As many as 50% of boys with conduct disorder continue to show antisocial behavior as young adults
(1), and the risk of antisocial personality development is even higher if antisocial behavior starts before age 10 years
(2). Attention deficit hyperactivity disorder (ADHD) has also long been associated with a higher risk of antisocial outcome
(3). However, a growing amount of data suggest that although there is indeed a close relationship between conduct disorder and antisocial personality disorder, no connection exists between ADHD and antisocial personality disorder
(4). The inconsistency in previous study findings could result from not considering the presence of comorbid conduct disorder in children with ADHD.
Progress has been made in uncovering biological risk factors in children that predispose them to developing antisocial personality disorder as grown-ups. In the field of psychophysiology, research has provided substantial data suggesting that lower levels of autonomic arousal (e.g., low resting heart rate), as well as autonomic hyporesponsiveness, indicate a greater likelihood of future antisocial behavior
(5,
6). In antisocial adolescents and adults, low responses to neutral and aversive stimuli have been found
(7,
8). In a previous study we found that boys with conduct disorder only and boys with comorbid ADHD and conduct disorder show low levels of electrodermal responses to orienting stimuli (i.e., nonprominent acoustic tones) and low levels of response to aversive tones but that boys with ADHD only did not differ from healthy comparison subjects on these measures
(9,
10). Fowles et al.
(5) suggested that there may be two attentional deficits in antisocial individuals of any age, one deficit with respect to attending to neutral stimuli and another deficit with respect to the anticipation of aversive events. In the search for factors underlying electrodermal hyporesponsiveness in antisocial individuals, temperamental dimensions, such as fearlessness, low levels of inhibitory control, or executive function deficits, have been discussed
(5,
11), and these dimensions may in turn give a predisposition toward antisocial behavior.
Case reports of patients with orbitofrontal damage who consistently showed an absence of punishment-related learning led Damasio et al.
(12) to establish the so-called somatic marker hypothesis. According to this hypothesis, somatic marker signals help in the anticipation of option-outcome scenarios with respect to punishment and reward
(13). Electrodermal hyporesponsiveness may be a relevant somatic marker, because individuals with “acquired sociopathy” after orbitofrontal cortex lesions were found to show low levels of autonomic responses to both positively and negatively valenced visual stimuli. Antisocial behavior in children has also been associated with amygdalar dysfunction, on the basis of findings of selective impairments in the processing of sad and fearful facial expressions
(14).
The objective of the current study was to examine psychophysiological responses as well as self-report measures of response to emotional stimuli (pictures of pleasant, neutral, and unpleasant phenomena) in 8–13-year-old boys with an exclusive diagnosis of conduct disorder or with the comorbid condition of ADHD plus conduct disorder, compared with children with ADHD only and healthy comparison subjects. ADHD children were chosen as a clinical comparison group for two reasons: 1) to control for probable psychophysiological effects related to the failure to adequately allocate attention to experimental stimuli and 2) because the choice of a comparison group with another extraversive disorder would possibly lead to findings that are specific for antisocial behavior. We had the specific hypothesis that children with conduct disorder and children with ADHD plus conduct disorder who viewed emotional pictures would report lower levels of emotional arousal on self-rating scales and would show lower levels of autonomic responses, compared with subjects with ADHD only and healthy comparison subjects.
