Suicide is an important public health problem
(1). The method of suicide does not appear to be randomly distributed. For example, violent method of suicide is more often used by males than females
(2–
4), and violent method is more common in suicide completers affected by psychosis
(5). On the other hand, the relationship between violent method and age remains unclear
(4–
7). Since the early work of Åsberg
(8), suicide method has been used in neurobiological studies of suicide attempters to select subjects who are more likely to have low indexes of serotonergic neurotransmission, which in turn tend to correlate with higher levels of aggression
(9). However, the relationship between use of violent method and history of aggressive behavior remains inconclusive
(10,
11). Moreover, it has not been investigated in suicide completers. Therefore, the main purpose of this study was to investigate clinical and behavioral correlates of violent method of suicide and to assess whether it represents a behavioral marker of lifetime aggressive behavior.
Method
Subjects for this study were individuals who had committed suicide identified through the Coroner’s Office and collected sequentially from the Greater Montreal area. Seventy-three percent of the families of these individuals agreed to participate in our clinical study. After a period averaging 4 months, these families were contacted again for interviews. This study was approved by our local institutional review board, and written informed consent was obtained from all participating families.
Suicides were classified on the basis of information provided by the Coroner according to criteria used in previous studies
(2,
5,
12). Overdoses, poisoning, gas, and drowning were classified as nonviolent methods of suicide; all other methods were classified as violent.
Psychiatric diagnoses in individuals who committed suicide were made by means of the psychological autopsy method. This technique has been well validated and is outlined elsewhere
(13–
15). Psychiatric diagnoses were obtained by using the Structured Clinical Interview (SCID)
(16) for DSM-IV axis I diagnoses and axis II personality disorders. Before applying the SCID, we used the Schedule for Affective Disorders and Schizophrenia for School-Age Children
(17) modified to include questions assessing personality disorders adapted from the Children’s Depression Inventory
(18). As reported elsewhere
(19), diagnoses obtained using these two different methods had an excellent concordance rate. Information collected with these interviews, from the Coroner’s notes, and from medical records was used by a panel of clinicians who made consensus DSM-IV diagnoses.
Two or more interviewers were asked to rate the same subject separately, and kappa coefficients for key diagnoses were excellent: kappa=0.96 for major depression, kappa=0.98 for alcohol abuse/dependence, kappa=1.0 for drug abuse/dependence, kappa=1.0 for bipolar disorder, kappa=1.0 for schizophrenia, and kappa=1.0 for cluster B personality disorders. These data are consistent with those previously presented by our group
(20) and probably are a direct result of frequent training sessions to avoid drifting between interviewers.
The Brown-Goodwin Lifetime History of Aggression
(21) and the Barratt Impulsivity Scale
(22) were used to assess lifetime aggressive and impulsive behaviors, respectively. The Temperament and Character Inventory
(23) was used to complement this information. Internal consistency estimates were excellent overall: alpha=0.88 for the informant version of the Brown-Goodwin Lifetime History of Aggression, alpha=0.89 for the Barratt Impulsivity Scale, and alpha between 0.73 and 0.88 for the Temperament and Character Inventory.
In addition, we compared information obtained using two different informants for the same deceased individual for personality trait measures and observed no significant differences (p values between 0.25 and 0.94). Furthermore, in studies with living subjects we compared information obtained with an informant and the subject and found no significant differences (p values between 0.67 and 0.98).
Chi-square, odds ratios, and Fisher’s exact tests were used to compare categorical variables, and t tests were used in the analysis of continuous variables. Logistic regression was used to obtain adjusted risks.
