Subjects
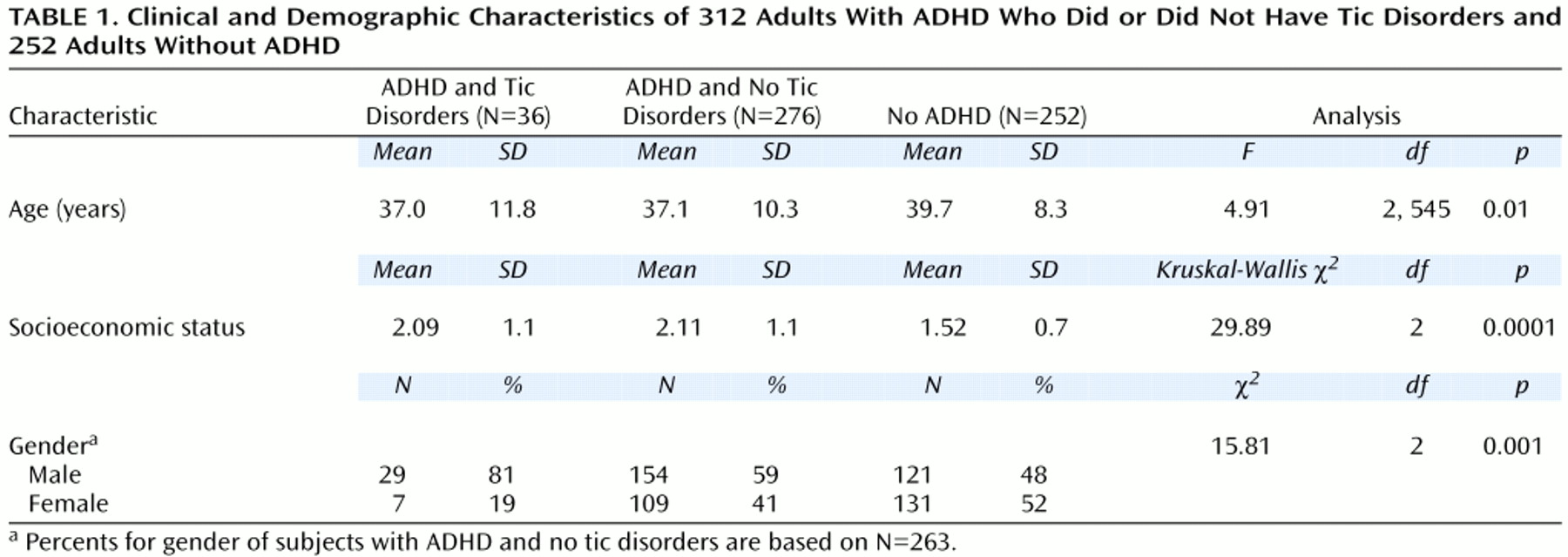
Subjects were 312 consecutively referred adults between the ages of 19 and 59 who met full DSM-III-R diagnostic criteria for ADHD (lifetime) after clinical assessment that was confirmed with structured diagnostic interview. Each patient had a diagnosis of childhood-onset ADHD that persisted as a full syndrome (eight or more of 14 ADHD symptoms) (87%, N=272) or partial syndrome (five or more of 14 ADHD symptoms) (13%, N=40) in adulthood. For all subjects, ADHD symptoms were clearly associated with both lifetime and current impairment. The comparison subjects were 252 healthy adults participating in ongoing studies at our center who did not have ADHD.
We excluded subjects only if they had major sensorimotor handicaps (paralysis, deafness, blindness), active psychosis, or a full-scale IQ of less than 80. We received approval from the institutional review board to review, analyze, and report on data on referred adults with ADHD treated at our center. After complete description of the study to the comparison subjects, written informed consent was obtained from the comparison subjects.
