Childhood abuse is associated with subsequent physical and emotional disorders
(1). A history of sexual abuse may place adolescents in psychiatric treatment at risk for HIV infection
(2). Adolescents in psychiatric treatment who have a history of sexual abuse report greater rates of substance abuse than their peers
(3). However, differences in sexual behavior have not been examined, to our knowledge. In public schools, survivors of sexual abuse have been found to be significantly more likely to be sexually active, to use condoms inconsistently, and to use alcohol and drugs than peers without a history of abuse
(4,
5). Many sexually abused adolescents also suffer from feelings of low self-esteem, fear of rejection, mistrust, and powerlessness
(6).
No differences in psychopathology have been found between adolescents with and without sexual abuse except for higher rates of posttraumatic stress disorder (PTSD) in those with abuse
(3,
7). It is, therefore, unlikely that tendencies toward HIV-related risk are directly related to differences in psychopathology. Our earlier study among adolescents in psychiatric treatment
(8) found no association between a history of sexual abuse and HIV-risk-related behaviors, although sexual abuse was associated with risky attitudes among girls
(8). The present study expands the literature by focusing on the behavior of a larger group of sexually active adolescents in intensive psychiatric treatment to examine the relationship between a history of sexual abuse and HIV-risk-related behavior.
Method
The study participants (N=208) attended psychiatric day schools and residential programs; 84.2% (208 of 247) of the youths eligible for the study (between 13 and 18 years of age, not psychotic, and able to participate in school activities) were enrolled. The diagnostic range of patients was similar to that found in other therapeutic settings (33.2% [N=69] had impulse-control disorders, 29.8% [N=62] had depressive disorders, and 9.1% [N=19] had PTSD as their primary diagnosis). Those without a history of sexual intercourse (N=92) were dropped from subsequent analyses. Eighteen adolescents had clinical histories of abusive sexual experiences only during childhood, and 10 had been abused sexually only since age 13. Thirty-three subjects had histories of childhood sexual abuse both before and during adolescence. Scale scores (examined by means of analysis of variance) and behaviors (examined by means of chi-square analysis) of the three groups of abused adolescents were similar, so they were combined for subsequent analyses (N=61). After describing the study to subjects, written informed consent was obtained from a parent or guardian.
All participants completed measures of HIV-related knowledge, tolerance of individuals with HIV, perceived susceptibility to HIV, intention to prevent the transmission of HIV, condom self-efficacy, and HIV self-efficacy, which have shown excellent reliability and internal consistency
(9,
10,
11). The Condom Self-Efficacy Scale
(10) reflects the emotional context of condom use (e.g., “You use a condom when you’re upset”), while the HIV Self-Efficacy Scale
(11) assesses practical skills (e.g., the ability to acquire and carry condoms). Assessed behaviors included history of sexually transmitted diseases, substance use, and frequency of purchasing and using condoms. Two subscales from the Weinberger Adjustment Inventory
(12) measured impulse control and self-restraint. A measure of general attitudes not related to HIV risk
(9) was completed.
Results
There were no differences in age, ethnicity, or history of substance abuse between the adolescents with (N=61) and without (N=55) a history of sexual abuse (age: mean=15.13 years, SD=1.53; mean=15.05, SD=1.35, respectively) (ethnicity: 40 white, 74.1%; 39 white, 75.0%) (history of substance abuse: N=30, 49.2%; N=27, 49.1%). However, more of those with a history of sexual abuse were female (N=32 of 61, 51.5%) than were those without a history of sexual abuse (N=11 of 55, 20%) (χ2=12.98, df=1, p<0.001). Those with a history of sexual abuse were diagnosed with PTSD more often (N=16, 26.2%) than were those without such a history (N=2, 3.6%) (χ2=11.25, df=1, p<0.001), whereas adolescents without a history of sexual abuse were more often diagnosed with attention deficit hyperactivity disorder (N=16, 26.2%) than were those with such a history (N=4, 7.3%) (χ2=10.23, df=1, p<0.001). Otherwise, there were no diagnostic differences between the groups. (Note that some data were missing.)
