Buprenorphine is an opioid medication typically prescribed for treating opioid use disorder. However, literature supports its utility for treatment-resistant depression (
1). Buprenorphine has a unique method of action: it is a partial agonist of mu opioid receptors and an antagonist of kappa and delta opioid receptors (
2). Recent research shows that the kappa opioid receptor’s role is crucial in buprenorphine’s function as an antidepressant (
3). Acute administration of kappa opioid receptor antagonists has been shown to produce antidepressant effects, while agonists exhibit prodepressive effects (
3).
The function of buprenorphine as an antidepressant is intriguing, since it is common for patients with substance use disorders to have a co-occurring mood disorder. One study found that in patients with a substance use disorder, 53% had a comorbid psychiatric illness (
4). Additionally, patients with co-occurring substance use and mood disorders have a higher risk of suicide (
5). Health care professionals often categorize such patients as "substance abusers" or "drug seekers," which minimizes the impact of their mood disorder and impedes its treatment (
6). We present a case of co-occurring disorders, in which buprenorphine-naloxone fulfilled both its prescribed purpose of treating opioid use disorder while also treating the patient’s severe depression.
Case
A 47-year-old Caucasian man with a history of depression and polysubstance abuse, including a significant history of prescription opioid abuse, presented to our emergency department after ingesting hardware nails, requiring foreign body removal. While in the emergency department, it became clear that the patient had suicidal intent, and psychiatric services were called. He reported worsening feelings of anhedonia and hopelessness for an unspecified period of time, as well as insomnia and escalating suicidal ideation over the past several days. He exhibited symptoms of opioid withdrawal, including mydriasis, rhinorrhea, myalgia, anxiety, gastrointestinal cramps, and restlessness and anxiety. He disclosed that he had been using prescription opioid medications for more than a decade, originally prescribed for pain while serving in the military, which eventually led to opioid use disorder. He had poor insight, loss of interest, low energy, poor eye contact, and was disengaged during conversations with his health care team. He was involuntarily admitted to the inpatient psychiatric unit of our behavioral health center as a result of his suicidal ideation and impulsive behavior.
The patient’s psychiatric history included seven previous hospitalizations after suicide attempts. He was originally diagnosed with depression in 2010, although he believed that he had depression for many years before his diagnosis. Additionally, he had a history of foreign body ingestion, including nails and lithium batteries. During previous inpatient hospitalizations, he underwent multiple medication trials, including sertraline, quetiapine (300 mg/day), fluoxetine (40 mg/day), and methadone (40 mg b.i.d.). Throughout these trials, he reported little to no benefit, and after many months he became nonadherent to the medications. He endorsed periods during which he was not using opioid medications but still experienced severe depressive symptoms. As a result, he was given the tentative diagnosis of treatment-resistant depression. However, this diagnosis was preliminary, because medication adherence could not be confirmed.
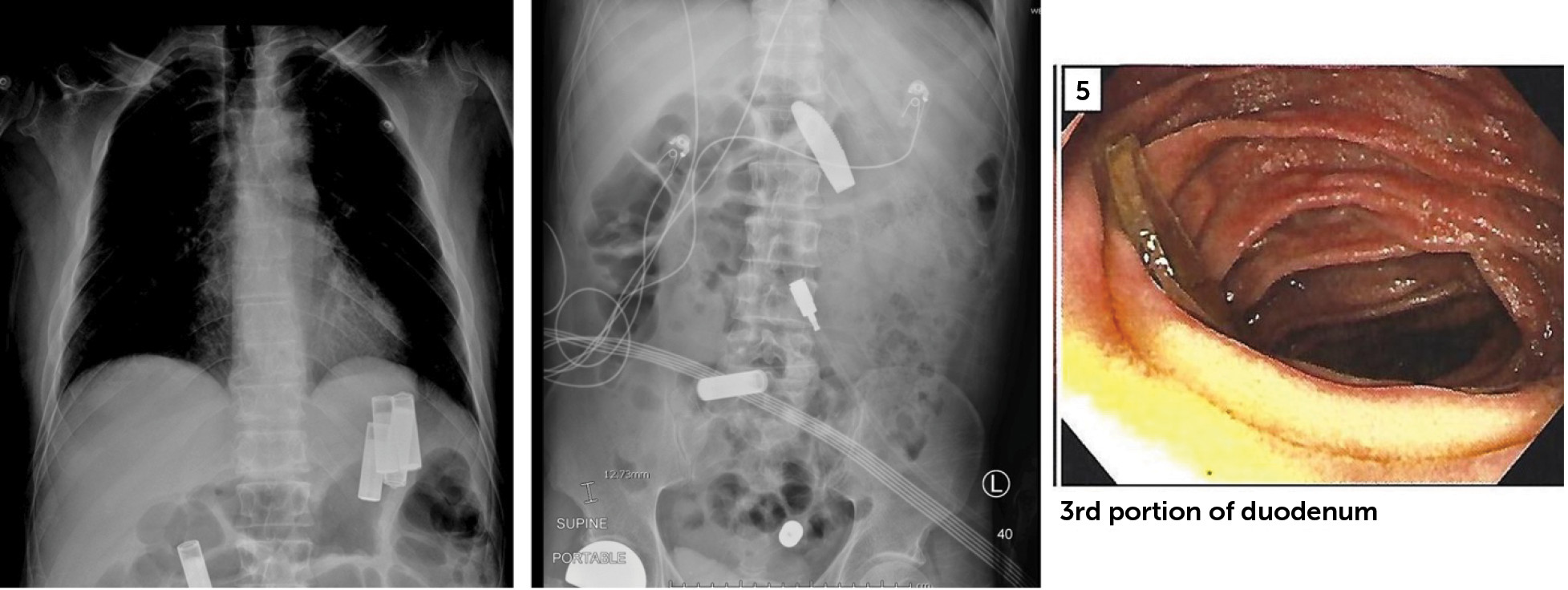
Throughout the first weeks of the patient’s treatment on the inpatient unit, he remained withdrawn, refusing to participate in any group activities or to engage with any of the other patients. He would not comply with vital sign checks and frequently became combative and disagreeable. He could not identify any goals for his treatment and had little to say when approached. While on the unit, he ripped out his IV, shoving the needle into his stomach, and swallowed batteries and a plastic knife. Endoscopy was required to retrieve the foreign bodies, which were lodged in his stomach and bowel (
Figure 1).