Diagnostic and Assessment Procedures
The procedures used to evaluate the referred adults with ADHD were identical to those used in our clinical research program and those used extensively in studies of boys and girls as well as adults with ADHD
(16). Briefly, we administered the Structured Clinical Interview for DSM-III-R
(17) supplemented with modules from the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Epidemiologic Version (K-SADS-E)
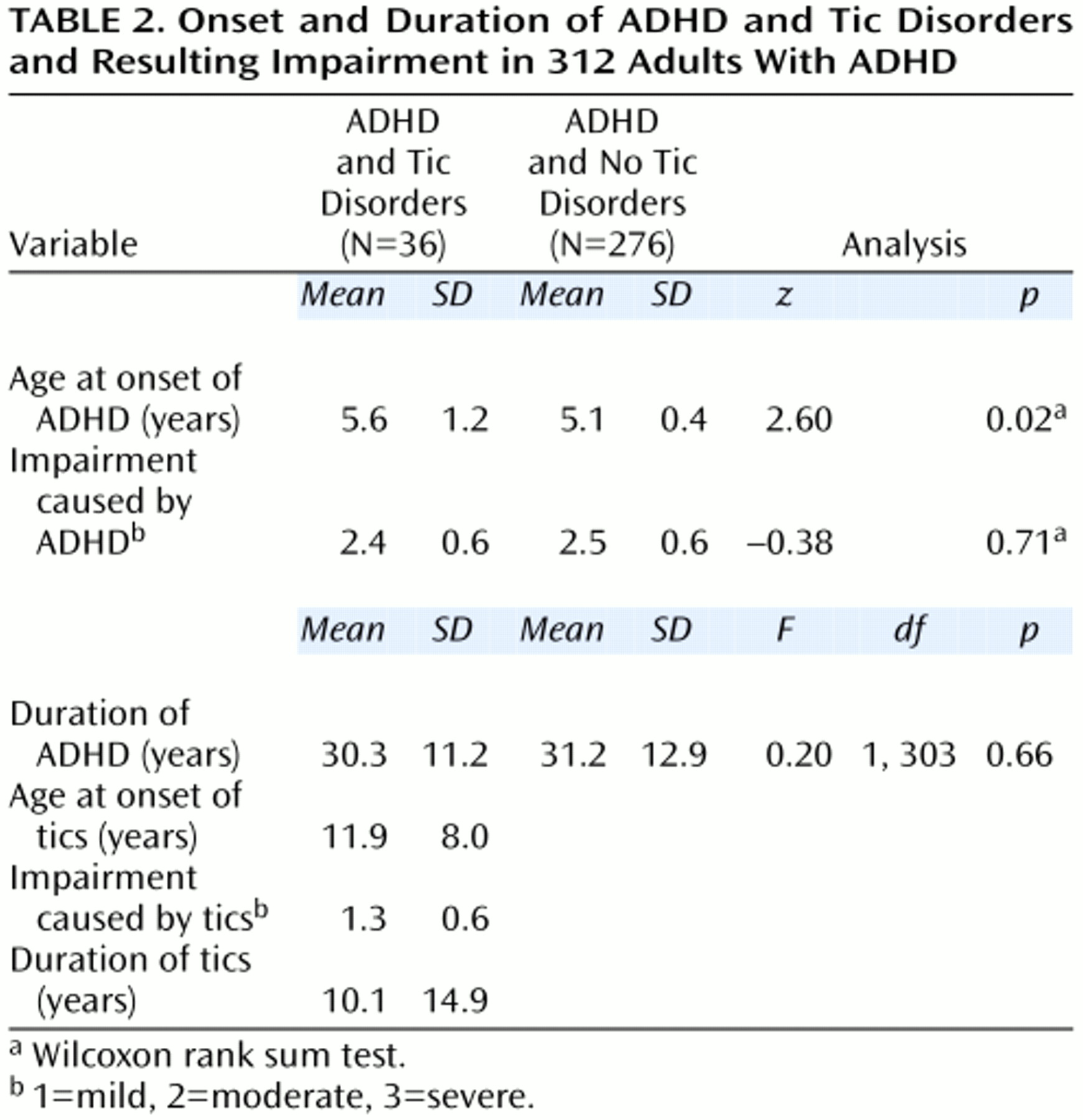
(18) covering childhood diagnoses. Rates of disorders are lifetime prevalences. The interviewers of referred adults were blind to the subjects’ clinical diagnoses but not to their referral status. For every diagnosis, information was gathered regarding the associated level of impairment (1=mild, 2=moderate, 3=severe), age at onset of symptoms, age at offset of symptoms, number of episodes, and treatment history.