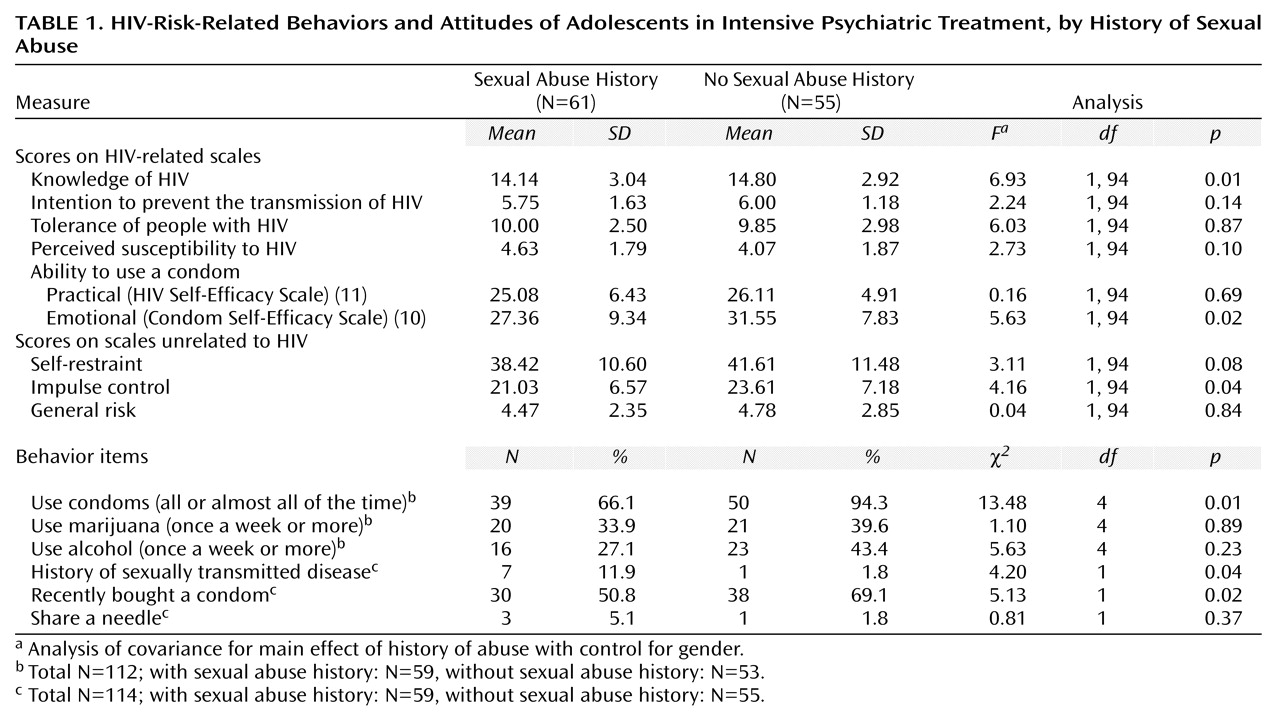
A multivariate analysis of covariance controlling for gender found a significant difference in overall HIV-risk-related behaviors and attitudes between adolescents with and without a history of sexual abuse (F=2.79, df=9, 86, p<0.01). Univariate tests found that adolescents with a history of abuse scored significantly lower on knowledge of HIV, condom self-efficacy, and impulse-control scales compared to their peers (
Table 1). Abuse was significantly associated with inconsistent condom use, failure to purchase condoms, and a history of sexually transmitted diseases.
To identify these associations with recent sexual behavior, a multiple logistic regression for inconsistent condom use examined simultaneously all significant variables (history of sexual abuse, condom self-efficacy, impulse control, and gender) (model χ2=14.87, df=4, N=108, p<0.01). Only a history of sexual abuse was found to be significantly associated with recent risky sexual behavior (adjusted odds ratio=3.06, 95% confidence interval=1.21–7.70) (Wald χ2=5.62, df=1, p=0.01).
Discussion
This study found that adolescents with a history of sexual abuse were three times more likely than their peers to report inconsistent condom use, a finding not attributable to gender or diagnostic differences. Having a history of abuse was also significantly associated with having more sexually transmitted diseases, less impulse control, and less knowledge of HIV than adolescents without a history of abuse. Participants with a history of sexual abuse scored significantly lower on the Condom Self-Efficacy Scale, which measures the perceived ability to use condoms in difficult situations. This new finding suggests that even among adolescents in psychiatric treatment with high HIV-related risk, those who have experienced sexual abuse have greater difficulties enacting “safe” sexual behaviors than those who have not been sexually abused.
This study has limitations. It is possible that a history of sexual abuse may be associated with the severity of a psychopathology that was not measured. However, there were few diagnostic differences, as has been consistent with the results of other studies. The finding of less nonsexual impulse control among those with a history of abuse suggests difficulties with behavior control that perhaps are not reflected in diagnostic or general distress measures. In addition, the cross-sectional design precluded analysis of causal links between sexual abuse and HIV-related attitudes or sexual initiation.
Clinicians should consider a history of sexual abuse as a marker for current HIV-risk-related behaviors among adolescents with psychiatric impairment. Adolescents with a history of sexual abuse may have particular difficulty being assertive in sexual situations. Sexual abuse may lead to low self-esteem, powerlessness, and difficulty maintaining appropriate sexual boundaries. Because sexuality may revive traumatic memories and affect, simple behavioral rehearsal does not appear to be sufficient to induce assertiveness. Therapy is an opportunity to assist adolescents in reducing their anxieties (e.g., “He might leave me if I make him use a condom”) and restoring the self-efficacy (e.g., “I can control what happens when I have sex”) needed for a safer future.