Results
A total of 310 individuals who had committed suicide were investigated: 36 female subjects and 274 male subjects with a mean age of 39.45 years (SD=13.91). Two hundred forty-two (78.1%) of these individuals used a violent method: 166 (68.6%) hanged themselves, 39 (16.1%) used a firearm, 12 (5.0%) used laceration, 18 (7.4%) jumped from a height, and seven (2.9%) used one of the following: traffic accident, electrocution, self-immolation, or strangulation with a plastic bag. On the other hand, 68 (21.9%) of the individuals who committed suicide used nonviolent methods. Of these, 36 (52.9%) died intoxicated by gases, 22 (32.4%) by drug poisoning, and 10 (14.7%) by drowning. This distribution of suicide methods is consistent with that reported for all suicide cases by the Quebec Coroner’s Office in 2000. The average age was lower in the violent method group (38.20 compared with 43.96 years) (t=2.54, df=305, p<0.02), and female subjects showed a tendency to use a nonviolent method (χ2=3.09, df=1, p<0.08).
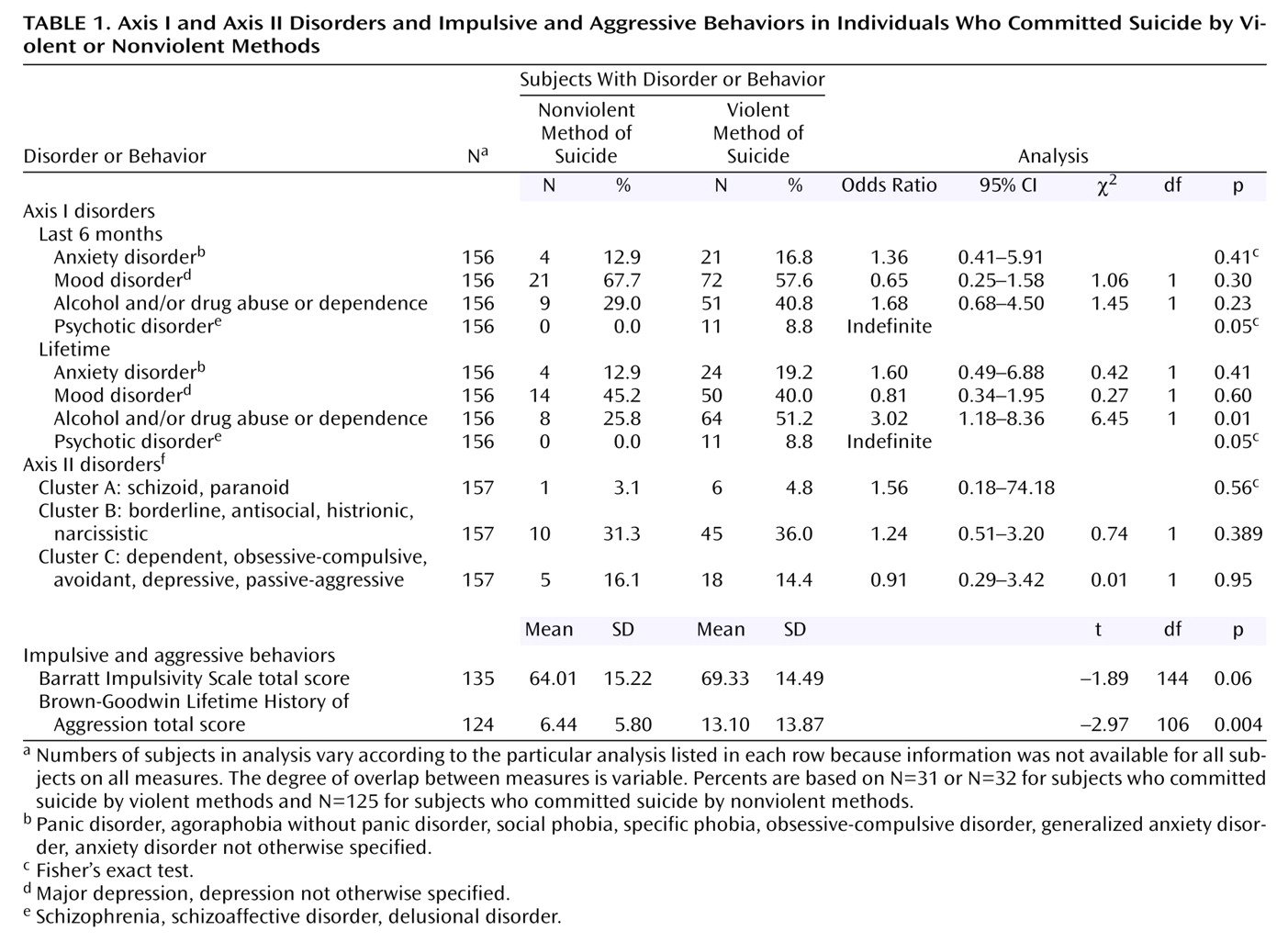
Last-6-month prevalence rates of anxiety disorders, mood disorders, and alcohol and/or drug problems (abuse/dependence) were comparable between groups. Similarly, lifetime prevalence rates of anxiety disorders and mood disorders were comparable between groups, as were the prevalence rates of cluster A, cluster B, and cluster C personality disorders. In contrast, prevalence rates of lifetime alcohol and/or drug problems and psychotic disorders (6-month and lifetime) were significantly associated with violent method of suicide (
Table 1).