We computed kappa coefficients of agreement by having three experienced, board-certified child and adult psychiatrists diagnose subjects on the basis of audiotaped interviews made by the assessment staff. The median kappa for 173 interviews was 0.86. For the diagnoses of tics and Tourette’s syndrome, perfect reliability was established both between trained raters and between raters and senior clinicians (kappa=1.0); the kappa for ADHD was 0.98. A committee of board-certified child and adult psychiatrists chaired by the program director (J.B.) resolved all diagnostic uncertainties.
To be given a diagnosis of adult ADHD, the subject must have 1) met DSM-III-R criteria for a diagnosis of ADHD by the age of 7, 2) had at least five DSM-III-R symptoms of ADHD at the time of assessment, and 3) described a chronic course of ADHD symptoms from childhood to adulthood. To elicit ADHD symptoms, we used the ADHD module from the K-SADS-E, wording questions in the past tense. If the subject endorsed a symptom to a clinically meaningful degree, we asked whether similar problems were currently present. By using this method we assured that the syndrome observed in adulthood had some continuity with the syndrome reported in childhood.
To be given a diagnosis of Tourette’s syndrome, the subject must have fulfilled all five DSM-III-R criteria: A) both multiple motor tics and one or more vocal tics, B) the tics occur many times a day nearly every day or intermittently throughout a period of more than 1 year, C) the anatomic location, number, frequency, complexity, and severity of the tics change over time, D) onset before age 21, and E) occurrence not due to psychoactive substance intoxication or central nervous system illness (DSM-III-R, p. 80). Non-Tourette’s-syndrome tic disorders were defined as either motor or vocal tics but not both; these tic disorders had to fulfill DSM-II-R criteria B, D, and E. Tic disorders were defined as chronic if the duration was at least 1 year; otherwise, tic disorders were classified as transient.
We used the following interview questions from the tic module of the K-SADS-E: 1) Did you ever have any frequent, jerky, repetitive motor movements such as lip smacking or frequent eye blinking? Other repetitive movements of the face or body (not rhythmic or fidgeting)? What about touching or squatting? 2) Did you ever have vocal tics (grunts or yelps) or utter obscenities? 3) Did the tics (or grunts) occur many times a day (usually in bouts), nearly every day or intermittently throughout a period of more than 1 year? 4) Did the severity and location of the tics change over time? 5) Were you ill at the time the tics occurred? and 6) Were you abusing drugs or alcohol at the time the tics occurred?