Results
Diagnostic Data
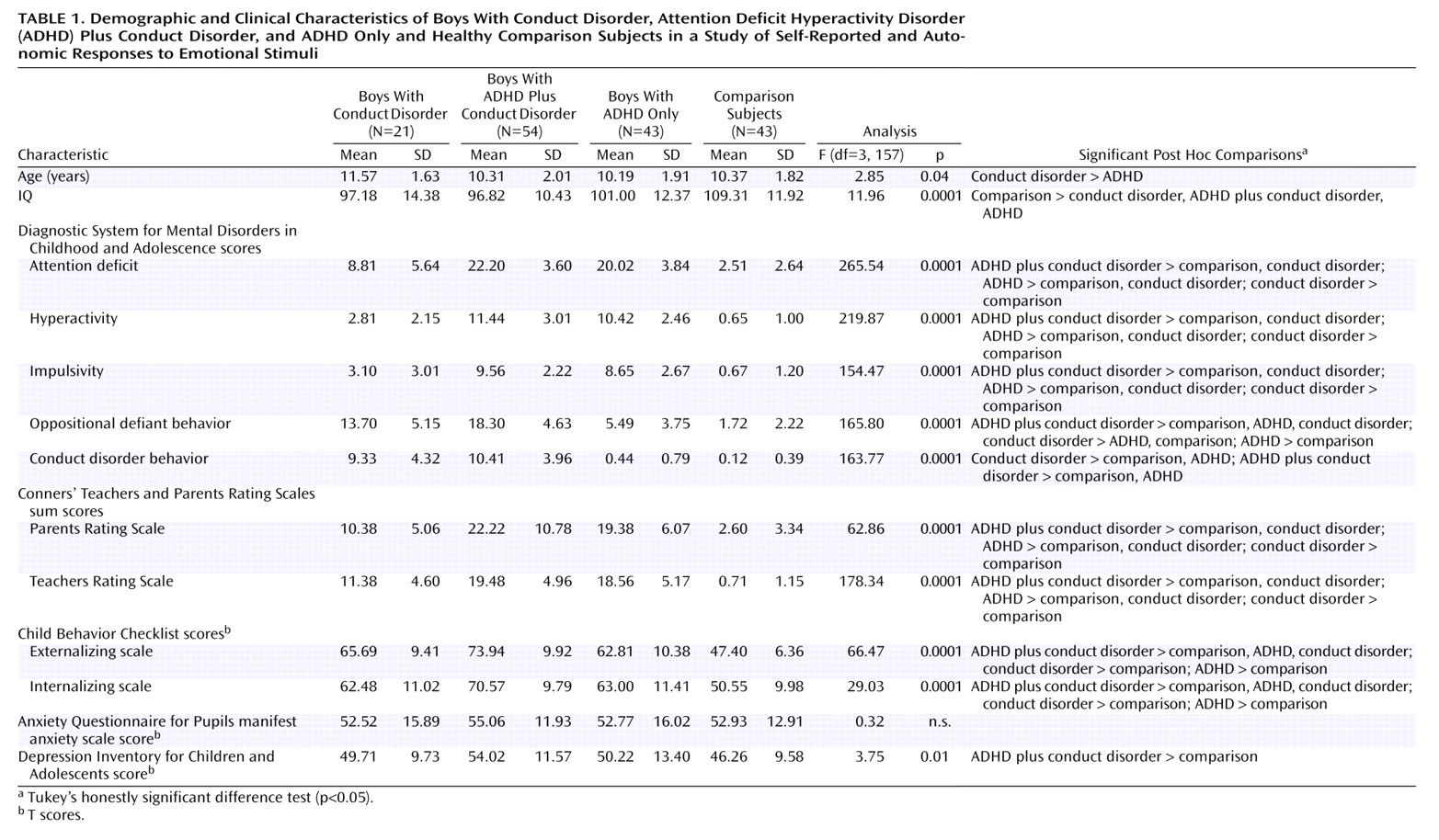
The subjects’ demographic and diagnostic data are summarized in
Table 1. There were group effects for age and intelligence. The ADHD boys were significantly younger than the conduct disorder boys, and the healthy comparison subjects were more intelligent than the other three groups, which were highly comparable with each other.
Data from all subscales of the diagnostic instrument (Diagnostic System for Mental Disorders in Childhood and Adolescence) confirmed significant overall group effects (p<0.0001). Post hoc Tukey’s tests revealed that, consistent with the design, the boys with conduct disorder only differed in ADHD symptoms from the boys with comorbid ADHD and conduct disorder. With regard to the conduct disorder symptoms, the boys with the comorbid condition showed more severe symptoms than those with conduct disorder only, and this difference reached the level of significance with regard to oppositional defiant behavior. By design the ADHD plus conduct disorder group did not differ from the ADHD group in the three ADHD criteria of attention deficit, hyperactivity, and impulsivity, but they differed in the severity of the two symptom criteria of conduct disorder (oppositional defiant behavior and conduct disorder behavior). Further diagnostic data based on the Conners’ Teachers and Parents Rating Scales supported the Diagnostic System for Mental Disorders in Childhood and Adolescence data, as they consistently showed that children with ADHD did not differ from those with ADHD plus conduct disorder in the severity of ADHD symptoms. Data from the Child Behavior Checklist showed a highly significant overall group effect on the externalizing and internalizing subscales, with all clinical groups differing from the healthy comparison subjects on both dimensions of psychopathology. Again, the ADHD plus conduct disorder group exhibited the most severe symptoms, with higher scores on the externalizing and internalizing subscales than the groups with conduct disorder only and ADHD only.
