Approximately one in 10 women is depressed during any trimester of pregnancy or any month within the first year after delivery
(1) . The consequences of depression can be devastating, inhibiting the woman’s ability to perform daily activities, to bond with her infant, and to relate to the infant’s father
(2 –
5) . Previous studies have found that any history of depression is one of the greatest risk factors for postpartum depression
(6), and studies that have followed women during pregnancy and throughout the postpartum period have found that approximately 50% of women with depression after delivery had depression during pregnancy
(7 –
9) . However, little is known about women’s depression status immediately before pregnancy and how that status relates to the trajectory of depression during and after pregnancy.
Pregnancy poses a unique challenge for the ongoing treatment of depression. For women with preexisting depression, pregnancy may interrupt the continuity of care from one health care provider before pregnancy to another during pregnancy. Moreover, consideration of medication use while trying to get pregnant or during pregnancy requires that the potential risks of antidepressant medication on fetal development be weighed against the severity of illness for the mother. Although there has been no evidence of major congenital malformations due to antidepressant exposure in the published literature
(10), recently concerns have been raised about first-trimester exposure to paroxetine and the increased risk for cardiovascular malformations (http://www.fda.gov/cder/drug/advisory/paroxetine200512.htm). In addition, second- and third-trimester exposure to all types of selective serotonin reuptake inhibitors (SSRIs) has been associated with an increased risk of persistent pulmonary hypertension in the newborn
(11) . Questions on safety associated with the long-term behavioral or neurological effect of prenatal exposure to antidepressants have not been fully examined. In the last several decades, antidepressant use has increased in the United States overall, although the trend among pregnant women in unknown. In light of these newly identified risks for the fetus and the overall increase in antidepressant use in the United States, monitoring the prevalence of women with depression and their antidepressant use before, during, and after pregnancy is of particular interest.
We examined the prevalence of diagnosed maternal depression and treatment, including antidepressant use, received any time during the 39 weeks before pregnancy, any time during pregnancy, and any time during the 39 weeks after pregnancy. To explore issues around continuity of care, we tracked the clinical department of the provider where depression was first identified in the medical records during the study period.
Method
We analyzed data from Kaiser Permanente Northwest (KPNW), a large nonprofit, prepaid, federally certified, accredited by the Joint Commission on Accreditation of Healthcare Organizations, group practice health maintenance organization (HMO) with 456,000 members in western Oregon and Washington state (as of 2004). Members included individuals covered by commercial and individual self-pay health plans, Washington State Basic Health Plan (subsidized), Medicare, and Medicaid. The HMO’s enrollment was demographically representative of the local community, and enrollees accounted for approximately 16% of the live births in the KPNW service area. The age distribution of KPNW enrollees delivering live births was similar to that of women delivering in the community.
To identify pregnancies, we used a complex validated computer algorithm that accessed multiple KPNW-automated data systems and searched for prespecified indicators of pregnancy
(12) . We found 100% agreement on live birth outcome among episodes identified by the algorithm and those reviewed by medical records. The data systems included the following: administrative systems that track time and type of patient membership; claims and financial data; encounter data sets that document all patient contacts for services; and the online medical records system (computerized patient records) used for inpatient care, from which selected variables are coded and extracted into a data set available for research and internal strategic planning purposes. The data available for our use included 1) hospital discharge abstracts; 2) diagnostic and procedure codes from same-day surgery records, ambulatory encounters, and emergency department and home health visits; 3) outside professional and facility claims and referrals; 4) imaging procedures; 5) laboratory test results; and 6) pharmacy dispensing records. After pregnancies were identified, live birth certificates were matched by using a probabilistic method to the KPNW births to gather additional demographic information such as the education and race/ethnicity of the mother. The probabilistic method involved a scored matching system based on the mother’s name (maiden and married), date of birth, social security number, and address and the infant’s name, date of birth, and facility of delivery/birth. A cutoff point was determined, and scores above the cutoff point indicated a match between KPNW and birth certificate data. For this study, 98.4% of live births were matched to a live birth certificate. This study was approved by the Centers for Disease Control and the KPNW institutional review boards.