As suggested by others
(19,
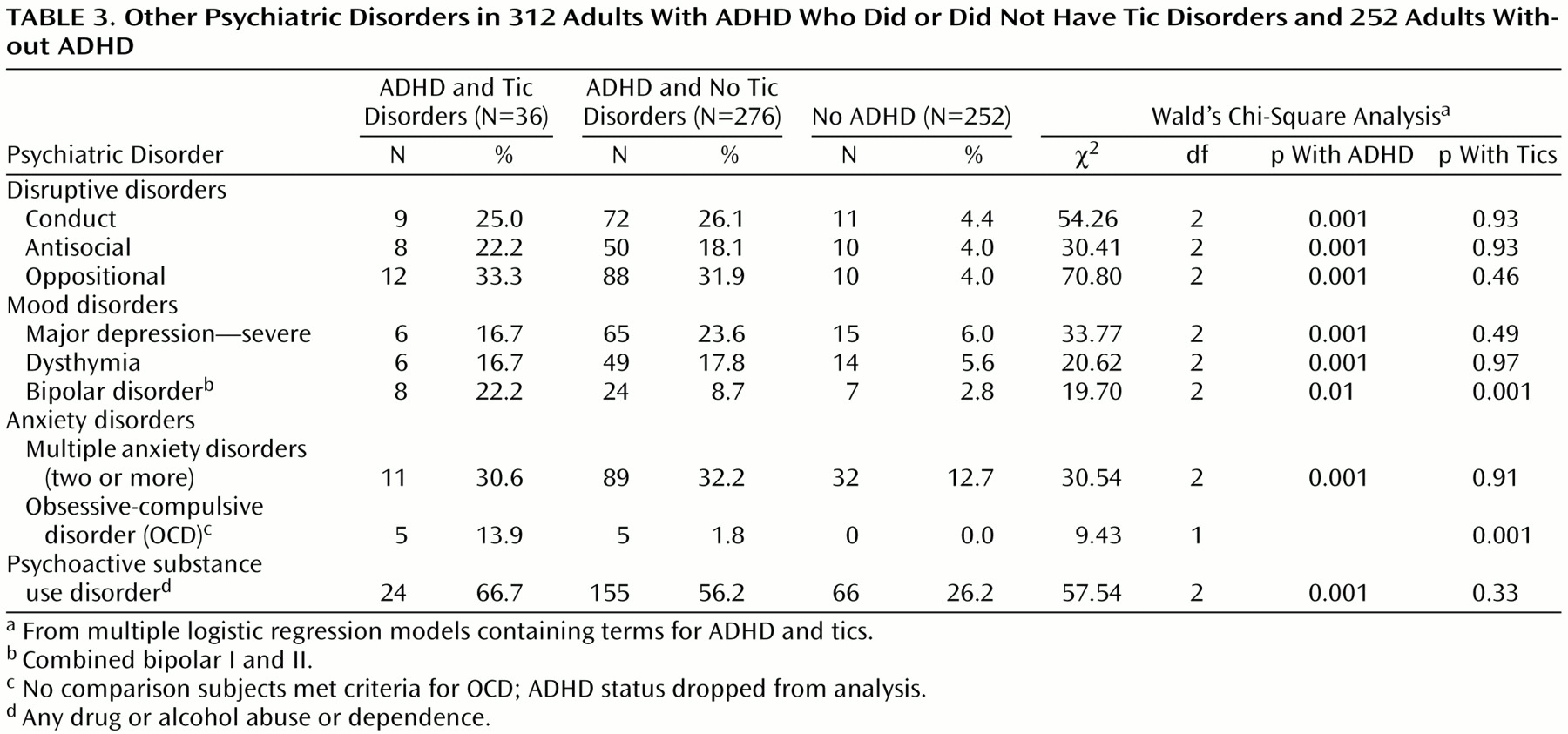
20), we diagnosed major depression only if the depressive episode was associated with marked impairment. Since the anxiety disorders comprise many syndromes with a wide range of severity, we used two or more anxiety disorders to capture the presence of a clinically meaningful anxiety syndrome. We refer to this as “multiple anxiety disorders,” as we have elsewhere
(21).