Self-report data showed no overall group differences on the anxiety scale. However, an overall group effect was found for the severity of depression (F=3.75, df=3, 157, p=0.01), although the mean values of all groups were still a long way from the pathological range (T score >60). Post hoc pairwise comparisons indicated that the boys with ADHD plus conduct disorder scored significantly higher than the healthy comparison subjects but that there was no difference between the clinical groups.
Emotional Ratings
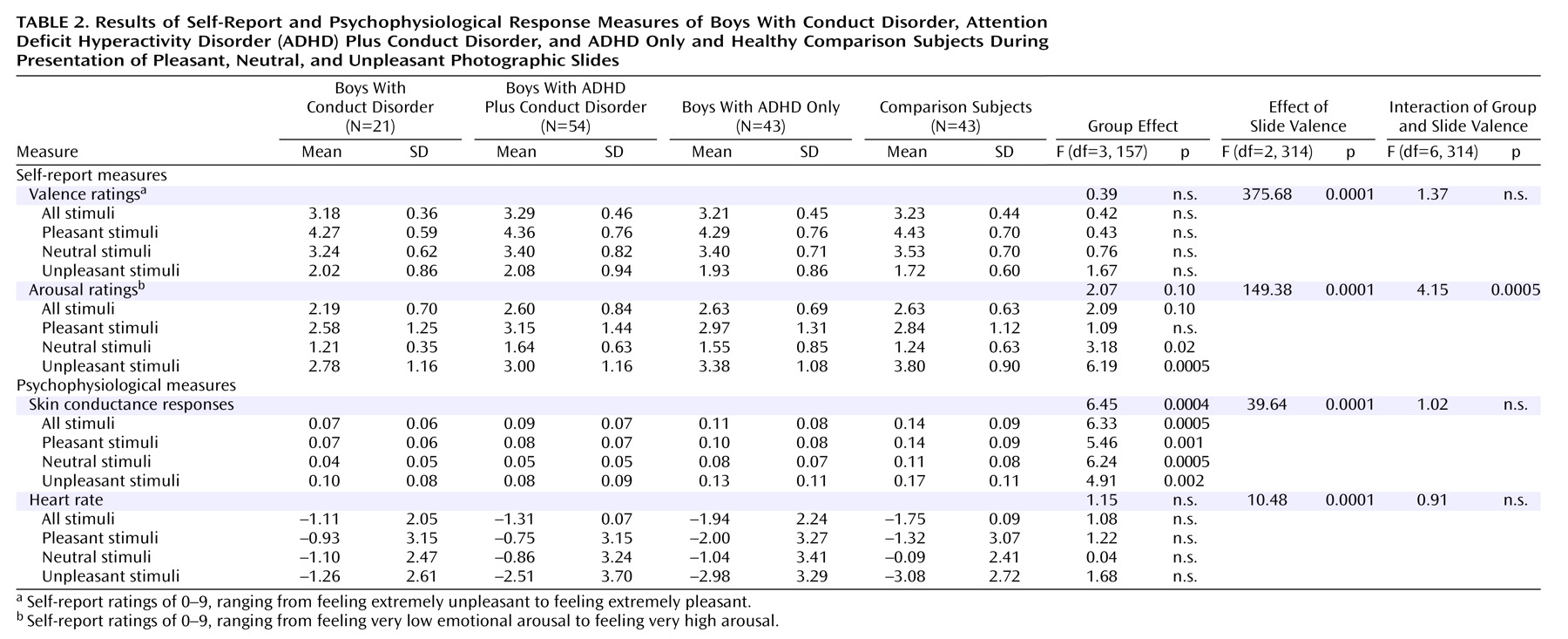
The slides selected from the International Affective Picture System were suitable for inducing various emotional ratings in 8–13-year-old boys. This finding was reflected in the repeated-measures ANOVA by the overall effect for slide valence category, which was significant for valence and arousal. For the valence ratings, neither a group effect nor an interaction effect (interaction of group and slide valence) was found (
Table 2). However, although contrasts did not show significant differences with regard to total valence ratings (F=0.03, df=1, 157, p=0.85), the combined conduct disorder and conduct disorder plus ADHD groups evaluated the negative pictures less aversively than did the combined ADHD only and healthy comparison groups, although this result did not reach significance (F=2.68, df=1, 157, p=0.10).
