Patient Characteristics
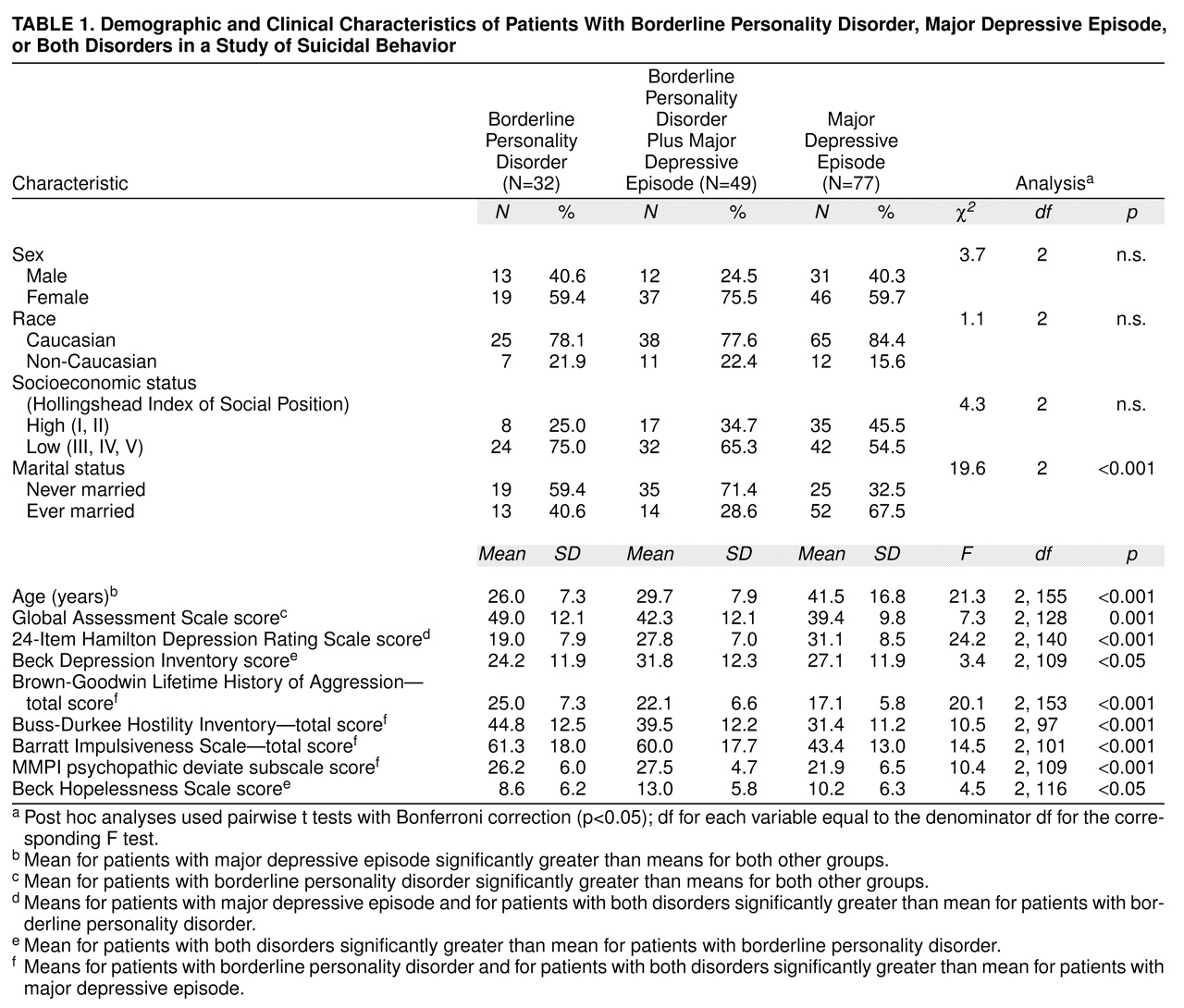
The study group consisted of 158 patients, 81 patients with borderline personality disorder and 77 with major depressive episode (
table 1). They ranged in age from 18 to 83 years. Although the depressed group was defined to exclude patients with any cluster B disorder, the group with borderline personality disorder, by design, included many patients with comorbid major depressive episode. Among the 81 patients with borderline personality disorder, 49 patients had comorbid major depressive episode and 32 did not. Additional frequent axis I diagnoses among patients with borderline personality disorder included adjustment disorder (11 patients, 34.4%) and dysthymic disorder (five patients, 15.6%). The group with major depressive episode only consisted of 31 men and 46 women, and the group with borderline personality disorder consisted of 25 men and 56 women. There were no significant differences between groups in gender, race, or socioeconomic status as measured by using the Hollingshead Index of Social Position (classes I and II, high social position, versus classes III–V, low social position). The depressed patients were significantly older than the patients with borderline personality disorder, and those with both disorders and had a higher proportion who had “ever married,” which was a function of age.