We selected all pregnancies ending in live births between Jan. 1, 1998, and Dec. 31, 2001, and where the mother was enrolled in KPNW 39 weeks before the pregnancy, during the pregnancy, and 39 weeks after the pregnancy. We chose 39 weeks before and after the pregnancy because 39 weeks was the mean gestational time period, and therefore, on average, the length of time would be the same for all three periods. We chose only pregnancies in which the woman was enrolled continuously during that period or with an interruption of no more than 12 weeks. Short eligibility interruptions typically result from administrative errors in processing a request for change in enrollment to accommodate divorces, adoptions, marriages, and benefit option changes. We chose the first pregnancy ending in a live birth for women with more than one pregnancy during the study period.
Depression was identified either by an ICD-9-CM diagnosis (296.2, 296.20–296.25, 296.3, 296.30–296.35, 296.82, 300.4, 309.0, 309.1, 309.28, or 311) or an antidepressant medication dispensed within 30 days of the ICD-9-CM diagnosis code 648.4, which is for “Mental Disorders Specific to Pregnancy.” Initially, we considered any use of an antidepressant as a possible diagnosis, but after review of the medical records, we found many of these women were being treated with antidepressants for indications other than depression (unpublished study by Williams et al.). The exception was women who had the ICD-9-CM diagnosis code 648.4. Antidepressant medications included tricyclics (amitriptyline, clomipramine, desipramine, doxepin, imipramine, and nortriptyline), SSRIs (fluoxetine, fluvoxamine, paroxetine, sertraline, citalopram, and escitalopram), monoamine oxidase inhibitors (tranylcypromine, phenelzine, selegiline, and isocarboxazid), heterocyclic antidepressants (e.g., nefazodone and trazodone), and others (bupropion, venlafaxine, and mirtazapine). Treatment for depression was defined as receiving at least one dispensing of antidepressant medication identified through pharmacy records or at least one mental health visit identified through electronic medical records with a depression or dysthymia diagnosis.
The patterns of depression were examined for associations with a variety of demographic and behavioral characteristics of the mother, diagnoses for anxiety, and the specialty of the provider who made the first diagnosis during the study period. The birth certificate provided information on the mother’s highest level of educational attainment, tobacco use during pregnancy (if missing from KPNW data), parity, marital status, race, ethnicity, and trimester of entry into prenatal care. KPNW data provided the specialty department in which the first diagnosis of pregnancy was made (e.g., internal medicine, obstetrics, or family practice), tobacco use during pregnancy, parity (if missing from the birth certificate), race, ethnicity (if missing from the birth certificate), and a diagnosis code for anxiety (ICD-9-CM codes 300.02, 300.00, 300.01, 300.21, 300.23, 300.2, 300.22, 300.29, 300.3, 309.21, 300.7, 300.81, 308.2, 308.3, 308.9A, or 309.81).
One study eligibility criterion required women to be enrolled in KPNW 39 weeks before through 39 weeks after delivery. Because we were concerned that women at higher risk of diagnoses of depression were more likely to be excluded, we compared the women who met the study enrollment criteria to those who did not (but had delivered a live birth during the study period) by maternal characteristics and depression status during pregnancy using the chi-square test of independence.
We examined the prevalence of depression and treatment before, during, and after pregnancy and tested for statistical differences with the generalized linear model with repeated measures because the same group of women was assessed in all three time periods. We also examined the association of depression diagnoses with maternal demographic and behavioral characteristics. Multiple variable logistic regression was used to assess the independent associations of the maternal characteristics with the mother’s depression. Initially, we used three models, one for depression diagnosis before pregnancy, one for during, and one for diagnosis after pregnancy, and found no differences in risk factors among the three time periods. Therefore, we report one model that compares women with a depression diagnosis at any time during the study period to those without a diagnosis.
Results
The majority of women in the study were white (79%), were between 20 and 34 years of age (73%), had at least 13 years of education (53%), and were married (76%). Compared with women eligible for the study, women who were ineligible because of enrollment requirements were statistically (p<0.05) less likely to be ≥35 years of age (11% versus 17%) and had fewer years of education (16% had <12 years of education versus 10%). They were more likely to be Hispanic (10% versus 7%), unmarried (31% versus 22%) and Medicaid recipients (32% versus 13%) and to have smoked during pregnancy (16% versus 12%). There was no significant difference between women eligible and ineligible for the study for any of the depression indicators during pregnancy: any depression diagnosis, major depression diagnoses, and antidepressant medication dispensed.
