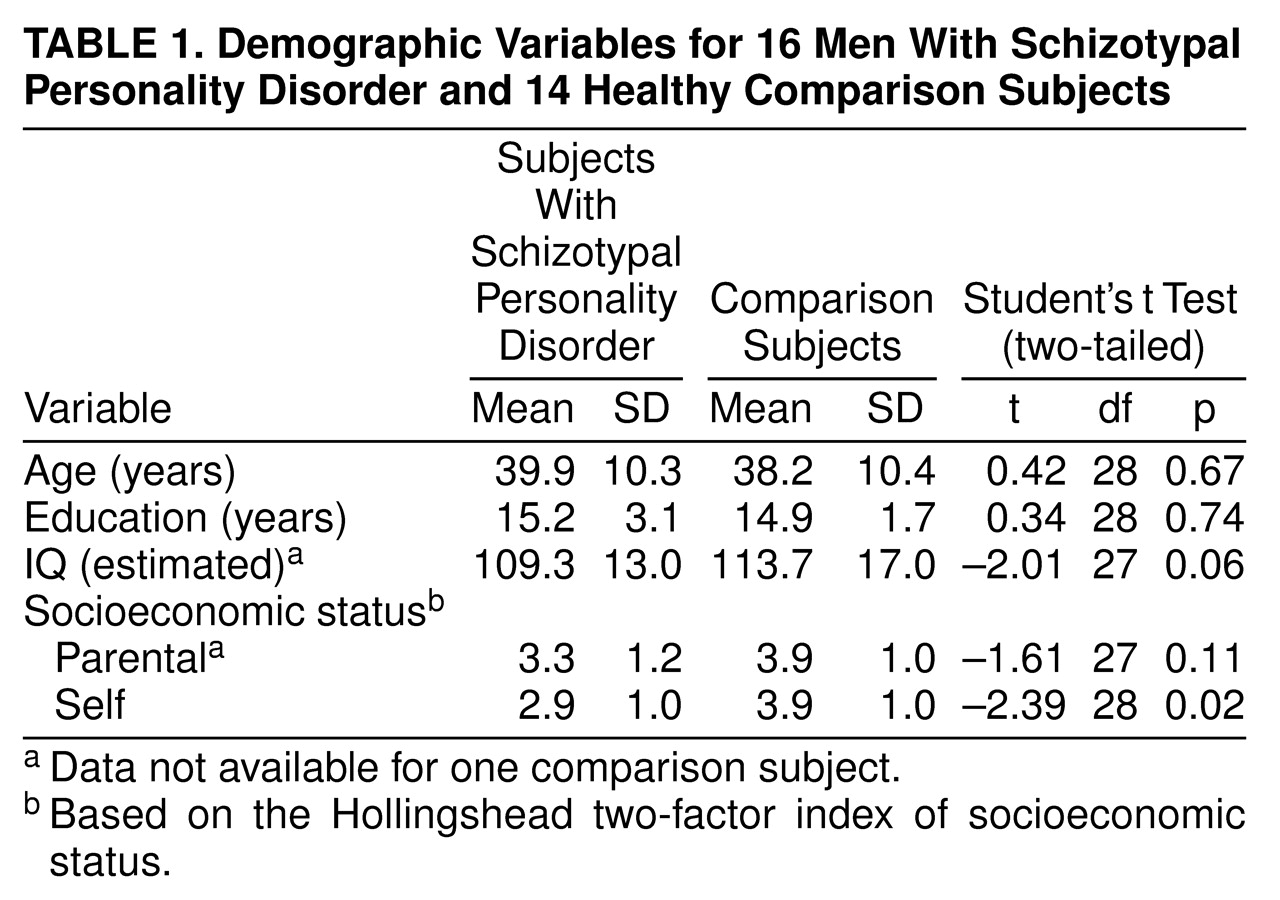
One approach to obtaining insight into schizophrenia is to examine nonschizophrenic disorders that are in the schizophrenia spectrum. For example, data indicate that schizotypal personality disorder has the same genetic diathesis as schizophrenia; the risks of schizophrenia in a sibling of a proband with schizotypal personality disorder and a sibling of a proband with schizophrenia are the same
(1–
4). Schizotypal personality disorder is thus an ideal spectrum disorder to study because subjects with this disorder often have not been treated with neuroleptics. In addition, persons with schizotypal personality disorder have not experienced the possible complicating effects of a chronic illness, including hospitalization, nor the stress of a long-term illness, which may result in glucocorticoid-induced cell morphological changes
(5,
6). Environmental richness and nutrition, which may be different in the chronically ill, have also been demonstrated to affect cellular morphology
(5,
6). There is also the further possibility that, by examining similarities and differences of neuroanatomical abnormalities in schizotypal personality disorder and schizophrenia, one can not only observe endophenotypic similarities but also perhaps determine what additional features in schizophrenia relate to an overtly psychotic course and/or what features in schizotypal personality disorder may protect against overt psychosis.
