In response to the concern that symptoms of posttraumatic stress disorder (PTSD) in the first month after trauma might reflect normal reactions to extreme stress, the authors of DSM-IV also examined acute stress disorder with the aim of identifying a pathological acute trauma response. Both acute stress disorder and PTSD share similar stressor and impairment criteria and similar constituent symptom clusters, but the specific number and intensity of the symptoms required in each cluster vary, and there are additional dissociative symptoms specified in acute stress disorder. Initial prospective studies have found that acute stress disorder predicts the later onset of PTSD extremely well
(1–
4). However, some commentators have questioned whether acute stress disorder is sufficiently different from PTSD (without the 1-month duration criterion) to warrant a separate diagnosis
(5). Demonstrating that the two disorders are distinct is important in validating the current conceptualization of acute stress disorder.
The most direct method of answering this question is to examine the overlap between those who in the month after a traumatic event are eligible for a diagnosis of either or both acute stress disorder and PTSD (without the duration criterion). Ideally, both diagnoses should draw as far as possible on the same set of items in order to minimize extraneous variance. Although interviews are normally the gold standard for diagnosis, the possibility of preconceptions about the relation between acute stress disorder and PTSD affecting clinical judgment makes a good argument for questionnaire methodology. To our knowledge, the only prospective study to have measured acute stress disorder and PTSD simultaneously according to strict DSM-IV criteria, with sufficient numbers of patients to make an overlap analysis realistic, is our previous study of victims of violent crime (4). This current study concerns new analyses from that data set on the overlap between acute stress disorder and PTSD within 1 month of a trauma and on their relative power to predict PTSD 6 months later.
Method
The participants were crime victims who were over 18 years old and were assaulted by a nonhousehold member. Over 90% of the crimes involved physical assault. After screening out ineligible participants, we conducted 157 interviews within 1 month of the crime. The 118 men and 39 women who participated had an average age of 35 years (SD=13, range=18–76). A total of 87.9% of these individuals (N=138) were successfully followed up at 6 months. Full details of recruitment, participants, and crimes have been presented earlier
(4). Written informed consent was obtained after complete description of the study to the participants.
Full details of all measures were provided in our previous report
(4). All participants received a set of dichotomous ratings indicating whether they had met criteria for an overall diagnosis of DSM-IV PTSD and acute stress disorder at baseline and DSM-III-R PTSD at follow-up.
All stressors qualified for criterion A1 of DSM-IV PTSD. At the outset of the study, we knew of no published interviews or questionnaires assessing PTSD criteria A2, F, or acute stress disorder. The second part of the PTSD stressor criterion (A2) was therefore assessed with three items in which fear, helplessness, and horror were rated on 3-point scales. Criteria B, C, and D were measured with the self-report version of the Posttraumatic Stress Disorder Symptom Scale
(6). Seventeen items corresponding to the reexperiencing, avoidance, and arousal symptoms of PTSD were rated on 4-point scales (0=not at all/less than 2 days, 1=once per week or less/a little bit/once in a while, 2=2–4 times per week/somewhat/half the time, 3=5 or more times per week/very much/almost always). To conform to DSM-IV criteria, items from the Posttraumatic Stress Disorder Symptom Scale were only counted toward a PTSD diagnosis if they were scored 2 or more. Criterion F (impairment) was assessed from separate items measuring clinically significant distress, role impairment, and confiding.
For acute stress disorder, stressor (A), reexperiencing (C), arousal (E), and impairment (F) criteria were measured by using the same sets of items that had been used for PTSD diagnoses but with different thresholds where appropriate. Criterion B was assessed by using the emotional numbing and amnesia items from the Posttraumatic Stress Disorder Symptom Scale supplemented by three new items inquiring about reduction in awareness, derealization, and depersonalization. Criterion D was assessed by using the two avoidance items from the Posttraumatic Stress Disorder Symptom Scale.
DSM-III-R PTSD was assessed at follow-up by using the original Posttraumatic Stress Disorder Symptom Scale. As previously explained
(4), the less restrictive DSM-III-R criteria were preferred in order to avoid lack of variation in Criterion A2 at the two measurement points, leading to artificially inflated levels of prediction.
Results
At baseline, 30 participants (19.1%) were found to meet the criteria for acute stress disorder and 33 (21.0%) for DSM-IV PTSD. A total of 28 met the criteria for both diagnoses, two for acute stress disorder without PTSD, five for PTSD without acute stress disorder; 122 did not meet the criteria for either diagnosis. Overall percentage agreement between the two diagnoses was 95.5%. Overall, 28 of 138 participants (20.3%) met the criteria for a DSM-III-R diagnosis of PTSD at 6 months. The patients with this follow-up diagnosis consisted of the following: 15 of the 26 (57.7%) with both diagnoses at baseline (of a total of 138 followed up), one of the two (50%) with acute stress disorder without PTSD, two of the five (40%) with PTSD without acute stress disorder, and 10 of the 105 (9.5%) who did not meet the criteria for either diagnosis.