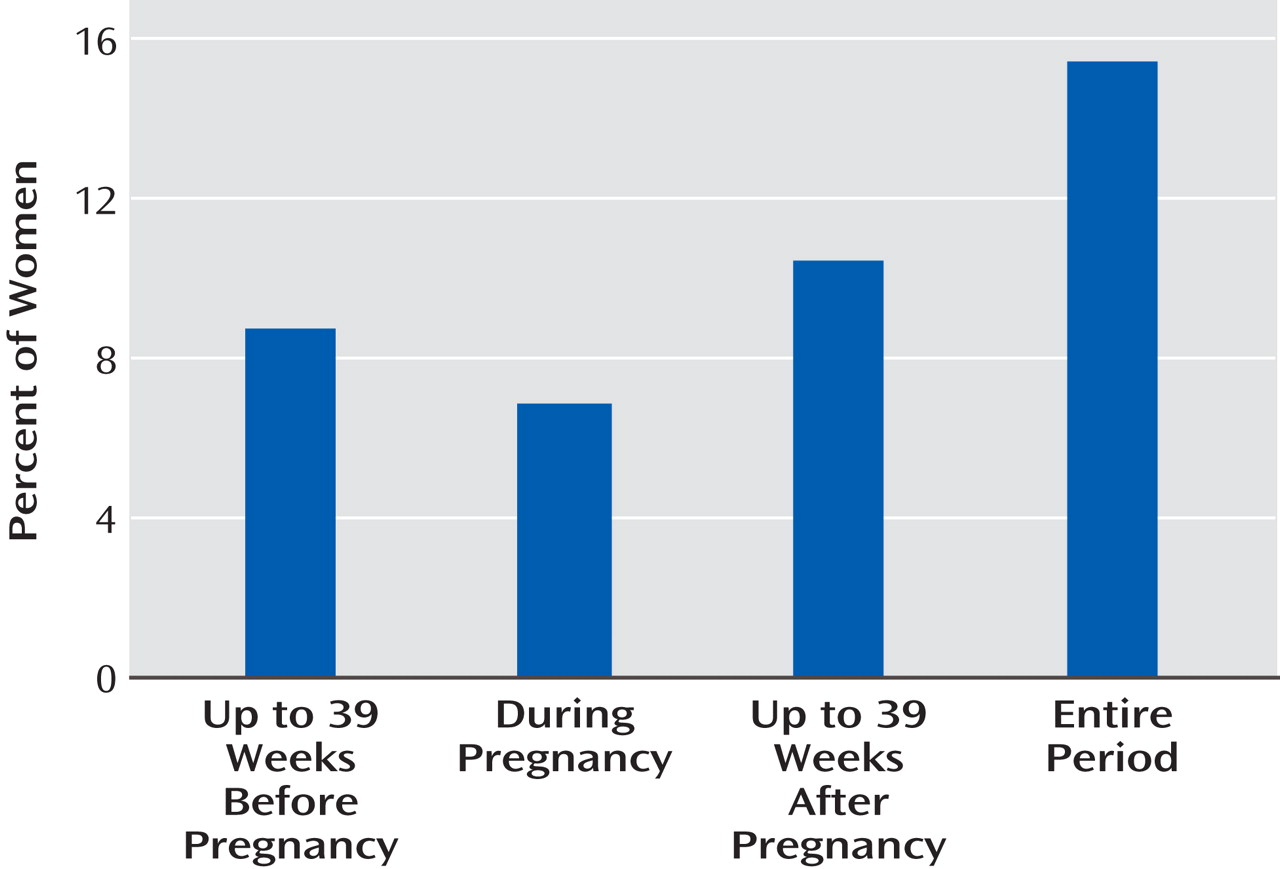
Among 4,398 women with eligible pregnancies, 678 (15.4%) were identified with depression during at least one period; 8.7%, 6.9%, and 10.4% had depression diagnoses before, during, and/or after pregnancy, respectively (
Figure 1 ). These prevalences were statistically significantly different from each other (p<0.05). Of women with identified depression, 17.5% also had a diagnosis of anxiety. This was the only comorbidity examined. Many women had more than one ICD-9 code for depression, with an average number of 1.4 types of depression diagnoses per woman: 71.2% of the women were diagnosed with depression disorder not otherwise specified, 25.2% with adjustment disorder with depressed mood, 20.6% with major depression, 11.8% with mental disorders specific to pregnancy, and 9.4% with dysthymic disorder. Of women with identified depression during the 39 weeks before pregnancy, 56.4% were also identified with depression during pregnancy. Of women with depression diagnoses in the postpartum period, 54.2% were also identified as depressed either before or during pregnancy.