Our initial examination of individual temporal lobe regions of interest in schizotypal personality disorder
(7) demonstrated smaller volume of the left superior temporal gyrus gray matter than in comparison subjects and an abnormal parahippocampal asymmetry. However, we did not find the markedly abnormal volumes for the medial temporal lobe that are often noted for schizophrenia. These findings are compatible with the hypothesis that abnormalities of the left superior temporal gyrus are a consistent anatomic component of the schizophrenia spectrum disorders, as found in several studies of schizophrenia
(8–
14), which we have reviewed elsewhere
(15–
17). A study
(18) of subjects with features of schizotypy (but not clinical schizotypal personality disorder) indicated a prefrontal volume deficit (involving a region and subject pool not evaluated by our group), suggesting that there may be an abnormality of the frontotemporal connection and/or that abnormalities in schizotypal personality disorder may be more widespread. These reports, however, suggest the possibilities that the abnormalities in schizotypal personality disorder may be more widespread than the temporal lobe and that any abnormalities in the frontal and temporal regions might also have an abnormality of the frontotemporal connection. As discussed in our reviews
(15–
17), one of the recurring issues in magnetic resonance imaging (MRI) studies of schizophrenia is the degree to which abnormalities are circumscribed or widespread throughout the brain. Thus, we decided to evaluate whether schizotypal personality disorder involves global anomalies in CSF, gray matter, cortical gray matter, and/or white matter. We here report larger than normal CSF volumes not attributable to large lateral ventricles.
RESULTS
A repeated measures ANOVA comparing the subjects with schizotypal personality disorder and the comparison subjects on the three tissue classes (gray and white matter and CSF) revealed a statistically significant main effect of diagnosis (F=4.69, df=1, 28, p=0.04). There was no statistically significant main effect of tissue class (F=0.74, df=1.34, 56, p=0.43). There was, however, an interaction between diagnosis and tissue class (F=3.97, df=1.34, 56, p=0.04). When cortical gray matter, instead of total gray matter, was entered into the analysis, the results were not meaningfully changed: there was still a main effect of diagnosis (F=4.28, df=1.00, 28, p=0.05) and an interaction between diagnosis and tissue class (F=4.15, df=1.30, 56, p=0.04) but no main effect of tissue class (F=0.65, df=1.30, 56, p=0.47).
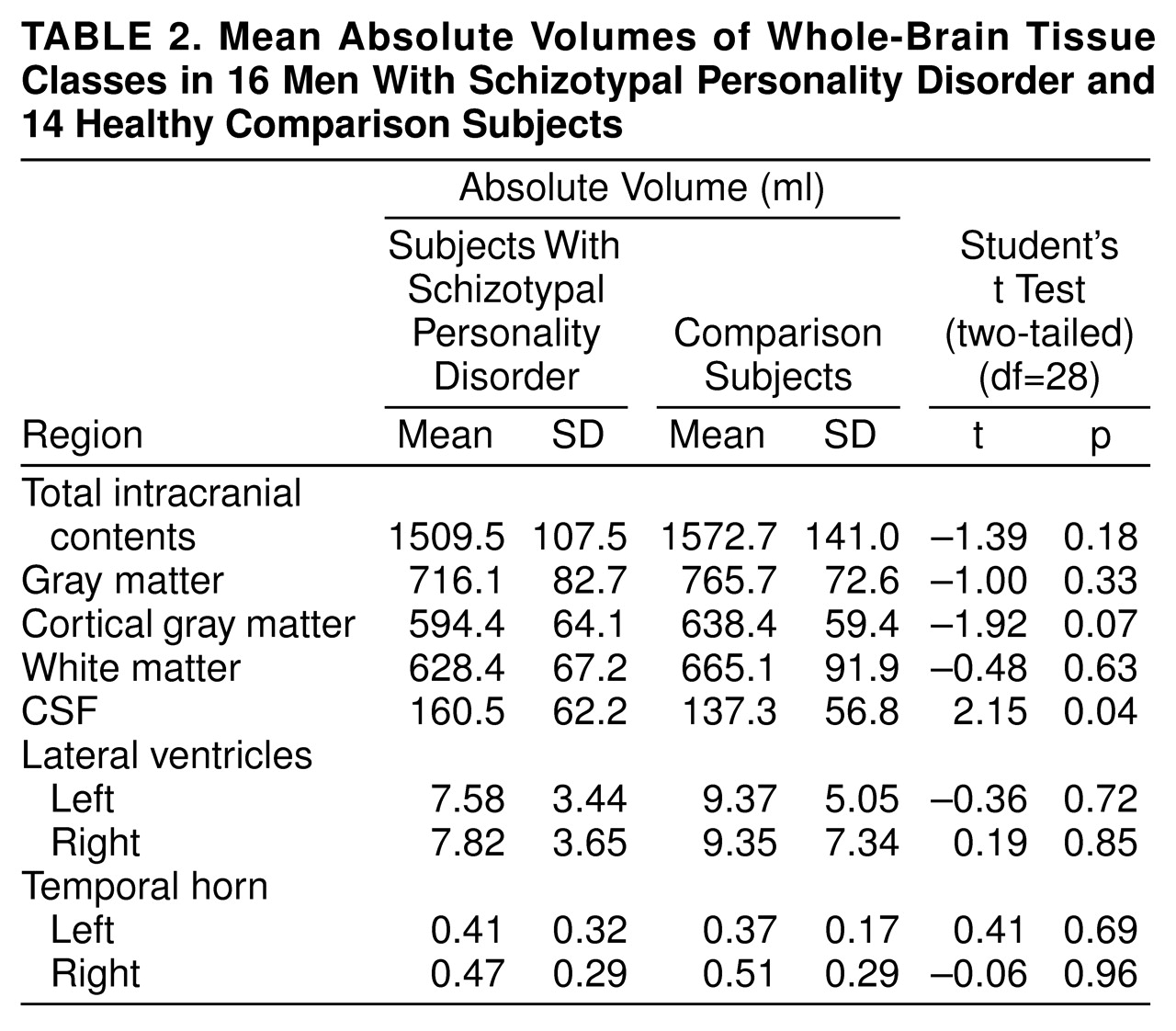
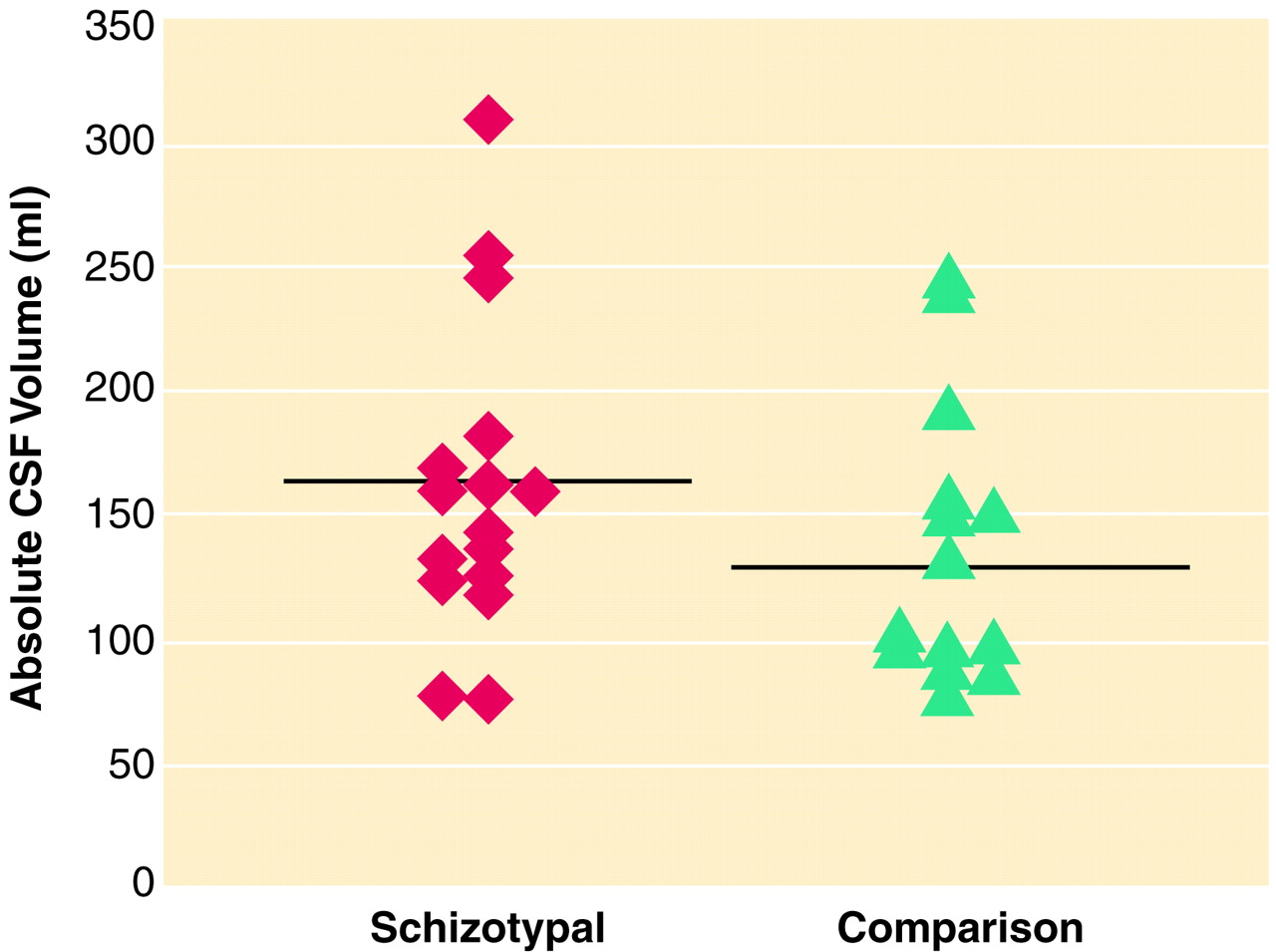
The planned contrasts demonstrated that the CSF volumes were larger in the subjects with schizotypal personality disorder than in the comparison subjects (
table 2 and