The overall group effect concerning arousal ratings approached significance, and there was a significant interaction of group and slide valence (
Table 2). The interaction effect was particularly produced by the ADHD plus conduct disorder group, which, relative to the healthy comparison group, gave higher ratings to the pleasant pictures and, particularly, to the neutral pictures but lower ratings to the unpleasant pictures. The ADHD only group reported a similar, but less marked, arousal pattern in response to the various slide categories. The conduct disorder group reported the lowest ratings for all slide valence categories. In a test of our specific hypothesis, contrasts showed that the combined conduct disorder and conduct disorder plus ADHD groups rated the pictures as less arousing, relative to the combined ADHD only and healthy comparison groups (F=3.66, df=1, 157, p=0.05). Considering each slide category, the combined conduct disorder and conduct disorder plus ADHD groups evaluated only negative slides as significantly less arousing (F=14.99, df=1, 157, p=0.0002); no difference was found with regard to positive stimuli (F=0.03, df=1, 157, p=0.85) and neutral stimuli (F=0.05, df=1, 157, p=0.82).
In contrast to intelligence and depressive state (measured with the Depression Inventory for Children and Adolescents), age had an influence on subjective arousal ratings for negative slides (F=3.66, df=1, p=0.05) in the covariance analysis. However, the effect of age alone is not likely to be sufficient to explain the group differences, because the overall group effect remained significant (F=5.69, df=3, 157, p=0.001).
Psychophysiological Data
An overall effect of slide valence was found, indicating that skin conductance responses were a function of slide valence category. Repeated-measures ANOVA revealed a main overall group effect but no interaction effect (
Table 2). Contrasts indicated that compared to the combined groups of ADHD boys and healthy comparison subjects, the combined groups of boys with conduct disorder only and with ADHD plus conduct disorder showed lower total electrodermal responses (F=12.81, df=1, 157, p=0.0005) as well as lower responses to each of the slide valence categories (pleasant: F=10.46, df=1, 157, p=0.001; neutral: F=15.03, df=1, 157, p=0.0002; negative: F=9.14, df=1, 157, p=0.003). Heart rate was modulated by the various slide valence categories; however, group effects were not found.
Age, intelligence, and depression were not found to be significant covariants of electrodermal response to the emotional stimuli (age: p=0.78; IQ: p=0.60; Depression Inventory for Children and Adolescents score: p=0.26).
Discussion
To our knowledge, this study is the first to assess self-report and autonomic measures of emotional responses to experimental stimuli in boys with conduct disorder. Special features of the study included the differentiation between conduct disorder boys with and without the comorbid condition of ADHD and the introduction of a clinical comparison group of ADHD children in addition to healthy comparison subjects. Our data indicate that compared to healthy comparison subjects and ADHD children, conduct disorder boys with and without comorbid ADHD reported lower levels of emotional response to aversive pictures only and showed lower intensity of autonomic responses to all categories of pictures independent of valence. In addition, our psychometric data indicate that children with the comorbid condition of ADHD plus conduct disorder are characterized by more severe behavioral disturbances than children with conduct disorder only, a finding that supports previous work by Pliszka et al.
(25).