To examine cognitive function, we used a test battery analogous to that used in previous reports of children and adolescents with ADHD
(22,
23). We estimated full-scale IQ from the vocabulary and block design subtests of the WAIS-R
(24–
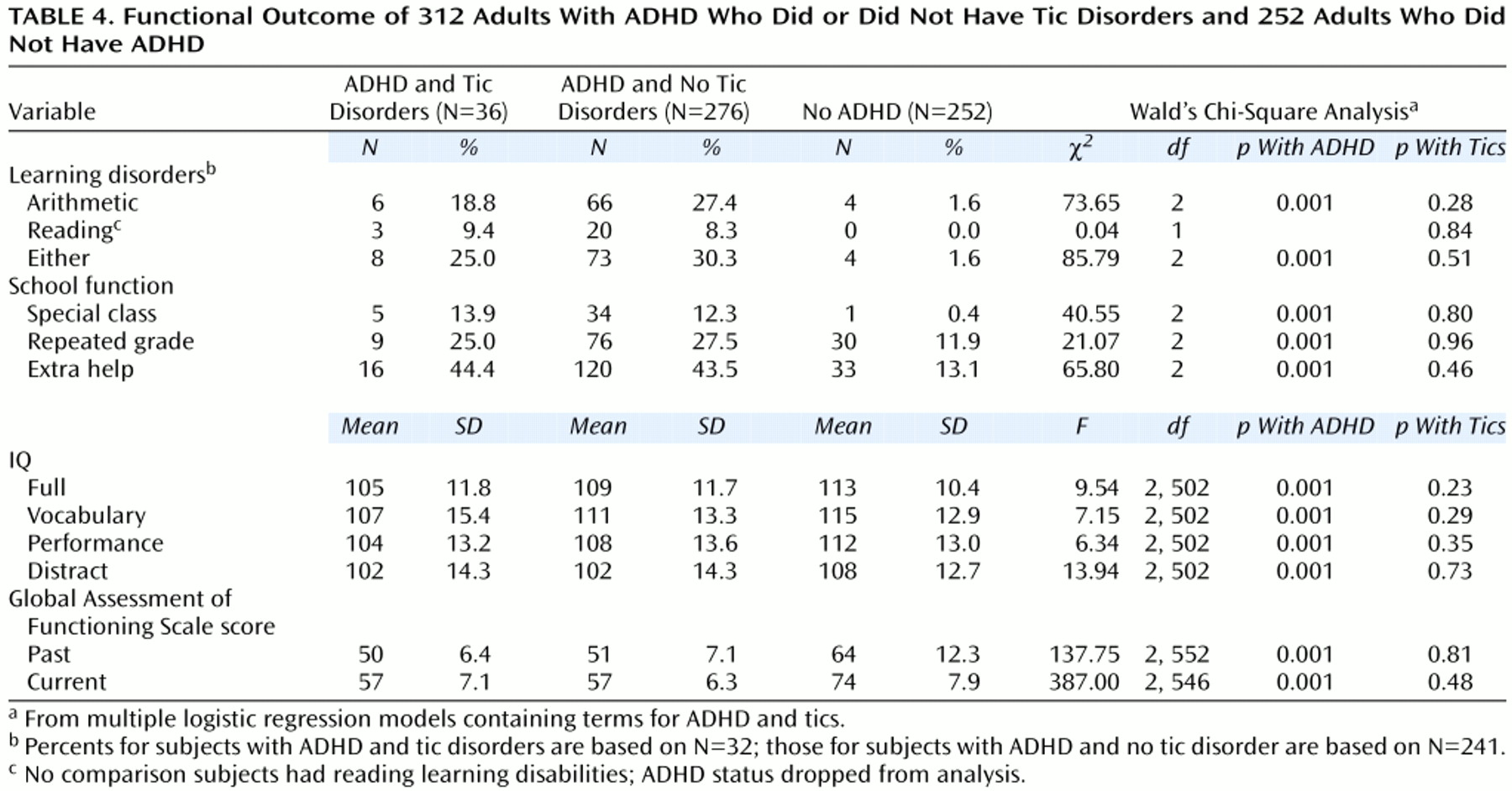
26). We used the digit symbol, digit span, and arithmetic subtests of the WAIS-R to estimate the freedom from distractibility IQ. Academic achievement was assessed with the arithmetic and reading subtests of the Wide Range Achievement Test, Revised
(27). We used the procedure recommended by Reynolds
(28) and others to define learning disabilities. To evaluate school functioning, we assessed three straightforward indexes of school failure: placement in special classes, in-school tutoring, and repeated grades. Psychosocial functioning was assessed with the Global Assessment of Functioning Scale (1=worst, 90=best) (DSM-III-R, p. 12). Socioeconomic status was measured with the four-factor Hollingshead scale (1=highest, 4=lowest)
(29).