figure 2). To determine whether the difference in CSF volume was driven by differences in the lateral ventricles, t tests were performed. There was no difference in the left or right lateral ventricle or in the left or right temporal horn. The range of the volumes of the left ventricle for the comparison subjects was 17.9 ml, whereas it was 13.7 ml for the subjects with schizotypal personality disorder. Two of the comparison subjects had large ventricular volumes. When these two subjects were removed from the analysis, the difference in ventricular volumes between the schizotypal and comparison subjects still lacked statistical significance. Subarachnoid CSF volume accounted for the difference in total CSF, as whole-brain CSF minus ventricular CSF remained significantly larger in the schizotypal group (t=2.69, df=28, p=0.01).
There was no difference between the two groups in overall intracranial contents (
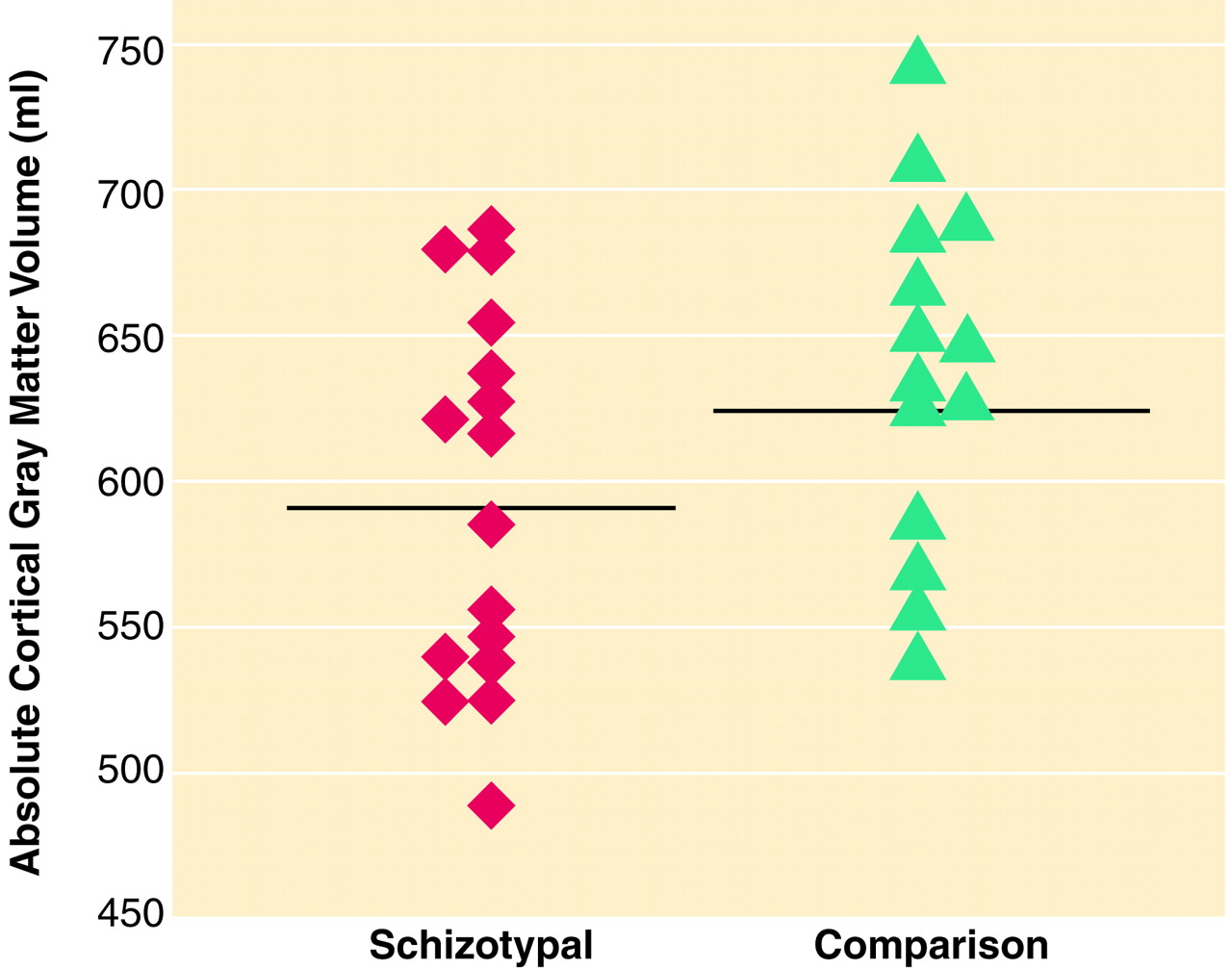
table 2). In addition, there was no difference between the comparison and schizotypal subjects in gray matter or in white matter. However, the subjects with schizotypal personality disorder had a smaller cortical gray matter volume, although the difference was not quite statistically significant (effect size=0.78, percentage difference=7.1%) (
table 2 and
figure 3). On the basis of this effect size, a power analysis suggests that fewer than 30 subjects per group would be needed to demonstrate a statistically significant difference in cortical gray matter volume.
DISCUSSION