His initial treatment included valproic acid (500 mg b.i.d.) as a result of unwitnessed seizures and to provide a mood-stabilizing effect, but he denied improvement, reporting continual suicidal ideation, anhedonia, and hopelessness, spending most of his time in his room lying supine on the bed.
Approximately 2 weeks into his treatment with valproic acid, he was evaluated for treatment with buprenorphine-naloxone, which was deemed appropriate because of the patient’s opioid use disorder and chronic pain. He was initially prescribed buprenorphine-naloxone in the morning (4 mg–1 mg), afternoon (4 mg–1 mg), and night (4 mg–1 mg), with the dosages later adjusted to 8 mg–2 mg, 2 mg–0.5 mg, and 2 mg–0.5 mg, respectively. The patient reported alleviation of his withdrawal symptoms and improvement in his chronic pain, with no notable side effects. In addition, he exhibited an instantaneous change in behavior, becoming adherent with his medications, complying with vital sign checks, and attending some of the group activities on the unit. He became more outgoing and personable and went on to attend group sessions voluntarily, even leading several activities himself.
The patient started engaging more with his care team and became open to possible changes to his medications. Although he had experienced improvement in his depression, fluoxetine was added in the third month of treatment to reduce residual depressive symptoms. The initial regimen was 20 mg/day, which was increased to 20 mg b.i.d. Two weeks before his hospital discharge, he was started on quetiapine to provide mood stabilizing effects. At this time, it was noted that he had a shift in his views toward medication-assisted therapy. Previously, he had discussed his disdain for psychotropic medications; however, after buprenorphine-naloxone treatment during this hospitalization, he disclosed that he felt that the medication was helpful and desired to continue his regimen.
The patient spent a total of 5 months on the inpatient unit. Upon discharge, he was found to have improved insight and judgment and no suicidal ideation and was optimistic and goal-oriented. He helped to develop his own aftercare plan, conducting a significant portion of the research on his own. He was discharged on buprenorphine-naloxone (morning, 8 mg–2 mg; afternoon, 2 mg–0.5 mg; and night, 2 mg–0.5 mg), fluoxetine (20 mg b.i.d.), and quetiapine (200 mg/day), with plans to follow up with outpatient psychiatry. Two weeks after his discharge, a member of his treatment team spoke with his mother via telephone, who reported that he was doing well.
Discussion
The above patient was prescribed buprenorphine-naloxone to treat his opioid use disorder. However, his depressive symptoms concordantly improved. This was not entirely unexpected, since buprenorphine-naloxone has been prescribed off-label as a treatment for patients with depression that does not respond to treatment with two or more different classes of antidepressants (
7).
Our patient’s treatment with buprenorphine-naloxone led to rapid amelioration of his mood, allowing him to engage openly with his care team. By relieving his anhedonia and hopelessness, the medication enabled him to advocate for himself. His treatment team recognized the opportunity to engage with him and collaborate toward improvement in his mental health, causing his treatment to become solely patient-centered.
These results demonstrate the potential benefits of buprenorphine-naloxone as a treatment modality for treatment-resistant depression. One benefit of this medication is that it can be prescribed in various forms, such as sublingual tablets, long-acting injectables, and implants. Additionally, it has a low side-effect profile, and it is safe for use with elderly patients and for patients with renal dysfunction (
8). However, there is some potential for abuse, particularly when buprenorphine is administered alone, although the addition of naloxone helps to minimize this risk (
8,
9). In addition, there is a risk for overdose when co-administered with benzodiazepines (
9).
Buprenorphine has been shown to decrease suicidal ideation in patients who are severely suicidal. Yovell et al. (
10) showed that buprenorphine significantly reduced suicidal ideation in patients with severe suicidal ideation without substance abuse, as measured with the Beck Scale for Suicide Ideation. This effect was observed within 2 weeks, which is faster than that of conventional selective serotonin reuptake inhibitors.
Studies have shown that patients treated with buprenorphine exhibit significant improvement in depressive symptoms, as measured with the Hamilton Rating Scale for Depression (HAM-D), specifically with reduction in depressed mood, fatigue, and hopelessness (
1). These improvements in depressive symptoms have been reported to occur within 48 hours of the first buprenorphine-naloxone dose and maintained throughout the course of treatment (
1). Research also shows that while buprenorphine-naloxone causes a significant decline in depression severity during treatment, if discontinued suddenly, there is a significant increase in depressive levels (
8).
A similar drug combination of buprenorphine/samidorphan has been shown to achieve this effect. One study demonstrated that patients with depression who had an insufficient response to SSRIs experienced significant improvement in several depression outcome measures, including scores on the HAM-D, the Montgomery-Åsberg Depression Rating Scale, and the Clinical Global Impression Scale (
11).