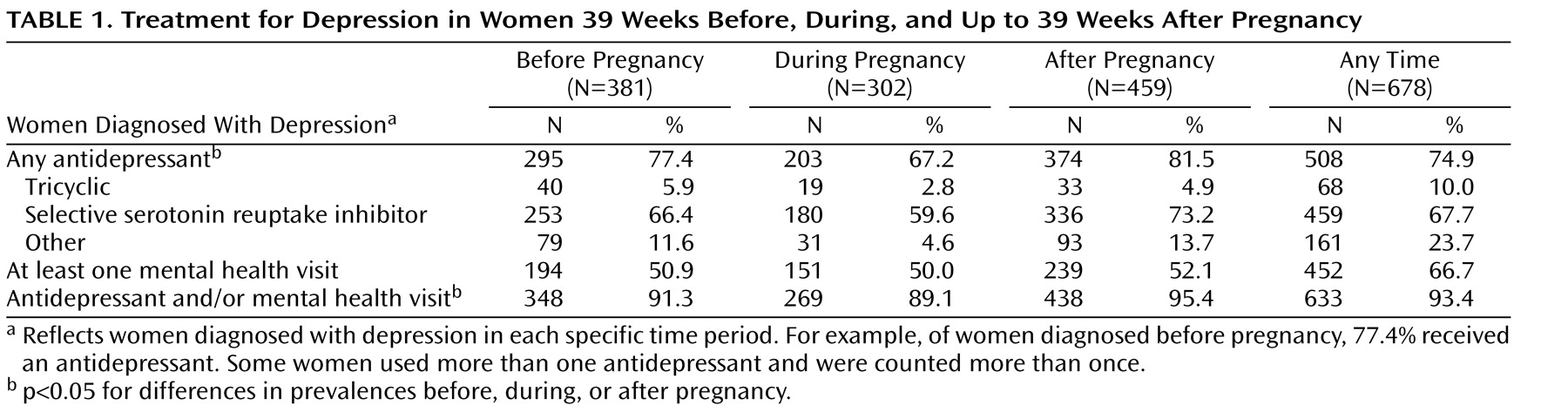
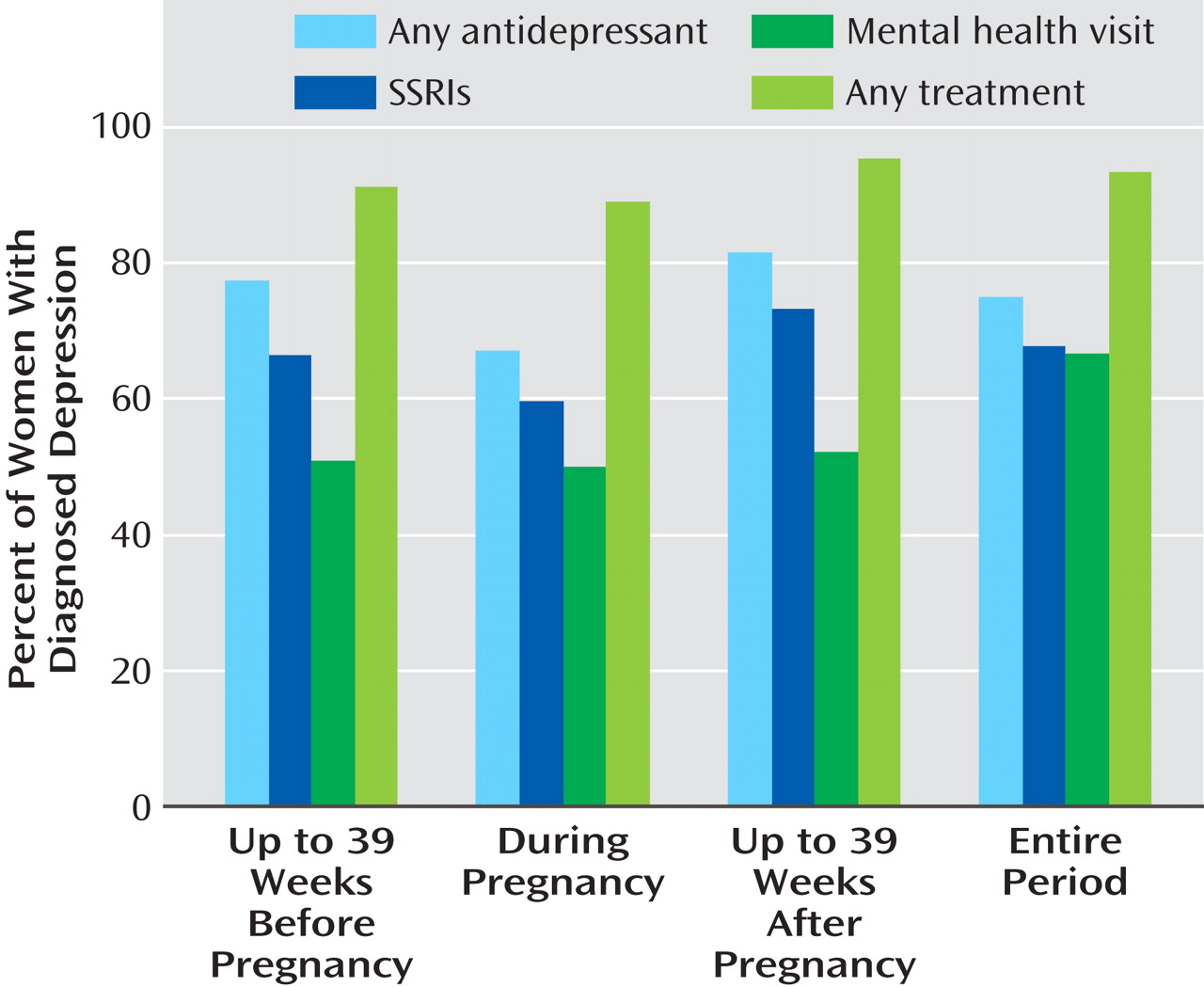
Of those identified with depression at any time during the study, 66.7% visited a mental health specialist at least once, and 74.9% received an antidepressant, with a total of 93.4% having at least one of these treatments for depression (
Table 1,
Figure 2 ). Statistically fewer (p<0.05) prescriptions were filled for antidepressants during pregnancy (67.2% of the women identified as depressed during pregnancy) than before (77.4%) or after pregnancy (81.5%). SSRIs were the most common type of antidepressant dispensed, and 180 women (4% of all pregnant women) received them during pregnancy. The percent of women with identified depression who used mental health visits as a form of treatment did not vary before, during, or after pregnancy.
During the entire study period, most depression was first identified by a primary care provider (41.3%), followed by a mental health provider (30.7%) and an obstetrics and gynecology provider (13.0).
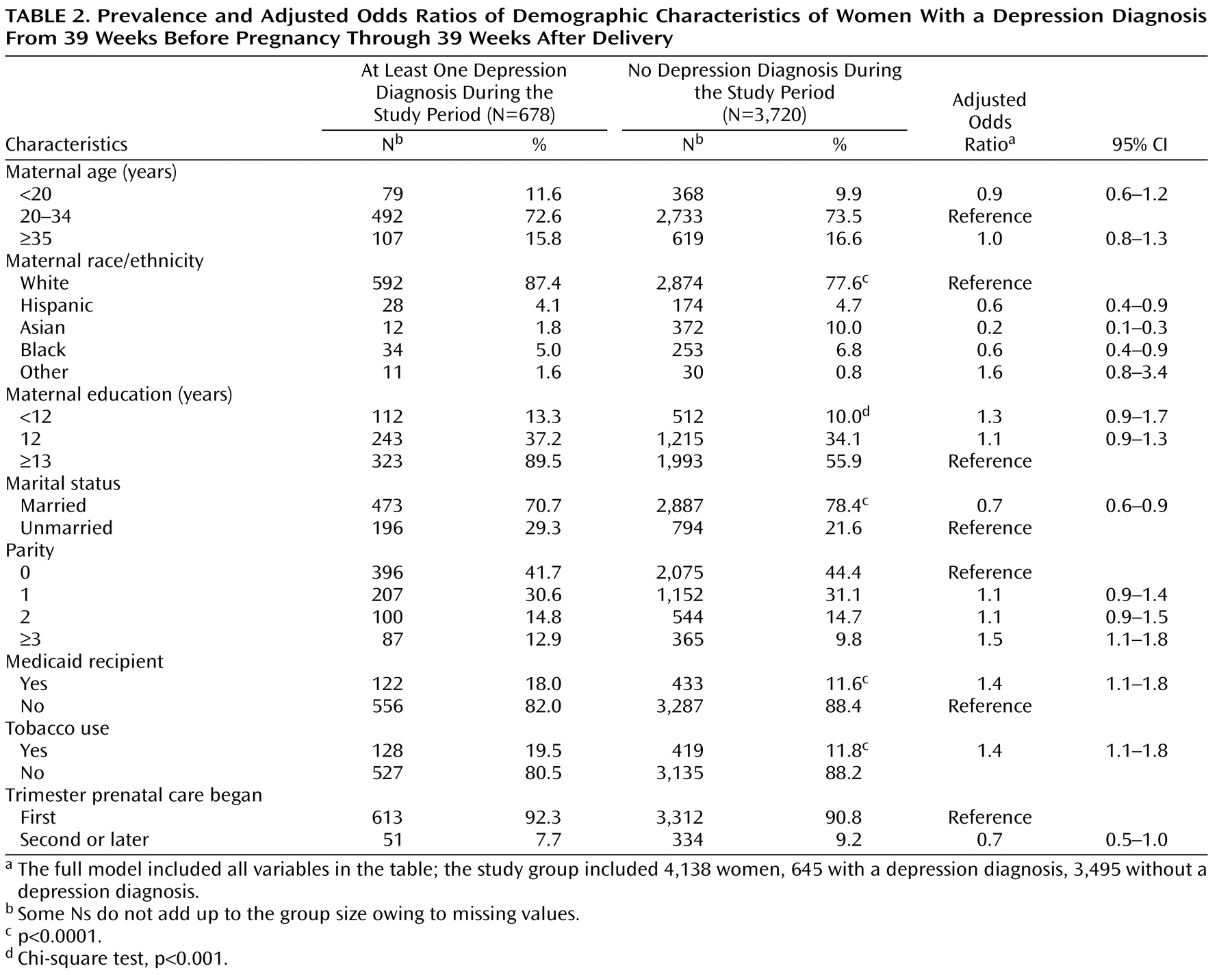