In this study of whole-brain measures in subjects with schizotypal personality disorder, ANOVAs demonstrated a main effect of diagnosis and an interaction between diagnosis and the brain’s three main tissue classes. Follow-up planned comparisons showed larger CSF volume in the schizotypal subjects than in normal comparison subjects. As lateral ventricle size did not differ, this difference in CSF volume derived from other sources. In addition, there was also a nonsignificantly smaller (p=0.07) cortical gray matter volume with a moderate to large effect size (0.78), suggesting that an increase in the subject number would result in statistically significant differences between groups in total cortical gray matter.
These data suggest that the abnormalities in schizotypal personality disorder are not confined to the temporal lobe
(7) but may be more widespread. As subarachnoid CSF accounts for the major portion of the nonventricular CSF (about 87% of whole-brain CSF)
(9), we think it likely that this component is larger than normal, a finding consistent with results of a previous computerized tomography (CT) study
(27). The most likely reason for a large CSF volume is a small volume of underlying gray or white matter. Our findings of no difference in white matter but smaller than normal cortical gray matter (although not statistically significant) suggest it may be primarily this latter component. Nonetheless, additional studies of gray matter volume in different cortical regions will be required to determine whether the larger CSF volume is accompanied by diffusely small gray matter volume or is better characterized by disproportionate abnormalities among regions, as has been true in the great majority of studies of schizophrenia (86%)
(15–
17).