Measures of lifetime history of aggressive behaviors were higher in the group that used a violent method of suicide. In addition, we found a nonsignificantly higher level of impulsive behaviors as measured by the Barratt Impulsivity Scale in the violent method group. Aggressive and impulsive behavior scores were also found to be significantly correlated (r=0.45, N=124, p<0.001). On the other hand, Temperament and Character Inventory measures were not statistically different between groups (data not shown). Finally, when we controlled for the effect of age, sex, substance disorders, and psychopathology (major psychiatric axis I disorders as a categorical variable), we found that history of lifetime aggression (p=0.03) and the interaction between lifetime aggression and lifetime impulsivity (p<0.06) remained associated with a violent method of suicide.
Discussion
To our knowledge, this study is the first to investigate the relationship between measures of aggression, impulsivity, and suicide method in individuals who committed suicide. Overall, our analysis supports the use of suicide method as a possible behavioral marker of lifetime impulsive aggression.
We found that younger age was associated with violent method and observed a nonsignificant gender effect. The effect of gender is consistent with previous findings
(2,
4,
6), and its nonsignificance may be a consequence of the relatively small number of female subjects included in this study. Although suicide cases in this study were obtained sequentially, our group has been focusing on male suicide and only more recently has started recruiting females. The age effects found in this study support the finding by Conwell et al.
(7) that older individuals who commit suicide are more likely to use nonviolent methods. Finally, we observed that lifetime alcohol and/or drug problems and psychotic disorders were associated with use of violent methods. In addition, significant correlations between lifetime history of substance misuse and impulsive behavior (r=0.41, N=135, p=0.001) and aggression (r=0.32, N=124, p=0.004) were found. These findings are consistent with those of previous studies
(24,
25) suggesting that there is probably a relationship between chronic alcohol and/or drug consumption and lifetime aggression and violence. Nevertheless, when we controlled for the history of substance use, as well as for other positive variables, we found that higher levels of impulsive and aggressive behavior and their interaction remained significant predictors of violent methods of suicide.
Given that the lethality associated with violent methods is considerably higher than that associated with nonviolent methods
(26), a possible hypothesis that could be drawn from our results is that the observed excess of impulsive-aggressive behavior among individuals who committed suicide may be a direct consequence of the fact that these individuals were more likely to use a violent method. This hypothesis is supported by recent data suggesting that differences in method explain a substantial amount of the difference between completed suicide and medically serious nonfatal suicide attempts
(27).
The major limitation of this study is intrinsic to the psychological autopsy method. However, our results on validity are consistent with the literature
(13–
15) and support the use of behavioral assessments obtained by means of informants. Other limitations in our analyses include the infrequency of diagnoses such as psychotic disorders.
In conclusion, our results suggest that violent method of suicide could be a valid behavioral marker of lifetime impulsive aggression. This relationship is probably mediated by several other factors that this study did not aim to assess and that remain to be investigated further. Additional research including suicide attempters with a larger number of female subjects who committed suicide and more individuals who committed suicide by nonviolent methods is needed to confirm and further understand the relationship between impulsive-aggressive behaviors, suicide method, and suicide outcome.