Women most likely to be identified as depressed at any time 39 weeks before through 39 weeks after the pregnancy were white, were unmarried, had three or more children before this pregnancy, smoked cigarettes during pregnancy, and had health coverage through Medicaid (
Table 2 ). Age, education, and trimester of entry into prenatal care were not associated with clinically identified depression.
Discussion
Women of childbearing age are at high risk for major depression
(13 –
15) . Pregnancy and new motherhood may increase the risk of depressive episodes
(16) . A recent evidence review sponsored by the Agency for Healthcare Research and Quality found that the point prevalence of depression ranged from 8.5% to 11.0% at different times during pregnancy and from 6.5% to 12.9% at different times during the first year postpartum
(17) . Our study found that the proportion of women with clinically identified depression was slightly higher during the postpartum period (10.4%) than before pregnancy (8.7%) or during pregnancy (6.9%), reinforcing the findings of the Agency for Healthcare Research and Quality evidence report on perinatal depression
(17) . The slightly higher prevalence postpartum may reflect the added stress of caring for a newborn. For some women, the events and circumstances of labor, delivery, and the postpartum represent a unique and even traumatic stress that may precipitate the first symptoms of depression. Alternatively, the increased prevalence postpartum could reflect detection differences in that clinicians may be more likely to identify and treat depression before pregnancy and in the postpartum than during pregnancy. Unique to this study was the identification of depression diagnoses in the period 39 weeks before pregnancy. Approximately 9% of the women had a diagnosis of depression in this time period, 77% of whom were dispensed an antidepressant and 56.4% of whom went on to have a depression diagnosis during pregnancy. Some of these women may have been faced with decisions regarding continuity of antidepressant use while trying to conceive and during the pregnancy. During pregnancy, some of these women also needed to decide which provider would be best to provide the continued care for their depression. Because they encounter multiple specialists in their reproductive years, women with chronic conditions such as depression pose unique challenges for continuity of care.
