, there was more uncertainty about childbearing than about marriage among both patients and spouses; 17.5% (N=7 of 40) of the patients and 25.0% (N=10) of their spouses were uncertain whether they would have children if they knew that they had a gene for bipolar disorder, compared to 7.9% (N=3 of 38) of the patients and 21.1% (N=8) of their spouses who indicated that they were uncertain whether they would still have gotten married if they knew that they had a gene for bipolar disorder.
When responses to questions about marriage and childbearing were analyzed separately by gender, there were no statistically significant differences between male and female patients or male and female spouses.
DISCUSSION
Our data indicate that attitudes toward presymptomatic and prenatal testing for bipolar disorder were quite positive. The majority of the bipolar patients and their spouses stated that they would want to take advantage of presymptomatic and prenatal genetic tests for bipolar disorder if they became available. Furthermore, the majority of both patients and spouses were in favor of testing minors for the gene. The greatest degree of uncertainty for both patients and spouses involved the testing of a fetus.
Importantly, the vast majority of patients and spouses believed that the benefits of knowing whether they or their spouse carries a gene for bipolar disorder outweigh the risks. The benefit ranked most important by both patients and spouses was to obtain treatment to prevent episodes of illness. Only a small group of patients (10.0%) and spouses (15.0%) felt that knowing that one carried a gene for bipolar disorder would make it harder for that person to reach his or her goals in life.
The overwhelming majority of the bipolar patients and spouses indicated that they would not choose to abort a fetus with a gene for bipolar disorder. Overall, respondents were less likely to justify abortion for carrying a gene for bipolar disorder than they were for carrying a gene for any of the other hypothetical conditions presented. This is in agreement with a study by Smith et al. (
15) which showed that members of bipolar disorder support groups, psychiatric residents, and medical students would all be more inclined to abort a fetus for another life-threatening or severely debilitating disorder than they would for bipolar disorder. However, compared to our patient and spouse groups, a greater percentage of their respondents indicated that they would end a pregnancy if the fetus were to definitely develop an unspecified course of bipolar disorder. This may be because our question left open the possibility that an individual may in fact have a gene for bipolar disorder but not develop any clinical symptoms. (When asked to estimate the likelihood that one could have a gene for bipolar disorder but not show any signs of the disorder at all, our patients gave a mean estimate of 31.7%, and the spouses gave a mean estimate of 30.5%.) Smith et al. also found that the intention to abort a fetus would be influenced by the projected severity of the illness and the likelihood of developing bipolar disorder. However, given the multifactorial nature of bipolar disorder, it is possible that a positive result of a genetic test for the disorder would still leave uncertainty about whether one will in fact develop the disorder. In addition, a positive genetic test result might not provide information about the severity of the illness.
It is interesting to note that there were no significant differences between the attitudes of patients and those of their spouses toward most of the issues addressed.
The relatively high rate of uncertain responses regarding childbearing, prenatal testing, and abortion indicate areas in which patients and spouses perceive a need for more information.
This was a pilot study, and several limitations may have influenced our results. First, we had a 50% response rate to our questionnaire, which is comparable to the general response rate for medical questionnaires (
17). Another limitation of the study was the small size of the study group. Trends that did not reach statistical significance in our study might well have reached significance with a larger group. In addition, it is apparent that our subject group was in some respects quite skewed; ascertainment was not systematic, and most respondents were well-educated and in their first marriage. The patients in their first marriage may represent those whose illness has caused less marital disruption. Most of the patient respondents were members of support groups or participants in a genetic study and would be expected to be better-educated and more willing to disclose personal information about the genetics of their disease.
Our study did not explore the length of time that affected individuals had been treated for bipolar disorder or how efficacious their treatment had been. These factors would be expected to affect attitudes toward marriage, childbearing, and disclosure of genetic information. In addition, we had no method of ensuring that patients were euthymic at the time that they completed the questionnaire. Finally, we had no normal (nonclinical) control group.
Despite the limitations of the study, the results are of considerable interest and value in terms of providing a basis for further research. The trends we observed suggest a strong likelihood that individuals will make use of genetic tests for bipolar disorder once they become available. In addition, they convey attitudes that may shed light on some of the concerns that have been raised regarding the possible misuse of genetic information. However, we must be careful about extrapolating from hypothetical intentions to actual requests for genetic testing. In the case of Huntington's disease—an incurable, genetic (autosomal dominant) neuropsychiatric degenerative disease for which genetic testing is now available—the current demands for testing are substantially below the rate predicted by early surveys (
18,
19). A study by Quaid and Morris (
20) surveyed 66 people at risk for Huntington's disease who chose not to undergo testing for the disorder. The five most important reasons that they cited for declining testing were lack of a treatment, increased risk to their children, the prospect of losing health insurance, financial costs of testing, and “the inability to undo the knowledge.”
The discovery of a genetic test for bipolar disorder will inevitably raise some similar concerns, but bipolar disorder differs in many respects from Huntington's disease. The availability of treatment, high rates of response to treatment, and aspects of the illness that might confer advantages to the individual, to interpersonal relationships, and to society may outweigh the potential disadvantages at the time of actual testing (
1,
9–
12).
Additional studies with larger study groups and broader sampling of the population would be useful. It would be informative to address the issue of how the degree of accuracy of a genetic test for bipolar disorder would influence people's attitudes toward testing. It is not clear how much genetic information will be required to justify making a genetic test for bipolar disorder available. Careful consideration must be given to the issue of testing minors. The question of whether parents' desire to know that their child has a gene for bipolar disorder outweighs the child's right to privacy—particularly if such knowledge could lead to earlier treatment and avoiding potential harm to the child—remains to be answered. Related issues, such as circumstances under which it might be permissible to deny testing to individuals and whether there might ever be circumstances that warrant mandatory testing, have already become real issues in the genetic testing for Huntington's disease (
21) and will undoubtedly have to be addressed in future testing for bipolar disorder. Data from continuing research on the issues identified here will be essential in facilitating the development of appropriate guidelines for the eventual genetic testing for bipolar disorder.