It is widely accepted that an individual who sustains a mild traumatic brain injury can also suffer acute stress disorder and posttraumatic stress disorder (PTSD)
(1–
3). The proposal that the absence of recall for the traumatic event precludes the development of PTSD
(4) has been called into question by evidence relating to the implicit encoding of traumatic memories
(5), the reconstruction of memories on the basis of a secondary source
(6), and the intact islands of memory of the trauma during the period of posttraumatic amnesia
(7).
Acute stress disorder was introduced in DSM-IV to describe acute reactions that predict PTSD
(8). One standard by which any new diagnosis is measured is its long-term stability across longitudinal studies
(9). Previous reports indicate that 13% of the people who sustain mild traumatic brain injuries suffer acute stress disorder
(3) and that the majority of these individuals (82%) are diagnosed with PTSD at 6 months posttrauma
(10). This research provides initial evidence for the proposal that acute stress disorder is a precursor of PTSD. Longer-term prospective study is required to validate the predictive ability of the acute stress disorder diagnosis. Accordingly, we determined the relationship between the acute stress disorder diagnosis and PTSD status 2 years posttrauma.
METHOD
The study group was selected from adult victims of motor vehicle accidents who were consecutively admitted to a major trauma hospital. A total of 79 patients were assessed within 1 month of the trauma, and 63 were reassessed at 6 months posttrauma. The participation of 50 individuals at the 2-year follow-up represents a retention rate of 63% of the initial study group and 79% of the group assessed at 6 months. The groups assessed at 1 and 6 months are described in full elsewhere
(10). At the 2-year assessment, two patients refused to participate and 11 had changed residences. The final study group included 31 men and 19 women, who ranged in age from 17 to 58 years (mean=27.00, SD=10.62). The subjects were assessed an average of 721.68 (SD=49.41) days posttrauma, and the mean injury severity score was 10.08 (SD=6.38)
(10,
11), indicating moderately severe injuries. Of the 50 subjects, 22 had been drivers in their accidents, 10 had been passengers, 12 had been motorbike riders, five had been pedestrians, and one had been a cyclist. Those who participated in the 2-year posttrauma assessment did not differ from nonparticipants in terms of age, diagnosis, length of hospital stay, injury severity score, or interval between trauma and assessment for acute stress disorder. At the 2-year follow-up, three patients (6%) had received anxiolytic medication, and three (6%) had received cognitive behavior therapy; 14 (28%) had settled compensation claims, and 19 (38%) still had compensation claims pending.
All three assessments were carried out by clinical psychologists with more than 5 years of experience in assessing traumatized individuals (including A.G.H.). After complete description of the study to the subjects, written informed consent was obtained. The diagnosis of acute stress disorder was made by using the Acute Stress Disorder Interview
(12). Dissociative amnesia was excluded as a possible symptom of acute stress disorder because of the overlap between dissociative and organic amnesia following mild traumatic brain injury. The 6-month and 2-year assessments involved the administration of the PTSD module from the Composite International Diagnostic Interview
(13). In addition, the patients were asked whether they had received psychological treatment and the status of any legal proceedings arising from the motor vehicle accident.
The full criteria for acute stress disorder were met by 14% (N=11) of the initial study group. PTSD was diagnosed in 24% (N=15) at 6 months posttrauma and in 22% (N=11) at 2 years posttrauma. Chi-square analyses indicated that the patients with PTSD were not more likely to report pending compensation than those without PTSD (χ
2=1.57, N=50, df=1, with Yates’s correction, n.s.)
(14).
Of the 11 subjects with acute stress disorder, 10 completed all three assessments; 80% (N=8) met the criteria for PTSD at the 2-year follow-up, and 20% (N=2) did not. Of the 40 who were not diagnosed with acute stress disorder and completed the three assessments, 8% (N=3) met the criteria for PTSD and 93% (N=37) did not. To provide the most conservative estimate, we also considered diagnostic status at 2 years posttrauma as a function of the initial study group; by this calculation, 73% of the patients with a diagnosis of acute stress disorder (eight of 11) met the criteria for PTSD at the 2-year follow-up.
