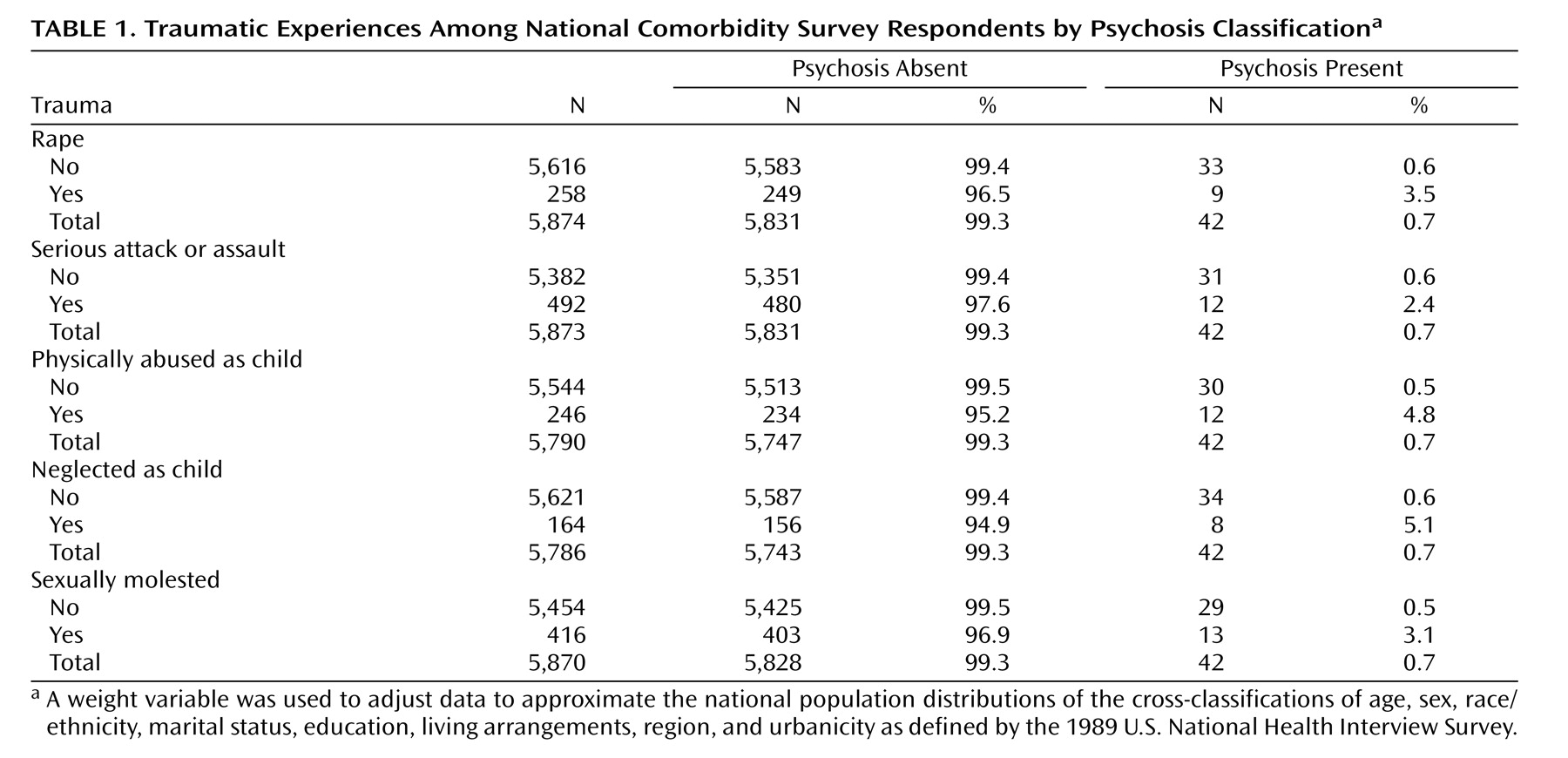
The traumatic experiences and psychosis classifications of the National Comorbidity Survey respondents are presented in
Table 1 . All analyses were conducted using hierarchical binary logistic regression in SPSS 11.0 where the model was built sequentially, retaining only those variables that were significant in each block. The following background variables were used as predictors in the first block: gender, age, depression (lifetime prevalence), family history (two variables were used to represent lifetime prevalence of depression in respondent’s mother and father), urbanicity (a binary variable representing urban or nonurban location), and income (four-category variable). The only significant predictor was depression (odds ratio=9.74, 95% CI=5.14–18.47; z=48.75, p<0.001). The trauma variables were entered in the second block, and physical abuse was the only significant predictor (odds ratio=2.68, 95% CI=1.11–6.52; z=4.76, p=0.03), although all the odds ratios were similar in magnitude and direction ranging from 1.50 to 2.68. The difference in model fit between a logistic model with all the odds ratios constrained to be equal and another in which each variable had a unique effect was not statistically significant (Δχ
2 =0.714, Δdf=4, p=0.94), indicating significant homogeneity among the effects of the trauma variables. The estimated common odds ratio for all variables was statistically significant (odds ratio=1.80, 95% CI=1.51–2.14; z=42.90, p<0.001). In the third block, five gender-by-trauma interactions were included, and the gender-by-rape interaction was found to be significant. The final model indicated that psychosis could be predicted by depression (odds ratio=5.09, 95% CI=2.99–8.66; z=36.06, p<0.001), physical abuse (odds ratio=3.45, 95% CI=1.90–6.25; z=3.45, p<0.001), and the gender-by-rape interaction (odds ratio=1.58, 95% CI=1.15–2.18; z=1.58, p<0.001). With depression removed from the model, the effects for physical abuse (odds ratio=4.49, 95% CI=2.47–8.12; z=24.56, p<0.001) and the gender-by-rape interaction (odds ratio=1.88, 95% CI=1.37–2.59; z=15.15, p<0.001) were slightly higher. To interpret the interaction, the same analysis was rerun separately for male and female subjects (after replacing the interaction term with only the rape variable). The effect for the rape variable was statistically higher for male subjects (odds ratio=5.81, 95% CI=1.24–27.17; z=4.99, p=0.02) than female subjects (odds ratio=4.05, 95% CI=2.02–8.08; z=5.67, p<0.001). With depression removed the effects for male subjects (odds ratio=8.19, 95% CI=1.85–36.32; z=7.66, p=0.01) and female subjects (odds ratio=5.65, 95% CI=2.87–11.10; z=25.30, p<0.001) were slightly higher.
To examine the cumulative effect of traumas, psychosis was regressed on an aggregate variable created to represent the number of traumatic events experienced by each respondent (0, 1, 2, and ≥3). The aggregate trauma variable was entered as a categorical predictor in the second block of a logistic regression, with depression entered in the first block. The first level (no traumatic experiences) was used as a reference category for a simple contrast. The odds ratios for one traumatic experience (odds ratio=2.12, 95% CI=1.13–3.99; z=5.46, p=0.02), two experiences (odds ratio=3.89, 95% CI=1.83–8.28; z=12.41, p<0.001), and three or more experiences (odds ratio=7.96, 95% CI=3.91–16.17; z=32.86, p<0.001) indicated an increasing likelihood of psychosis as the number of trauma types experienced increased.