The depressed patients and the patients with comorbid disorders had significantly greater observer-rated depression (Hamilton depression scale) and lower (more impaired) scores on the GAS compared to patients with borderline personality disorder (
table 1). The group with both disorders had the highest self-rated depression scores on the Beck Depression Inventory and Beck Hopelessness Scale; their scores were significantly higher than patients with borderline personality disorder but were not significantly different from those of depressed patients.
Patients with borderline personality disorder and patients with both disorders had higher scores on all measures of impulsive aggression compared to the depressed patients. For each measure of impulsive aggression, the mean difference in scores between the group with borderline personality disorder and the group with comorbid disorders, on the one hand, the depressed group, on the other, was significant (according to a post hoc pairwise t test with Bonferroni correction, p<0.05). However, the mean difference between the scores for the group with borderline personality disorder and the group with comorbid disorders was not significant.
Suicidal Behaviors
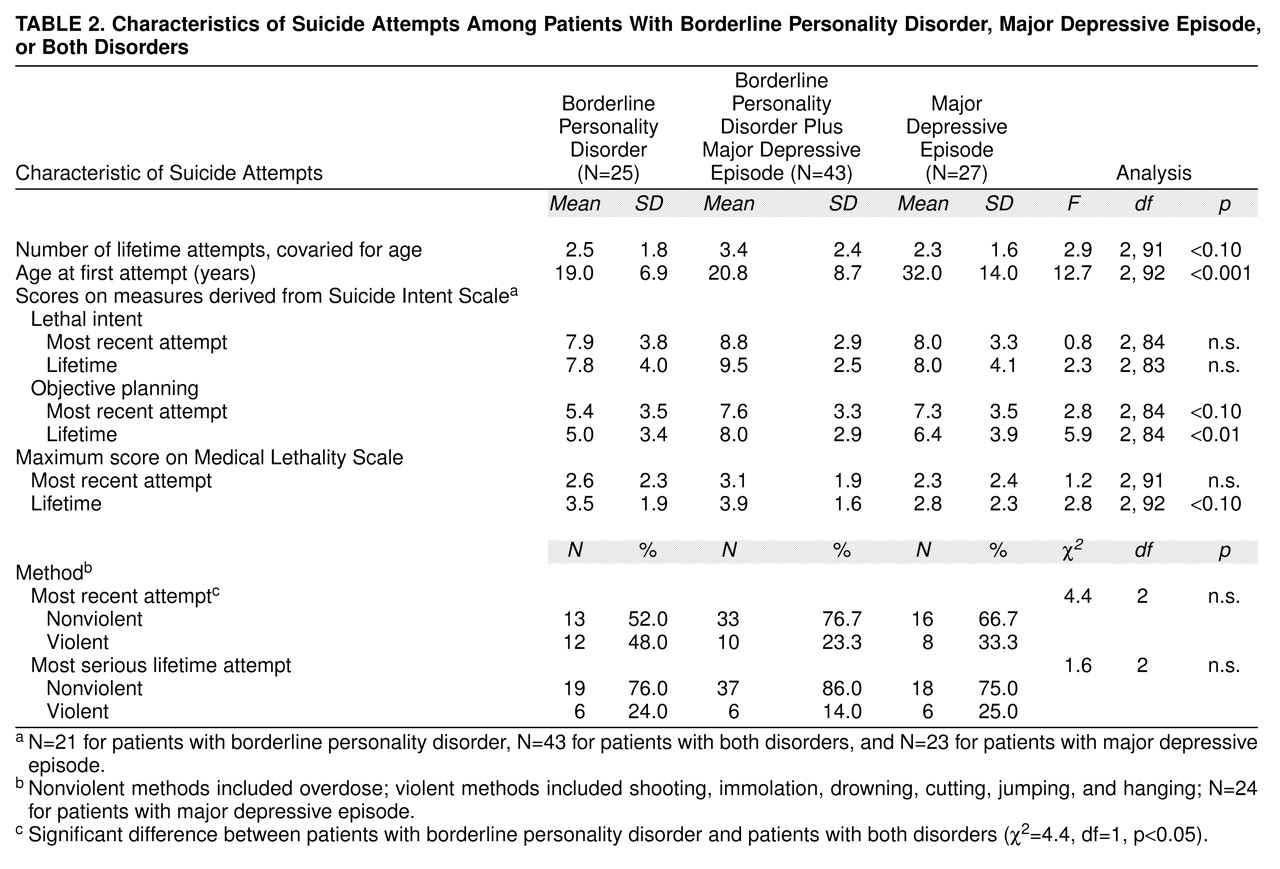
Group differences. Suicide attempts were more prevalent among the total sample of borderline patients compared to the depressed patients (
table 2). Among the 81 patients with borderline personality disorder, 68 patients had a lifetime history of suicide attempts and only 13 patients—seven patients with borderline personality disorder only and six patients with comorbid major depressive episode—had never attempted suicide. In the depressed group, 27 patients had a lifetime history of suicide attempts and 50 patients had never attempted suicide (χ