In an important MRI study
(28) examining the possible role of genetics in overall brain morphology, schizophrenic subjects and their siblings—10% of whom had schizotypal personality disorder—were shown to have smaller cortical gray matter volumes and larger sulcal CSF volumes. However, only the schizophrenic subjects had large lateral ventricles and concurrently small white matter volumes. The authors hypothesized that genetics contributed to the small cortical gray matter volume and that psychotic illness effects or “nonshared causative effects” contributed to the large ventricular volumes
(28). Their finding is similar to ours: the subjects with schizotypal personality disorder showed a tendency for smaller cortical gray matter, no abnormality in ventricular volume, but a significantly larger than normal subarachnoid CSF volume.
Also, consistent with the preceding hypothesis, Buchsbaum and co-workers
(29) showed no abnormality in lateral ventricle size in subjects with schizotypal personality disorder. However, they did find large temporal horns in those subjects. Possible reasons for the difference in temporal horn findings are their 1) use of a clinic population, 2) inclusion of both men and women, 3) inclusion of both right- and left-handed subjects, 4) use of axial images rather than coronal images, and 5) different tracing procedures. Indeed, only one study
(30) showed high ventricle-brain ratios (VBRs) in subjects with schizotypal personality disorder, although these subjects may have VBRs intermediate between those of schizophrenic and comparison subjects
(31) and larger VBRs than those of nonaffected siblings
(32).
Overall, although there are differences in the technology used, populations sampled, and brain regions measured, there appears to be an emerging consensus from the literature. In terms of global measures, schizotypal personality disorder appears to be associated with large CSF volume and, possibly, small cortical gray matter volume. The exact area of the large CSF volume may differ among studies, and more work is needed to understand these differences.
The nonnormal distribution of CSF volume demonstrated in this study may not be unusual as a skew toward the right (toward higher values) has also been reported in chronic schizophrenia
(33). Thus, in the schizophrenia spectrum disorders, the skew toward higher values may reflect a severity factor affecting CSF volume. Although the reported CSF volume for this comparison group was not statistically different from a normal distribution, there are literature reports of a “tail” of higher CSF values in the general population
(34), where mean CSF volume is usually between 130 and 140 ml
(35,
36). Our mean value of 137 ml and our finding that two comparison subjects had CSF volumes 100 ml above the mean are consistent with these reports.
Moreover, the size of the lateral ventricles may also vary greatly in the general population. In a postmortem study of 183 grossly normal brains
(37), the mean lateral ventricle size was 7 ml and the range was 2 to 39 ml, values that are consistent with our current findings of large lateral ventricles in two comparison subjects. No history of head trauma or developmental abnormalities was noted for either subject. (Removing these two normal subjects from the analysis had no effect on the absence of a statistically significant difference in lateral ventricle size between the schizotypal and comparison subjects.) The present data thus appear compatible with literature reports of variability of CSF and ventricle size in the general population and with a tendency for distributions to be skewed toward higher values.
Although there was no difference in total gray matter volume between the two groups, when total gray matter was more carefully delineated into cortical gray matter only, the subjects with schizotypal personality disorder showed nonsignificantly smaller volumes. In studies of schizophrenia, measurements of gray matter have yielded conflicting results: some studies have demonstrated a smaller than normal total gray matter volume
(38–
40) or cortical gray matter volume
(39,
41,
42) and others have not
(9,
10,
13,
43). From our review of such studies
(15–
17), however, the evidence suggests a nonuniform distribution of gray matter volume deficits in schizophrenia, i.e., that the deficits are greater in some areas than in others. One CT study
(30) of subjects with personality disorders in the schizophrenia spectrum (the majority of whom had schizotypal personality disorder) used a visual scale to show “cortical atrophy” (greater sulcal prominence), which likely is compatible with our finding of larger than normal subarachnoid CSF volume.
The ability to generalize these findings to all persons with schizotypal personality disorder is limited by the relatively small number of subjects and the use of only male subjects. Future plans include the study of female subjects. Drawing subjects from the community may yield subjects less severely affected than in clinic groups but has the important advantage of finding subjects not yet exposed to neuroleptics or other psychotropic medications. In addition, these data do not address the issue of whether the abnormalities are neurodevelopmental and/or degenerative in nature, as this was not a longitudinal study designed to study changes over time.
The finding of larger than normal overall CSF volume and suggestive evidence for smaller cortical gray matter volume, taken together with previous findings of focal deficits in the temporal lobes of the same subjects, suggest that neuroanatomic abnormalities in schizotypal personality disorder may be present in widespread locations but may be greater in some regions than in others, not unlike what is seen in schizophrenia
(15–
17).