According to the self-report data, the combined groups of conduct disorder and ADHD plus conduct disorder boys rated negative pictures as less arousing than the other two groups, and they tended to evaluate these pictures as less aversive. These findings are consistent with the theory of fearlessness in antisocial individuals of any age and may reflect an insensitivity toward potentially frightening events, which may interfere with anticipation of danger
(26). Furthermore, the two ADHD groups gave higher arousal ratings to neutral stimuli, but lower ratings to negative stimuli, compared with healthy comparison subjects, producing an interaction of group and slide valence. Conduct disorder boys reported the lowest arousal ratings throughout, indicating that children with pure conduct disorder generally experience low levels of arousal or experience indifference in response to pictures. These differential results suggest that self-ratings of emotional stimuli in children with conduct disorder are more likely to reflect real emotional experiences, compared to those of adults with personality disorder diagnoses, who do not differ in self-ratings of emotional stimuli from healthy comparison subjects and therefore appear to possess associative processing faculties that allow stimulus-appropriate evaluations
(27).
As for the findings on autonomic responses, our hypothesis that children with conduct disorder would exhibit a specific deficit in responding to affective stimuli was not supported, i.e., we failed to find an interaction of group by slide valence in the electrodermal data. Conduct disorder children with and without an additional diagnosis of ADHD showed low levels of response to aversive stimuli but also to emotional (both positive and negative) stimuli in general and to neutral pictures, as well. Therefore, the deficit in conduct disorder children that accounts for electrodermal hyporeactivity may extend beyond a failure to anticipate future punishment or reward and points to a generalized autonomic hyporesponsivity in this experimental situation.
The difference in findings between the two applied sets of measurements—self-report and autonomic responsiveness—again supports the observation of a dissociation between measures of emotional and physiological reactivity
(28) and reinforces the long recognized need in the emotion literature to examine multiple response domains. One could speculate that boys with conduct disorder with and without ADHD report low levels of arousal to negative pictures in particular because these appraisals fit their self-image of being fearless, tough, and “cool”
(29). Psychophysiological data, however, which are closer to basic information processing systems than are self-ratings, suggest that hyporesponsiveness is not restricted to a failure to identify aversive events
To guide research to identify the underlying deficit of autonomic hyporesponsivity, one hypothesis, focused on attention deficit, is that antisocial individuals are characterized by a fundamental deficit in allocating attentional resources to stimuli
(5). However, this view may be questioned, because the autonomic responses of ADHD children without coexistent conduct disorder did not differ from those of comparison subjects, even though the ADHD children had severe attentional deficits. Alternatively, decreased autonomic responses in the conduct disorder and ADHD plus conduct disorder children may reflect the way children process complex stimuli that may signal an emotionally potent event. Our results support the findings of Schmidt et al.
(30), who reported low levels of response to nonemotional tones in undersocialized aggressive children, and they are consistent with data previously obtained by our research group in an analogous study design in which adults with psychopathy exhibited a generalized deficit in electrodermal responsivity
(31). Therefore, the general autonomic hyporeactivity we found in the conduct disorder children with and without ADHD may reflect a deficit in associative processing systems that respond to complex cueing contexts, as was found by Patrick and Lang
(32) in their study of adult antisocial individuals.
Autonomic hyporesponsiveness appears to be a highly reliable correlate of childhood conduct disorder and adult psychopathy; however, the underlying deficit is far from clear. Some methodical limitations need to be considered, as well, concerning demographic and clinical characteristics of our cohort. As in other studies
(33), the comparison subjects had a higher IQ than the clinical groups, although this difference had no influence on group effects in psychophysiological data. The boys with conduct disorder only were older than the boys in the other groups, and this age difference was significant in the comparison between the conduct disorder only and ADHD only groups. However, the age distribution was typical of child psychiatric samples. The broad majority of children under the age of 12 who meet the criteria for conduct disorder also meet the criteria for ADHD
(34). Again, covariance analyses indicated that psychophysiological data were not confounded by differences in age. In addition, the group sizes were quite heterogeneous because of the selection bias associated with a clinical population in which conduct disorder comorbid with ADHD is more likely to occur than is pure conduct disorder. Klein et al.
(35), who sought to find a group of children with pure conduct disorder for a research study, discovered that 69% of the conduct disorder group concurrently had ADHD.
In summary, our data indicate that conduct disorder children with and without ADHD, but not children with ADHD only, are characterized by a response deficit when exposed to complex visual stimuli of unpredictable affective quality.