2=40.1, df=2, p<0.001). Patients with comorbid disorders had a mean of 3.0 lifetime attempts (SD=2.5), significantly more than patients with borderline personality disorder only (mean=1.9, SD=1.9), who, in turn, had more attempts than the depressed patients (mean=0.8, SD=1.5), with age as a covariate (F=17.1, df=2, 154, p<0.001). The differences were less robust when the analysis was restricted to patients who had attempted suicide (F=2.9, df=2, 91, p=0.06) (
table 2). Two depressed patients reported five and eight attempts, respectively. When these two outliers were omitted, the differences between groups who had attempted suicide was more robust (F=16.7, df=2, 89, p=0.02). Patients with borderline personality disorder or comorbid disorders attempted suicide for the first time earlier in life than the depressed patients; no significant difference in age at first suicide attempt was found between patients with borderline personality disorder and patients with comorbid disorders. There were no significant differences between groups on the lethal intent factor derived from the Suicide Intent Scale for the most recent or most serious lifetime attempt. Patients with comorbid disorders had the highest score on the objective planning factor derived from the Suicide Intent Scale (for the most serious lifetime attempt). Their score was significantly higher than that of patients with borderline personality disorder, although it was not significantly different from the score for the depressed patients. Differences between the three groups for medical damage assessed by using the Beck Lethality Scale (for the most serious lifetime attempt) fell short of statistical significance (F=2.83, df=2, 92, p=0.06). However, the suicide attempts of the pooled group of patients with borderline personality disorder had a greater lifetime level of lethality than those of the depressed patients (t=2.2, df=93, p=0.03). There was no significant difference between the three groups in the proportion of patients using violent or nonviolent methods. However, in the most recent attempt, more patients with borderline personality disorder used violent methods compared to patients with comorbid disorders (χ
2=4.4, df=1, p<0.05).