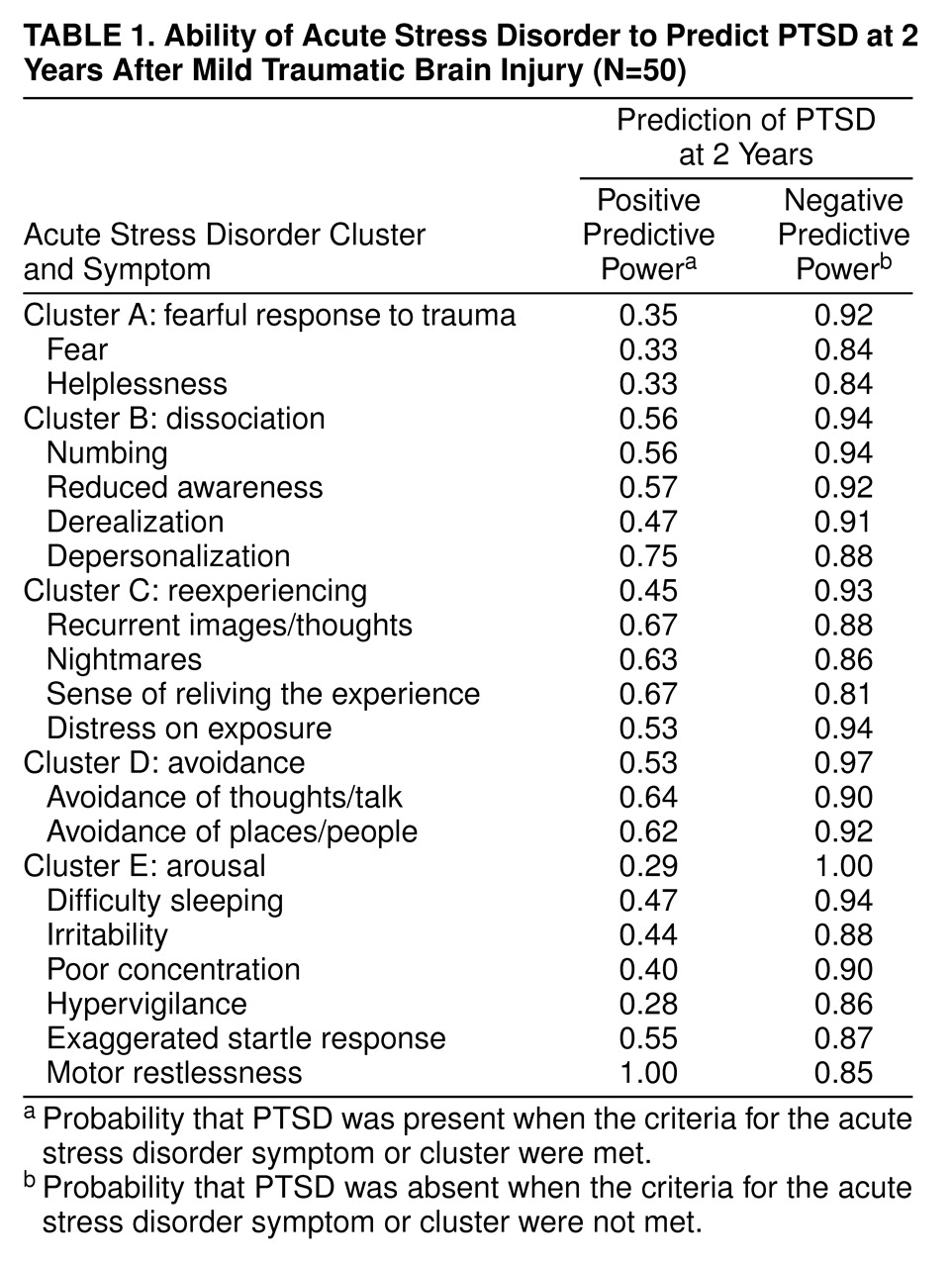
Table 1 presents the positive and negative predictive power of each acute stress disorder symptom and each symptom cluster on the basis of diagnostic status at 2 years posttrauma. Whereas all of the symptoms of acute stress disorder had reasonably strong negative predictive power, the symptoms with the strongest positive predictive power were numbing, reduced awareness, depersonalization, recurrent images/thoughts, nightmares, a sense of reliving the traumatic experience, avoidance, and motor restlessness.
Table 1 also presents the positive and negative predictive power for each acute stress disorder diagnostic cluster. All clusters had strong negative predictive power; positive predictive power varied. When the threshold for the dissociative cluster was set at two (rather than three) symptoms, the positive predictive power increased to 0.82, but the negative predictive power decreased to 0.77. When two symptoms were required for each of the reexperiencing and avoidance clusters, there was an increase in positive predictive power (0.73 and 0.92, respectively), and the negative predictive power stayed constant (0.92 and 0.97, respectively). When three arousal symptoms were required, the positive predictive power improved to 0.56 and the negative predictive power decreased marginally to 0.94.
DISCUSSION
At 2 years posttrauma, 22% of the participants met the full criteria for PTSD. This rate is consistent with previously reported incidence rates of PTSD following motor vehicle accidents
(15). The finding that 80% of the patients who satisfied the criteria for acute stress disorder had PTSD at 2 years posttrauma adds support to the utility of the acute stress disorder diagnosis as a predictor of chronic PTSD. It needs to be recognized that this figure may not take into account the individuals who did not participate in the follow-up assessments. The current findings also indicate that the predictive power of the acute stress disorder criteria may be enhanced by placing greater emphasis on acute reexperiencing, avoidance, and arousal symptoms. This suggestion is consistent with findings in prospective studies of study groups without traumatic brain injury that indicate that many trauma survivors who do not display acute dissociative symptoms subsequently develop PTSD
(16).
The strong predictive power of numbing and depersonalization supports the notion that dissociative mechanisms may prevent the processing and integration of trauma-related information and thereby contribute to ongoing PTSD
(17). The role of acute motor restlessness in predicting subsequent PTSD accords with evidence that persistent PTSD may be mediated by heightened arousal in the acute posttrauma phase
(18,
19).
When the patients who had received therapy were excluded, the findings were nearly identical to those from the initial analyses. Although comparable proportions of PTSD and non-PTSD patients reported ongoing litigation, we recognize that compensation issues may influence the reporting of PTSD symptoms. Also, these results may not be generalized to other trauma populations. Moreover, future research needs to determine the relationship between acute stress disorder and development of other psychiatric disorders in the acute posttrauma phase. In summary, although the current findings point to the utility of the acute stress disorder criteria, there appears to be a need for refinement of these criteria to enhance predictive power.