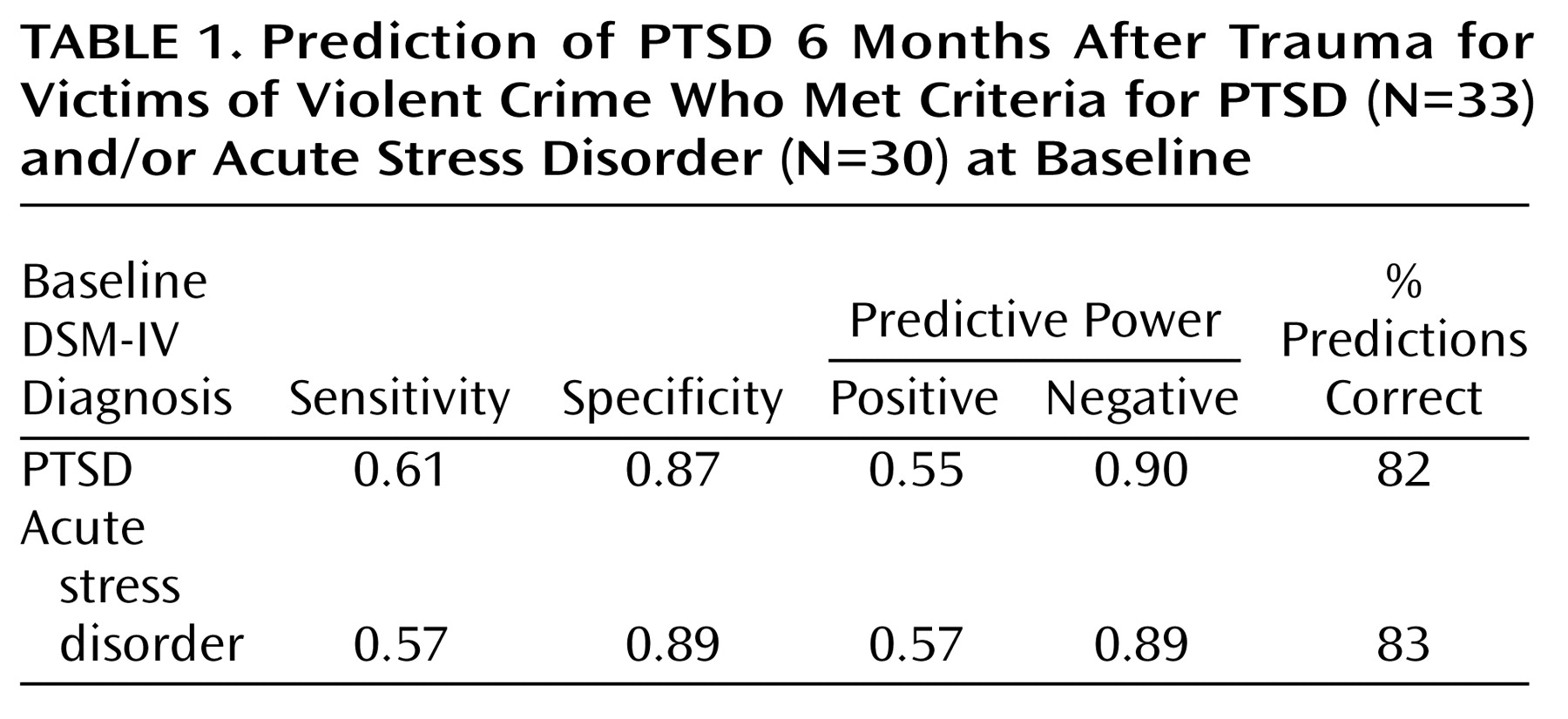
Table 1 shows the sensitivity of each diagnosis, i.e., the probability that someone with PTSD at 6 months would have earlier met the criteria for PTSD or acute stress disorder, and its specificity, i.e., the probability that someone without later PTSD would not have met the criteria for PTSD or acute stress disorder at baseline.
Table 1 also shows the positive predictive power of each diagnosis, i.e., the probability that someone with that diagnosis would later develop PTSD, and its negative predictive power, i.e., the probability that someone without that diagnosis would not subsequently develop PTSD. The overall percentage of patients correctly classified is also shown. From
Table 1, it is evident that the two baseline diagnoses were equivalent in predicting later PTSD.
Discussion
Our results suggest that acute stress disorder as currently formulated may not be sufficiently distinct from PTSD without its duration criterion, although caution is necessary until the findings are replicated in groups of other trauma survivors and in groups with different rates of disorders. One implication is that the undoubted ability of acute stress disorder to predict later PTSD may be unrelated to the greater number of dissociative symptoms required by a diagnosis of acute stress disorder. Our previous analyses
(4) showed that there was little difference between the symptom clusters in their ability to predict later PTSD, with reexperiencing and arousal symptoms somewhat more effective than equivalent numbers of dissociative symptoms. Also, it should be noted that our data primarily spoke to the issue of whether acute stress disorder can be successfully constructed around a variety of dissociative symptoms occurring either
during or
after trauma, a distinction that is not always noted. Our findings may indicate that posttraumatic dissociative reactions, such as depersonalization and derealization, are a common form of response and do not in any way contradict the growing evidence for the importance of peritraumatic dissociation as a psychological process that may impede the processing of information during the trauma itself.