Relationship of clinical and attempt characteristics. Do the core clinical characteristics of depressed patients and patients with borderline personality disorder who attempt suicide predict the characteristics of their suicidal behaviors, such as number of attempts, level of subjective intent or objective planning, degree of medical damage, and choice of method? To explore this question, we used a multiple regression analysis that included dependent variables with little intercorrelation between measures. Depression was assessed by using the Hamilton depression scale and the Beck Hopelessness Scale, and impulsive aggression was assessed by using the Brown-Goodwin Lifetime History of Aggression. Diagnosis (borderline personality disorder only, borderline personality disorder plus major depressive episode, and major depressive episode only) and age were included as independent variables, and lifetime number of suicide attempts (log transformed) was the dependent variable. Stepwise selection was used to choose a best regression model that included the independent variables of the initial model. The initial model with all variables, including all main effects and the interaction of diagnosis with each of the other covariates, explained 29% of the variance (adjusted R2, F=5.5, df=11, 107, p<0.001). None of the interaction terms were significant at the p≤0.05 level. A positive relationship was found between lifetime number of attempts, history of aggression, and hopelessness. This model predicted 60% more suicide attempts for the patients with borderline personality disorder and for those with comorbid disorders compared to the depressed patients, with no difference between the two groups with borderline personality disorder. Age and Hamilton depression scale score did not contribute significantly to the model. The final predictor model included diagnosis, history of aggression, and hopelessness and explained 30% of the variance (adjusted R2) in lifetime number of suicide attempts (F=13.7, df=4, 114, p<0.001). Using this predictor model, an increase in 1 point on the Brown-Goodwin Lifetime History of Aggression led to a 3% increase in predicted lifetime number of suicide attempts (95% confidence interval [CI]=1%–4%). A 1-point increase on the Beck Hopelessness Scale led to a 2% increase in predicted lifetime number of suicide attempts (95% CI=0%–4%).
The data analyses were repeated by using data from the patients who had attempted suicide. We developed a model that included all of the candidate independent variables—diagnosis, history of aggression, hopelessness, and the interactions of each main effect with diagnosis. The dependent variables were characteristics of suicide attempts, including degree of lethal intent and objective planning, medical damage, and violence of the method, for both the most recent and the most serious lifetime suicide attempts. As lifetime number of suicide attempts (log transformed) was not significantly correlated with age in any group, both were included as independent variables in these analyses.
Lethal intent for the most serious lifetime attempt was predicted by hopelessness, as a single variable and best model, across all groups (adjusted R2=10.0, F=8.4, df=1, 67, p<0.01). Diagnosis, age, lifetime number of attempts, and history of aggression were not related to lethal intent. Findings were not significant for the most recent attempt.
In the regression analysis that examined clinical predictors of objective planning, a significant interaction was found between diagnosis and hopelessness, prompting separate regression analyses for each diagnostic group. Among patients with comorbid disorders, increases in the level of objective planning (for the most serious lifetime attempt) were predicted by increases in hopelessness, with increasing age as a secondary factor. A full model with all variables explained 36% of the variance (adjusted R2=35.8, F=5.33, df=4, 27, p=0.003), and hopelessness and age together explained 27% of the variance (adjusted R2=26.7, F=6.7, df=2, 29, p<0.01). There were no significant predictors of objective planning in the groups with borderline personality disorder or the depressed group. History of aggression and lifetime number of suicide attempts were not related to the degree of objective planning in any diagnostic group. Findings for the most recent attempt were very similar. In the group with comorbid disorders, hopelessness and age predicted objective planning (adjusted R2=26.1, F=6.7, df=2, 30, p<0. 0004).
The full model was not significant in predicting the degree of medical damage (for the most serious lifetime attempt). The degree of medical damage was predicted by the lifetime number of suicide attempts, as a best model, across all diagnostic groups (adjusted R2=9.0, F=7.9, df=1, 70, p<0.01). Age, aggression history, and hopelessness did not predict the degree of medical damage. No predictors were found for the most recent attempt.
There were no relationships between predictor variables and choice of violent or nonviolent methods for either the most recent or the most serious lifetime attempts.