The use of antidepressants was the most common form of treatment and was found to be lower during pregnancy than before or after. Surprisingly, there was no evidence that mental health visits were used as an alternative to medications because the percentage of women using this form of treatment was not higher during pregnancy. Two-thirds of the women identified as depressed during pregnancy were dispensed antidepressants, the majority of which were SSRIs. Ongoing monitoring of SSRI use during and after pregnancy is warranted, given the associations with cardiovascular malformations and persistent pulmonary hypertension of the newborn and the lack of information on the long-term neurological and behavioral effects on the newborn
(11) . Although we found that 4% of all pregnant women were dispensed an SSRI in our study, these data were collected before the concerns were publicized regarding persistent pulmonary hypertension of the newborn and cardiovascular malformations, and it is possible that these recent findings of potential harm to the fetus may affect current SSRI use during pregnancy. The potential risks of SSRIs must be balanced against the risk of relapse of depression, particularly for women with well-controlled symptoms before pregnancy, because women who maintain their antidepressant medications throughout pregnancy are less likely to relapse compared with women who discontinue their medication
(13) .
Consistent with other studies, approximately 50% of the women diagnosed with depression postpartum were also diagnosed in an earlier phase of the study
(7 –
9) . This suggests that previous depression should be part of the medical history for pregnant and postpartum women. In addition, because approximately 50% of the women were identified as depressed during only one time period (39 weeks before, during, or 39 weeks after the pregnancy), clinicians may need to be aware of the potential for depression in all of their patients, and screening of all pregnant and postpartum women may be warranted. We recommend more research on two-part screening, a simple screening question and clinical impressions applied to all pregnant women, and then follow-up with a more structured depression scale and clinical interview for women screening positive for depression and dysthymia at the first screen. Although Gaynes et al.
(17) did not find strong evidence to support the hypothesis that the prevalence of depression is higher during pregnancy or in the first year postpartum compared to nonchildbearing times, they nevertheless suggested that pregnancy and the early postpartum period provide natural opportunities to screen for and treat depressive symptoms through regular prenatal obstetrical care and postpartum pediatric care.
Consistent with the literature, the demographic characteristics associated with clinically identified depression included women with fewer economic resources (Medicaid recipients) or with less social support (unmarried)
(2,
6,
9,
18 –
20) . These women may be experiencing more stress in their lives than women with more economic resources or social support, and stress has been found to trigger some depression episodes
(21) . We found that white women were more likely to be identified with depression than black and Asian women, but it is unclear if this reflects a true difference in prevalence or in detection and treatment. At least one study found that black and Hispanic patients with depression were less likely to be diagnosed than white patients, other things being the same
(22), and a study of impoverished, inner-city pregnant and postpartum women found that the rates of depression did not differ between black and white women
(19) . Women who smoked during pregnancy had a higher prevalence of depression, which may suggest special challenges for smoking cessation approaches for these women during and after pregnancy. Taken together, none of the maternal risk factors for depression (besides a history of depression) were strong enough to support focusing only on a high-risk-demographic approach to pregnancy-related depression identification.
The purpose of this study was not to estimate all depression, diagnosed and undiagnosed, but to better understand the prevalence of diagnosed and treated depression before, during, and after pregnancy. As such, this study was limited to clinically identified cases of depression and likely underestimates the “true” prevalence of depression in this population
(23,
24) . The importance of previous history may be understated in this study because we only examined it within 39 weeks before the pregnancy. Our study design required that women be enrolled 39 weeks before and after delivery. As such, the women covered by Medicaid were more likely to be excluded from the study group because their coverage ended 60 days after delivery. These women also were more likely to be diagnosed with depression. Thus, our study findings were limited to women with stable insurance coverage and who were potentially less likely to be at risk for depression. Another limitation of this study was our reliance on ICD-9-CM diagnosis codes, which are subject to inaccuracies, and because our study was based largely on administrative data, we were not able to assess the degree to which depression was controlled by therapy, nor could we distinguish mental health visits used to prescribe antidepressants from those that solely provided counseling. Moreover, the women received a code for depression diagnosis based on the clinical impression of the providers, and the retrospective nature of these data did not allow us to specify the criteria for ascribing the diagnosis. Still, this cross-sectional view reflects the reality of this clinical setting.
Approximately one in seven women was identified with and treated for depression during the 39 weeks before through the 39 weeks after pregnancy, and more than half of these women had recurring indicators for depression over the period. The high level of treatment among women identified with depression (93.4% overall) suggests that women are willing to obtain treatment if identified with depression. The acceptability of treatment does support routine screening for depression, which could uncover undetected depression and, with appropriate treatment, mitigate the devastating effects of this disease on the mother, infant, and other siblings. Depression is an illness that affects a substantial proportion of women around the time of pregnancy, and antidepressant use was the most common approach to treatment. Continuity of care and balancing the treatment needs of women and the risk of harm to the fetus are the challenges of treating women during this period.